Ncpf and splenomegaly
Reading File
Finding Sources
Finding Sources
Searching PubMed
"non-cirrhotic portal fibrosis" AND splenomegaly
Finding Sources
Finding Sources
Searching PubMed
"non-cirrhotic portal fibrosis" AND splenomegaly
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Here is a detailed answer:
Non-Cirrhotic Portal Fibrosis (NCPF) and Splenomegaly
What is NCPF?
Non-cirrhotic portal fibrosis (NCPF) - also called idiopathic portal hypertension (IPH), hepatoportal sclerosis, Banti syndrome, and idiopathic noncirrhotic portal hypertension (INCPH) - is a syndrome characterized by:
- Portal hypertension
- Patent hepatic and extrahepatic portal veins
- Absence of cirrhosis or a recognizable cause of cirrhosis
- Normal or near-normal liver function
These terms have been "indiscriminately used to describe the same entity." - Sleisenger & Fordtran's GI and Liver Disease
Splenomegaly in NCPF - The Hallmark Feature
NCPF causes massive splenomegaly - this is its most striking and characteristic finding. The splenomegaly in NCPF is typically far greater than that seen in cirrhotic portal hypertension.
The classic triad of NCPF is:
- Massive splenomegaly
- Pancytopenia (hypersplenism - thrombocytopenia, leukopenia, anaemia)
- Absence of stigmata of liver dysfunction (no jaundice, no ascites at presentation, no palmar erythema, no spider naevi)
"Non-cirrhotic portal fibrosis, a condition common in tropical countries, is associated with massive splenomegaly and pancytopenia without stigmata of liver dysfunction."
- Bailey & Love's Short Practice of Surgery, 28th Ed.
Pathophysiology
The mechanism of splenomegaly in NCPF is presinusoidal portal hypertension:
- Obliterative portal venopathy and subendothelial thickening of intrahepatic portal veins cause increased resistance to portal blood flow
- The obstruction is presinusoidal, so sinusoidal (hepatic venous) pressure is relatively preserved - this explains why liver function remains normal
- Elevated portal pressure leads to congestion of the spleen, causing progressive splenomegaly
- Splenic enlargement results in sequestration and destruction of blood cells - this is hypersplenism, producing the characteristic pancytopenia
Histological Features
Liver biopsy findings supporting NCPF/INCPH include:
- Obliterative portal venopathy (obliteration of small intrahepatic portal vein branches)
- Nodular regenerative hyperplasia
- Periportal/perisinusoidal fibrosis
- Absence of true cirrhosis (bridging fibrosis, regenerative nodules)
Yamada's Textbook of Gastroenterology notes NCPF is differentiated from cirrhosis on MR elastography by a higher spleen-to-liver stiffness ratio.
Associated Conditions (Causes/Predisposing Factors)
INCPH/NCPF is associated with four categories (Sleisenger & Fordtran's):
- Drugs and toxins: purine analogs (didanosine, azathioprine, 6-thioguanine), oxaliplatin
- Immune disorders: connective tissue diseases, common variable immunodeficiency (CVID), HIV infection
- Prothrombotic conditions: myeloproliferative disorders, antiphospholipid syndrome, protein S deficiency
- Genetic disorders: Turner syndrome, telomerase disease, Adams-Oliver syndrome
50% of cases remain unexplained. The condition is particularly common in India (tropical countries), though its incidence appears to be declining.
Clinical Features
| Feature | NCPF | Cirrhosis |
|---|---|---|
| Splenomegaly | Massive | Moderate |
| Liver function tests | Near normal | Abnormal |
| Ascites | Late/absent initially | Common |
| Oesophageal varices | Present | Present |
| Pancytopenia | Prominent (hypersplenism) | Present but milder |
| Jaundice | Absent | Often present |
| Liver stiffness | Low | High |
Upper GI bleeding from oesophageal varices is often the presenting complaint. Patients tolerate bleeding better than cirrhotics because liver synthetic function is preserved.
Investigations
- Endoscopy: Oesophageal/gastric varices
- Ultrasound + Doppler: Splenomegaly, patent portal and hepatic veins, no features of cirrhosis
- CT/MRI: Confirms splenomegaly, rules out portal vein thrombosis, may show periportal changes
- MR elastography: High spleen-to-liver stiffness ratio (distinguishes from cirrhosis)
- Liver biopsy: Confirms obliterative portal venopathy, absence of cirrhosis
- Fibroscan (transient elastography): Liver stiffness is typically LOW (distinguishing from cirrhosis)
- Blood counts: Pancytopenia from hypersplenism
Management
Variceal bleeding:
- Propranolol (beta-blocker) for prevention of recurrent variceal bleeding - controlled trials confirm efficacy in NCPF patients
- Endoscopic variceal band ligation / sclerotherapy
- TIPS or portosystemic shunts for refractory bleeding
Splenomegaly / Hypersplenism:
- Splenectomy or partial splenic embolization (PSE) for severe symptomatic hypersplenism (severe pancytopenia)
- After splenectomy, there is an increased risk of glomerulonephritis (noted in Brenner & Rector's The Kidney - splenorenal shunt surgery also associated with increased GN incidence)
Anticoagulation: Only if an underlying prothrombotic disorder is identified
Key Distinguishing Points (Exam Focus)
- NCPF causes massive splenomegaly with preserved liver function - the classic differentiator from cirrhosis
- The pancytopenia is due to hypersplenism (sequestration), not bone marrow failure
- Variceal bleeding is well tolerated because hepatic reserve is maintained
- Liver biopsy shows obliterative portal venopathy, NOT cirrhosis
- Fibroscan shows low liver stiffness but high splenic stiffness
Sources: Bailey & Love's Surgery (28th Ed.) | Sleisenger & Fordtran's GI and Liver Disease | Yamada's Textbook of Gastroenterology (7th Ed.) | Robbins Pathologic Basis of Disease | APASL Guidelines (Sarin SK et al., Hepatol Int 2007)
Cardiac cirrhosis
Finding Sources
Finding Sources
Searching PubMed
"cardiac cirrhosis" AND liver
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Cardiac Cirrhosis
Definition
Cardiac cirrhosis (also called congestive hepatopathy or cardiac hepatopathy) is chronic liver injury resulting from long-standing right-sided or biventricular congestive heart failure, causing sustained elevation of central venous pressure that is transmitted to the hepatic sinusoids. It is an increasingly uncommon cause of chronic liver disease given advances in heart failure management, but its incidence is rising in patients with congenital heart disease - especially after the Fontan procedure.
- Harrison's Principles of Internal Medicine, 22nd Ed.
Pathophysiology - Step by Step
The sequence of events is:
- Right-sided heart failure → elevated venous pressure → transmitted via IVC and hepatic veins to hepatic sinusoids
- Sinusoidal congestion and dilatation → sinusoidal edema → decreased oxygen delivery to hepatocytes
- Centrilobular (Zone 3) hepatocyte ischemia and necrosis - Zone 3 is most vulnerable because it is furthest from the portal arterial supply and is directly adjacent to the hepatic venule; when left-sided failure co-exists (poor cardiac output), this hypoperfusion worsens the centrilobular necrosis
- Mechanical force from sinusoidal distension + intravascular stasis → promotes intravascular microthrombi → localized ischemia → pericentral (centrilobular) fibrosis
- With chronic and repeated insults, fibrosis progresses outward, eventually bridging between central veins (rather than between portal tracts) → "reverse lobulation"
- End result: established cardiac cirrhosis
"Right-sided heart failure results in transmission of increased central venous pressure from the heart directly to the hepatic sinusoids. The result is centrilobular congestion and sinusoidal edema that further decrease oxygen delivery... The acute and chronic damage results in progressive centrilobular fibrosis."
- Sleisenger & Fordtran's GI and Liver Disease
Gross Pathology - "Nutmeg Liver"
In acute/subacute congestion, the gross appearance is the "nutmeg liver":
- Central (centrilobular) areas appear dark red (congested, necrotic) and slightly depressed
- Surrounding parenchyma is tan/yellow (viable hepatocytes)
- The mottled pattern on cut surface resembles a cut nutmeg - hence the name
Histopathology
The histologic hallmarks are:
| Feature | Description |
|---|---|
| Sinusoidal dilatation | Enlarged, engorged sinusoids in Zone 3 |
| Hepatocyte atrophy | Compression/atrophy of centrilobular hepatocytes |
| Centrilobular necrosis | Loss of Zone 3 hepatocytes; correlates with recent hypotension |
| Centrilobular fibrosis | Perivenular fibrosis developing around central veins |
| Bridging fibrosis | Connects central vein to central vein (not portal tract to portal tract - the key distinguishing feature) |
| "Reverse lobulation" | Portal tracts become the center of "pseudonodules" with central veins at the periphery |
| No/sparse inflammation | The cirrhosis is bland - minimal inflammatory infiltrate |
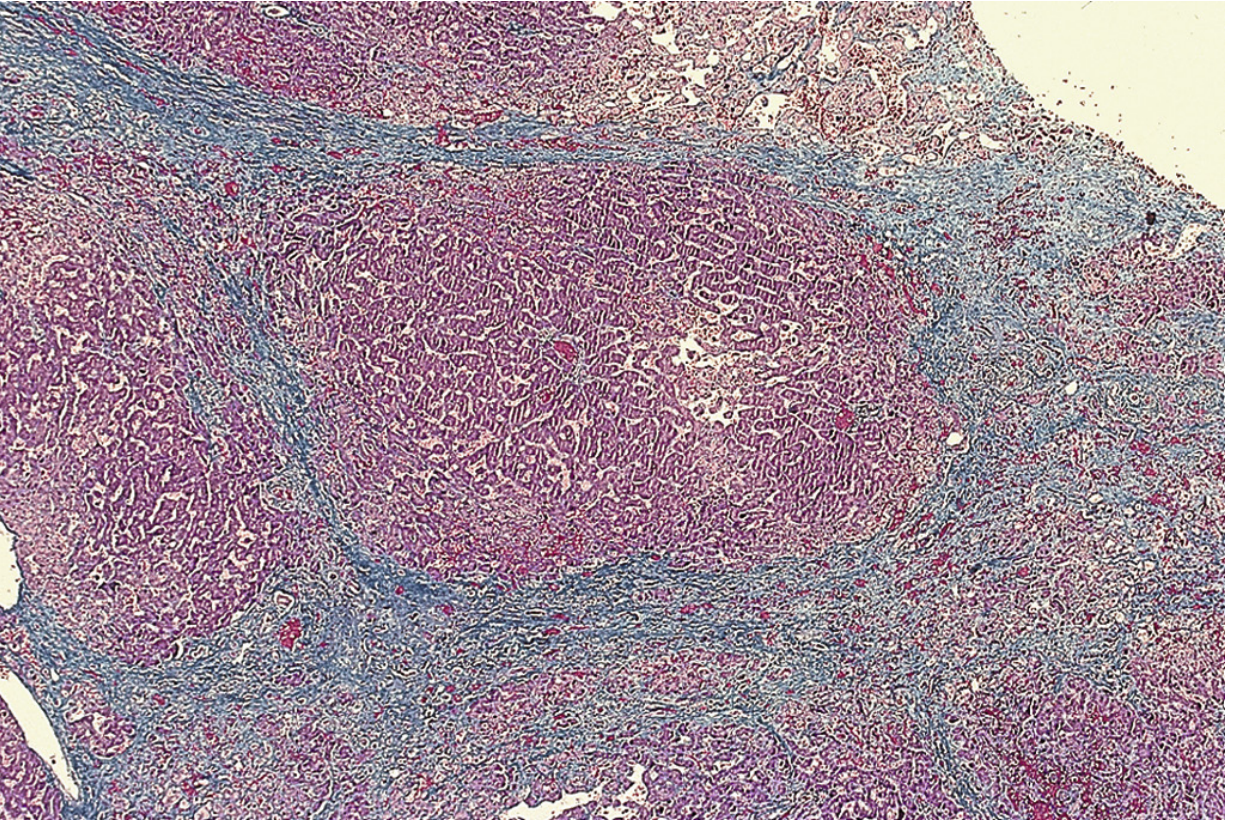
Histopathology of cardiac cirrhosis: portal tract lies centrally in a regenerative nodule; fibrotic bands bridge central veins - the reverse lobulation pattern. Sinusoids are dilated and congested. No inflammatory cells. (Masson trichrome stain.) - Sleisenger & Fordtran's
Causes of Cardiac Cirrhosis
Any cause of sustained right-heart failure can lead to it:
- Right heart failure from any cause: ischemic cardiomyopathy, dilated cardiomyopathy
- Valvular disease: tricuspid regurgitation (pulsatile liver), mitral stenosis (raises pulmonary and right heart pressures)
- Constrictive pericarditis
- Pulmonary hypertension
- Congenital heart disease: particularly after the Fontan procedure (see below)
Clinical Features
Symptoms/signs are dominated by the underlying heart disease. Liver-specific features:
- Hepatomegaly - often the most prominent finding; liver is firm and enlarged
- Pulsatile liver - specifically with tricuspid regurgitation (venous pulsations transmitted to liver)
- Hepatojugular reflux - JVP rises on pressing over the liver
- Dull RUQ pain - capsular distension from hepatomegaly
- Ascites - high serum-ascites albumin gradient (SAAG >1.1 g/dL), high protein concentration (>2.5 g/dL) - distinguishing it from portal hypertensive ascites from cirrhosis
- Jaundice - mild; seen in <10% of patients, typically with severe/acute heart failure
- Peripheral edema and pleural effusions - from heart failure itself
- Splenomegaly - from portal hypertension (congestive splenomegaly)
- Spider telangiectasias and varices - usually NOT present; variceal bleeding does not occur from congestive hepatopathy alone
Laboratory Findings
| Test | Finding |
|---|---|
| Serum bilirubin | Mildly elevated (<3 mg/dL) in most; the most common abnormality |
| ALP | Characteristically elevated |
| AST/ALT | Normal or mildly elevated; AST usually > ALT |
| Prothrombin time | Prolonged in >75% of cases; resistant to vitamin K |
| Albumin | May be low (synthetic dysfunction in severe/established cirrhosis) |
| LFTs on treatment | Improve slowly or normalize with effective cardiac therapy |
"ALP levels are characteristically elevated, and aminotransferases may be normal or slightly increased, with AST usually higher than ALT."
- Harrison's, 22nd Ed.
Important: If aminotransferases are markedly elevated (>3000 U/L) in a heart failure patient, think ischemic hepatitis ("shock liver") - a distinct, acute superimposed condition where ALT/LDH ratio <1.5 is characteristic.
Imaging
- Ultrasound: Hepatomegaly, ascites, dilated IVC and hepatic veins (key finding), splenomegaly
- CT with contrast: Inhomogeneous hepatic enhancement during portal phase; dilated hepatic veins and IVC; hepatomegaly
- Doppler US: May detect pulsatile hepatic vein flow in tricuspid regurgitation
Differentiation from Other Conditions
| Feature | Cardiac Cirrhosis | Budd-Chiari Syndrome | Sinusoidal Obstructive Syndrome (SOS/VOD) |
|---|---|---|---|
| Cause | Right heart failure | Hepatic vein thrombosis | Bone marrow transplant conditioning; pyrrolizidine alkaloids |
| Biopsy | Centrilobular fibrosis; no RBC extravasation | Centrilobular necrosis + RBC extravasation | Centrilobular congestion + occlusion of sinusoids |
| IVC/hepatic veins | Dilated | Occluded | Patent |
| Ascites protein | High | High | High |
| Key distinguishing sign | Pulsatile liver (TR); JVP elevated | No cardiac cause | Post-BMT setting |
Fontan-Associated Liver Disease (FALD)
A growing special population: patients with single ventricle physiology who undergo the Fontan procedure (systemic venous blood routed directly to pulmonary artery, bypassing the right ventricle) develop chronic passive hepatic congestion from elevated systemic venous pressures. Long-term complications include:
- Progressive liver fibrosis and cirrhosis
- Portal hypertension - oesophageal varices in ~20-50% of older Fontan patients
- Hepatocellular carcinoma (HCC) - a recognized long-term risk
- Combined heart-liver transplantation may be required in advanced cases
Current guidelines recommend liver imaging (USG, CT, MRI) and fibrosis markers as part of routine surveillance in adult Fontan patients.
- Fuster & Hurst's The Heart, 15th Ed.
Treatment
- Primary treatment: Optimise the underlying cardiac disease (diuretics, ACE inhibitors, cardiac resynchronisation, valve repair/replacement, heart transplantation)
- Liver function tests improve with effective cardiac therapy
- Paracentesis for tense ascites when needed
- Variceal bleeding prophylaxis if varices develop (uncommon in pure congestive hepatopathy)
- In FALD with end-stage liver disease: consider combined heart-liver transplantation
"The presence of congestive hepatopathy does not affect the prognosis in patients with heart failure; the mortality rate is determined primarily by the severity of the underlying cardiac disease."
- Sleisenger & Fordtran's GI and Liver Disease
Key Exam Points
- Cardiac cirrhosis is due to right heart failure - the raised CVP is transmitted to hepatic sinusoids
- Fibrosis bridges central vein to central vein - "reverse lobulation" - not portal to portal (as in typical cirrhosis)
- Grossly = "nutmeg liver"; histologically = bland, no inflammation, dilated sinusoids
- Pulsatile liver = tricuspid regurgitation
- Ascites has high SAAG + high protein
- Prothrombin time prolonged and vitamin K resistant
- Variceal bleeding is uncommon; distinguish from Budd-Chiari by absence of RBC extravasation on biopsy
- Fontan procedure patients are an important emerging group at risk for FALD and HCC
Sources: Harrison's Principles of Internal Medicine (22nd Ed.) | Sleisenger & Fordtran's GI and Liver Disease | Robbins & Kumar Basic Pathology | Robbins, Cotran & Kumar Pathologic Basis of Disease | Frameworks for Internal Medicine | Fuster & Hurst's The Heart (15th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.