Treatment for sle
Reading File
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND "therapy"[MeSH Terms]
Finding Sources
Searching PubMed
"lupus erythematosus, systemic"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have a thorough foundation. Let me compile the full answer.
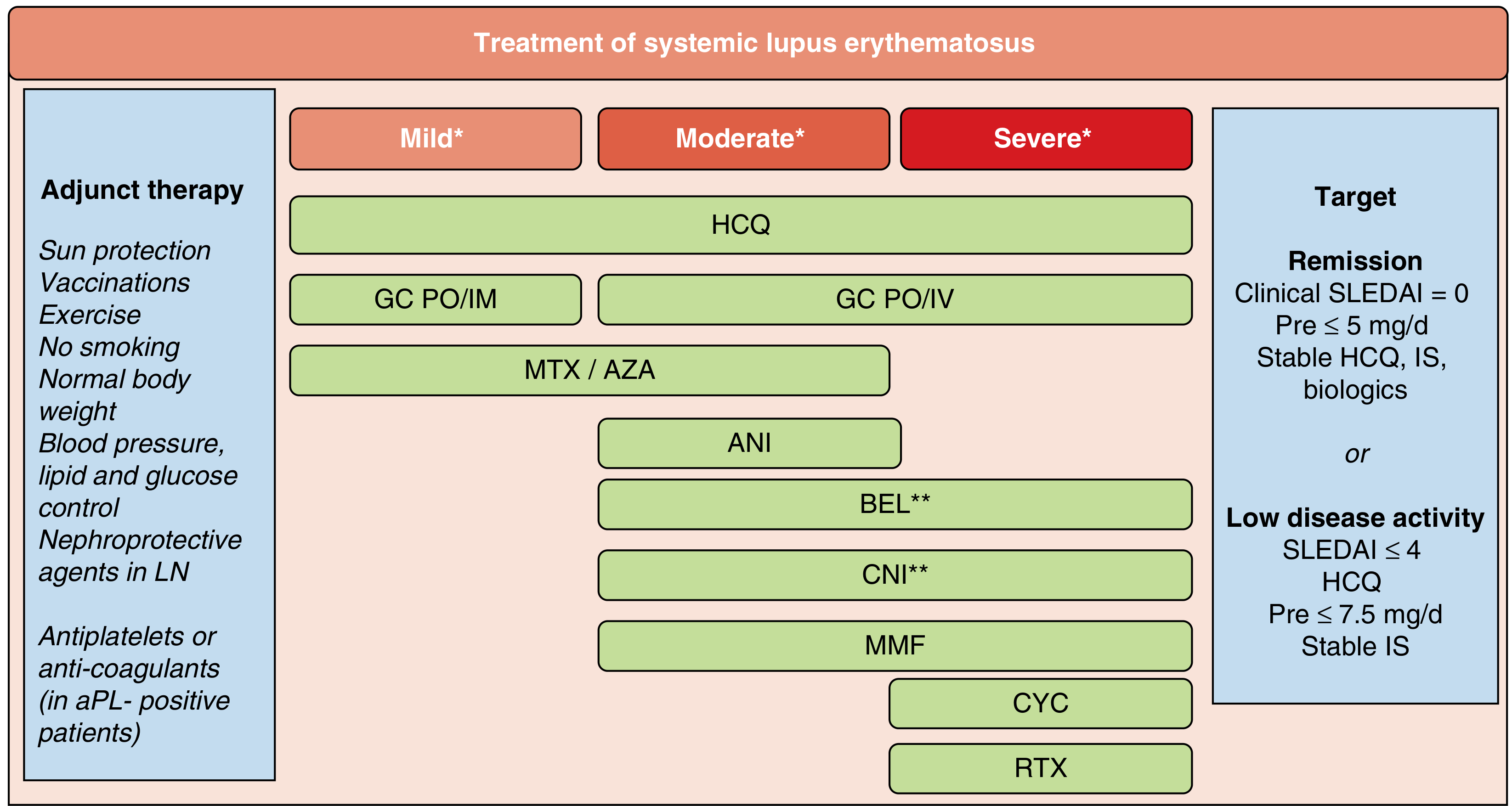
Treatment of Systemic Lupus Erythematosus (SLE)
SLE follows a relapsing-remitting course and requires a treatment strategy tailored to disease severity and organ involvement. The overarching goals are achieving remission or low disease activity (SLEDAI ≤ 4), minimizing glucocorticoid (GC) toxicity, and preventing irreversible organ damage.
Treatment Flowchart
1. Hydroxychloroquine (HCQ) - Universal Backbone
Recommended for ALL SLE patients who do not have contraindications.
- Dose: Must not exceed 5 mg/kg real body weight/day (to minimize retinal toxicity)
- Ophthalmologic screening: At baseline, 5 years after starting, then annually
- Benefits: Controls skin disease, arthritis, serositis, and mild hematologic abnormalities; reduces risk of flares, end-stage renal disease, type 2 diabetes, venous thromboembolism, and cardiovascular events; improves overall SLE survival
- Mechanism: Reduces lysosomal activity, inhibits MHC class II antigen presentation, and blocks TLR7/TLR9 signaling
- Safety in pregnancy: Not teratogenic; continued during pregnancy to prevent flares
2. Mild SLE (Skin, Joints, Mucosal)
| Agent | Role |
|---|---|
| HCQ (antimalarial) | First-line; backbone |
| NSAIDs | Symptomatic relief for arthritis/serositis |
| Low-dose oral GCs (prednisone ≤ 7.5 mg/day) | Short-term control |
| Methotrexate (MTX) | Skin and joint disease, steroid-sparing |
| Azathioprine (AZA) | Steroid-sparing DMARD |
3. Moderate-to-Severe SLE
Glucocorticoids
- Oral or IV GCs are used for rapid disease control
- Goal: Taper to prednisone ≤ 5 mg/day (remission target) or ≤ 7.5 mg/day (low disease activity target)
- High-dose IV methylprednisolone "pulse" therapy (500-1000 mg/day x 3 days) for severe flares
Immunosuppressants
- Mycophenolate mofetil (MMF): 2-3 g/day; first-line for lupus nephritis (LN) and extrarenal moderate-severe SLE; comparable or superior to cyclophosphamide with better tolerability; strongly teratogenic
- Azathioprine (AZA): 2-3 mg/kg/day; used in mild-moderate disease and as maintenance; safe in pregnancy (unlike MMF)
- Methotrexate (MTX): Useful for musculoskeletal and mucocutaneous manifestations
4. Severe/Organ-Threatening SLE - Cyclophosphamide (CYC)
Used for proliferative lupus nephritis (PLN) and other severe organ involvement (CNS, vasculitis):
NIH Protocol (IV pulse CYC):
- Initial dose: 0.75 g/m² IV (reduce to 0.5 g/m² if GFR < 1/3 normal)
- Monthly pulses for 6 months (7 total pulses)
- Adjust to keep WBC nadir > 1500/mm³; max dose 1 g/m²
- Bladder protection: Vigorous hydration + mesna (20% of CYC dose) to prevent hemorrhagic cystitis
- Key toxicities: Myelosuppression, gonadal toxicity (premature ovarian failure), infections (especially herpes zoster), bladder carcinoma
5. Biologic Agents
Belimumab (anti-BAFF/BLyS monoclonal antibody)
- FDA-approved for active SLE and active lupus nephritis
- Consider when: persistent disease activity or frequent flares despite standard of care; unable to taper GCs to acceptable dose; add-on to standard therapy in LN
- Given IV or subcutaneously
Anifrolumab (anti-interferon-α/β receptor antibody)
- FDA-approved for moderate-to-severe nonrenal SLE on background standard therapy
- Targets the type I interferon pathway, which is hyperactivated in most SLE patients
Rituximab (anti-CD20 B-cell depleting antibody)
- Reserved for severe or refractory SLE - not FDA-approved for SLE but widely used off-label
- Useful in refractory LN, severe cytopenias, neuropsychiatric SLE
Obinutuzumab (next-generation anti-CD20)
- Phase 3 trials ongoing for proliferative LN; showed superior complete renal response vs. placebo in the NOBILITY phase 2 trial (35% vs. 23% at 52 weeks) - PMID 39927615
6. Lupus Nephritis - Specific Approach
| Class | Induction | Maintenance |
|---|---|---|
| Proliferative LN (III/IV) | MMF (2-3 g/day) or IV CYC | MMF or AZA for ≥ 18-24 months |
| Membranous LN (V) | MMF preferred | MMF or AZA |
| Add-on | Belimumab + MMF/CYC | Continue belimumab |
- Add voclosporin (calcineurin inhibitor, CNI) or belimumab to MMF/GC induction for enhanced renal response (approved combinations)
- HCQ continued throughout; reduces risk of end-stage renal disease even in LN
7. Antiphospholipid Syndrome (aPL-positive SLE)
- Low-dose aspirin (antiplatelet) for primary prevention
- Long-term anticoagulation (warfarin, target INR 2-3) for patients with thrombotic events
- Avoid direct oral anticoagulants (DOACs) in triple-positive aPL
8. Adjunct/Supportive Measures
- Sun protection (UV triggers flares)
- Vaccinations (especially influenza, pneumococcus, COVID-19) - avoid live vaccines on immunosuppression
- Smoking cessation, weight control, BP/lipid/glucose management
- Nephroprotective agents in LN: ACE inhibitors or ARBs to reduce proteinuria
- Calcium + vitamin D supplementation on chronic steroids
- Osteoporosis prophylaxis with bisphosphonates if on long-term GCs
Treatment Targets
| Target | Definition |
|---|---|
| Remission | Clinical SLEDAI = 0, prednisone ≤ 5 mg/day, stable HCQ/IS/biologics |
| Low disease activity (LLDAS) | SLEDAI ≤ 4, HCQ, prednisone ≤ 7.5 mg/day, stable IS |
Sources:
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set (2022), Chapter 82
- Goldman-Cecil Medicine International Edition (2022), Chapter on Immunomodulatory Agents
- Recent RCT: Obinutuzumab in LN - Furie et al., NEJM 2025 [PMID 39927615]
This is a shared conversation. Sign in to Orris to start your own chat.