Explain minimum alveolar concentration
Reading File
Finding Sources
Searching PubMed
minimum alveolar concentration inhaled anesthetics
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from three major anesthesia textbooks. Let me compose the full answer.
Minimum Alveolar Concentration (MAC)
Definition
MAC is the alveolar concentration of an inhaled anesthetic (expressed as volume % at 1 atmosphere) that prevents movement in response to a standardized surgical stimulus (typically a skin incision) in 50% of subjects. It was defined by Eger and colleagues in the 1960s and remains the primary measure of inhaled anesthetic potency.
Because alveolar concentration rapidly equilibrates with brain partial pressure (in well-perfused organs), MAC mirrors the concentration of anesthetic at its site of action in the CNS. It is therefore directly analogous to the EC₅₀ (median effective concentration) used for intravenous drugs.
"MAC is a useful measure because it mirrors brain partial pressure, allows comparisons of potency between agents, and provides a standard for experimental evaluations."
- Morgan & Mikhail's Clinical Anesthesiology, 7e
MAC Values of Common Agents
| Agent | MAC (%) |
|---|---|
| Nitrous oxide (N₂O) | ~105* |
| Halothane | 0.75 |
| Isoflurane | 1.2 |
| Sevoflurane | 2.0 |
| Desflurane | 6.0 |
*A MAC >100% means hyperbaric conditions are required to achieve 1.0 MAC at sea level. Lower MAC = higher potency.
MAC Variants
These are extension of the basic concept to different clinical endpoints:
| Variant | Description | Approximate value |
|---|---|---|
| Standard MAC | Prevents movement to incision in 50% | 1.0 MAC |
| 1.3 MAC | Prevents movement in ~95% (≈ EC₉₅) | 1.3× standard MAC |
| MAC-awake | Alveolar concentration at eye-opening to command | 0.15-0.5 MAC |
| MAC-BAR | Blunts adrenergic response to noxious stimuli | ~1.5× standard MAC |
| MAC-amnesia | Loss of awareness/recall | ~0.4-0.5 MAC |
The MAC-awake hysteresis is notable: patients lose consciousness at ~0.4-0.5 MAC but may regain it at lower concentrations (as low as 0.15 MAC), likely because of differing wash-in vs. wash-out kinetics.
MAC Additivity
MAC values from different agents are roughly additive for the immobility endpoint. For example:
- 0.5 MAC isoflurane + 0.5 MAC N₂O = ~1.0 MAC (equivalent suppression of movement)
However, additivity does not hold for all endpoints. Cardiovascular effects are not simply additive: 0.6 MAC N₂O + 0.6 MAC isoflurane causes less hypotension than 1.2 MAC isoflurane alone, because isoflurane is a more potent vasodilator and myocardial depressant per MAC equivalent than N₂O. - Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
Meyer-Overton Correlation and Potency
The classic Meyer-Overton correlation shows that anesthetic potency (1/MAC) correlates with lipid-water partition coefficient - agents more soluble in lipid are more potent. This originally supported a lipid membrane theory of anesthetic action. However, modern understanding shows anesthetics bind directly to specific protein targets (e.g., GABA-A receptors, NMDA receptors).
The plot below illustrates this correlation across many compounds:
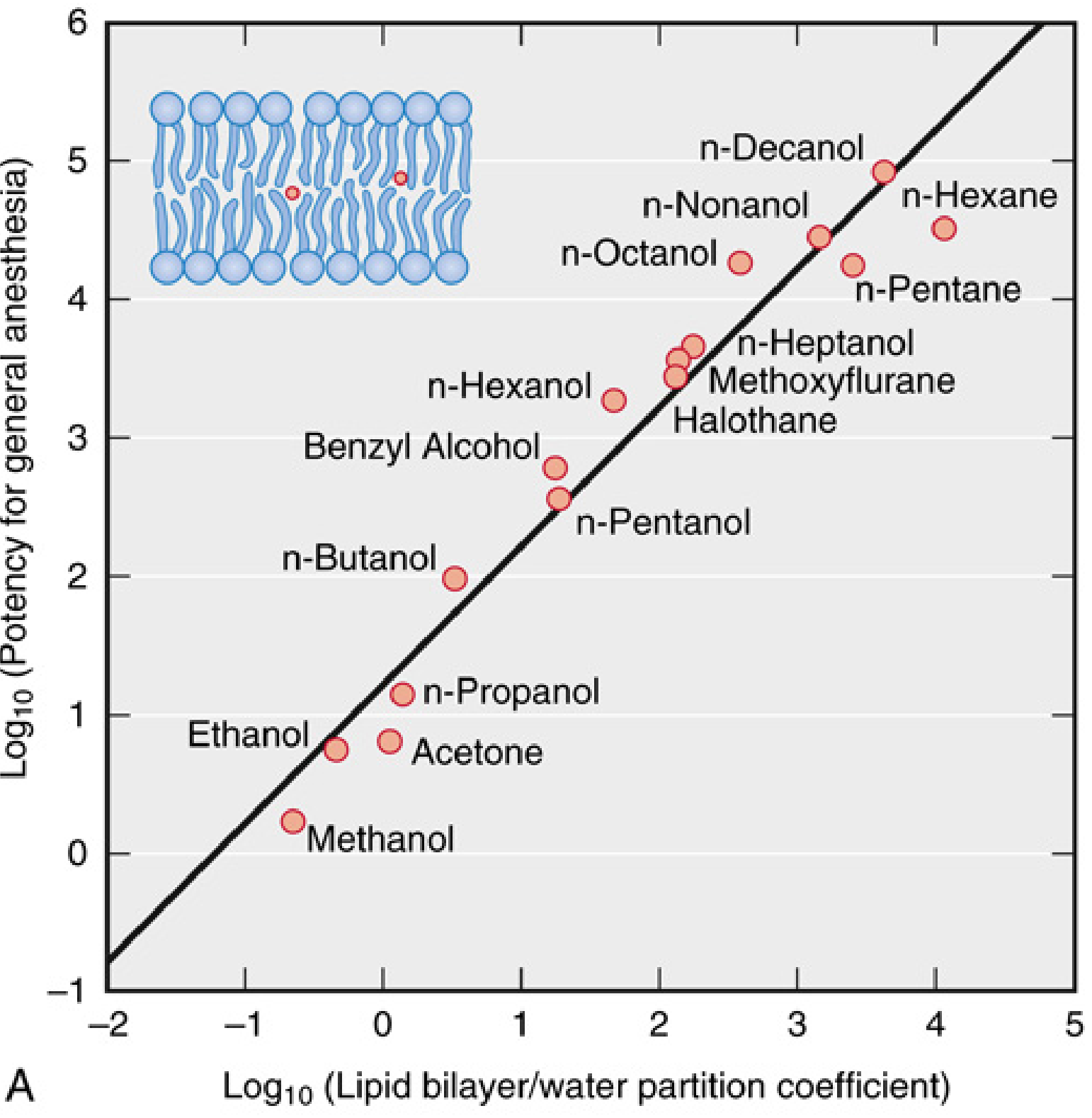
(From Miller's Anesthesia, 10e - each point is a different compound; the diagonal line shows the near-perfect log-log relationship)
Factors Modifying MAC
Factors that INCREASE MAC (more anesthetic required)
- Hyperthermia
- Hypernatremia
- Chronic ethanol abuse
- Elevated CNS catecholamines (MAO inhibitors, acute cocaine/amphetamine/ephedrine/levodopa)
- Red hair (MC1R mutations - ~19% increase, particularly in females)
Factors that DECREASE MAC (less anesthetic required)
- Increasing age - approximately 6% decrease per decade; ~22% decrease from age 40 to 80
- Hypothermia
- Hyponatremia / hypo-osmolality
- Metabolic acidosis
- Hypoxia (PaO₂ <38 mmHg)
- Severe hypotension (MAP <50 mmHg)
- Pregnancy
- Acute ethanol administration
- Drugs: opioids, benzodiazepines, barbiturates, ketamine, lidocaine, α₂-agonists (e.g., dexmedetomidine), verapamil, Δ-9-THC
- Severe anemia (<4.3 mL O₂/dL blood)
Factors that do NOT alter MAC
- Duration of anesthesia
- Sex (with the exception of the red hair effect)
- Type of surgical stimulation
- Thyroid dysfunction
- Hypo/hypercarbia (within usual clinical ranges)
- Metabolic alkalosis
- Hyperkalemia
- Magnesium levels
Clinical Limitations of MAC
MAC is a population median (ED₅₀), not a precise guide for the individual patient. It is most useful during maintenance, not during rapid concentration changes (induction/emergence). The 95% confidence range is approximately ±25% around stated MAC values. In practice, 1.2-1.3 MAC is the target during maintenance to reliably prevent movement in most patients.
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 294-295
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, pp. 1407-1410
- Miller's Anesthesia, 10e, pp. 1807-1809, 2274
This is a shared conversation. Sign in to Orris to start your own chat.