Parotid gland anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have thorough content from multiple authoritative textbooks. Here is the comprehensive answer:
Parotid Gland Anatomy
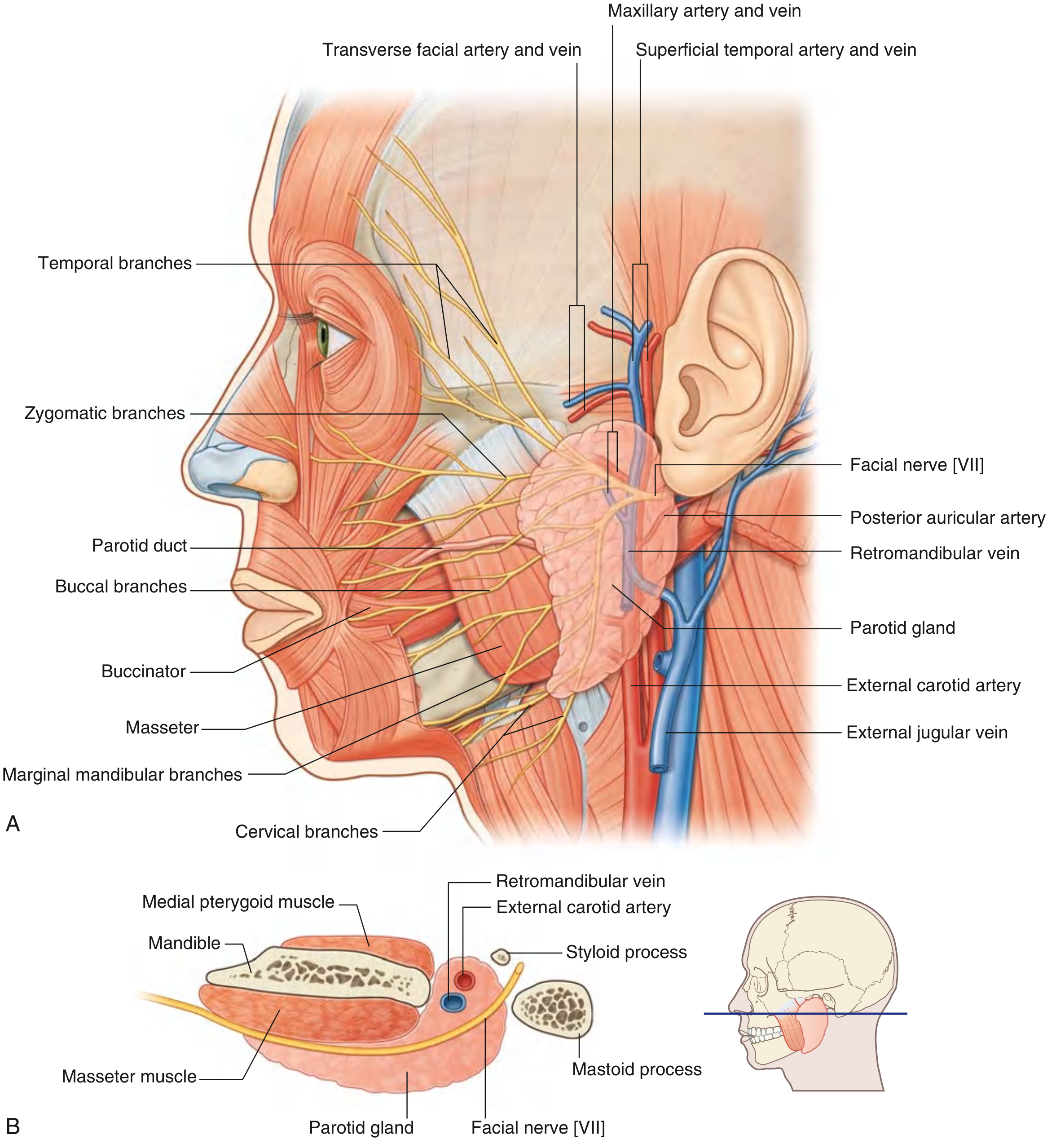
Fig. 8.65 - Parotid Gland. (A) Lateral view showing facial nerve branches, parotid duct, and vascular relationships. (B) Cross-section showing deep relations. — Gray's Anatomy for Students
Overview
The parotid gland is the largest of the three paired major salivary glands. It is a purely serous gland, producing watery saliva rich in salivary amylase.
Location and Borders
| Border | Relation |
|---|---|
| Anterior | Masseter muscle |
| Superior | Zygomatic arch |
| Posterior | Tragal cartilage and sternocleidomastoid muscle |
| Inferior (tail) | Between ramus of mandible and SCM, overlying the digastric muscle |
| Deep | Pretyloid compartment of the parapharyngeal space |
The gland sits anterior to and below the lower half of the ear, superficial, posterior, and deep to the ramus of the mandible. It extends from the lower border of the mandible up to the zygomatic arch, and posteriorly it covers the anterior part of the sternocleidomastoid muscle, continuing anteriorly to halfway across the masseter muscle.
- Gray's Anatomy for Students, p. 1051
- K.J. Lee's Essential Otolaryngology, p. 642
Lobes
The parotid is divided into superficial and deep lobes by the facial nerve. About 80% of parotid parenchyma is superficial lobe. Histologically these are not true distinct lobes (no true fascial plane separates them) - the facial nerve is the surgical dividing landmark.
Fascia
The gland is enclosed by the parotidomasseteric fascia (part of the investing layer of deep cervical fascia):
- Attaches to the root of the zygoma superiorly
- Thick attachment to the mastoid process posteriorly
- Thin fascia separates it from tragal/conchal cartilage anteriorly
- Thick fascia at the anterior-inferior tip separates it from the submandibular gland
Parotid Duct (Stensen's Duct)
- Emerges from the anterior border of the gland, midway between the zygomatic arch and the corner of the mouth
- Traverses over the masseter muscle
- At the anterior border of masseter, turns medially, pierces the buccinator muscle
- Opens into the oral cavity adjacent to the upper second molar tooth (parotid papilla)
Structures Passing Through the Parotid
The parotid is unique among salivary glands in having major structures coursing through its substance. From superficial to deep (mnemonic: Some Rebels Fight: Snobbish Rascals Fight, or remembered as: facial nerve - retromandibular vein - external carotid artery, superficial to deep):
1. Facial Nerve (CN VII)
- Exits the skull via the stylomastoid foramen (posterolateral to the styloid process, anteromedial to the mastoid process)
- Enters the parotid and forms the pes anserinus (goose's foot) where it divides into upper (temporofacial) and lower (cervicofacial) divisions
- Five terminal groups emerge from the borders of the gland:
- Temporal - from upper border
- Zygomatic - from upper/anterior border
- Buccal - from anterior border
- Marginal mandibular - from lower border
- Cervical - from lower border
Surgical landmarks to identify the facial nerve trunk:
- Tympanomastoid suture line
- Posterior belly of the digastric muscle (marks the depth of the nerve)
- Tragal pointer (the nerve lies ~1 cm deep and inferior to the tip of the tragal cartilage)
- Retrograde identification by tracing a peripheral branch
Note: In children under 2 years, the facial nerve trunk and divisions are more superficial.
2. Retromandibular Vein
- Formed within the parotid substance by the junction of the superficial temporal vein and maxillary vein
- Passes inferiorly through the gland
- Divides just below the inferior border into anterior and posterior branches
- The anterior branch joins the internal jugular vein (via the common facial vein); the posterior branch joins the external jugular vein
3. External Carotid Artery
- Enters at the inferior border of the gland (or passes deep to it)
- Gives off the posterior auricular artery within/near the parotid
- Terminates into two branches near the lower border of the ear:
- Maxillary artery - passes horizontally, deep to the mandible
- Superficial temporal artery - continues superiorly, gives off the transverse facial artery, then emerges from the upper border of the gland
Lymphatics
The parotid is unique in having both intraglandular (~20 nodes) and periglandular lymph nodes (unlike the submandibular gland, which has only periglandular nodes). This is clinically important as cutaneous malignancies of the scalp, temple, and face can metastasize to intraparotid nodes.
- K.J. Lee's Essential Otolaryngology, p. 643
Innervation
Secretomotor (Parasympathetic)
- Preganglionic: Glossopharyngeal nerve (CN IX) via the lesser petrosal nerve
- Relay: Otic ganglion (just inferior to the foramen ovale, associated with CN V3)
- Postganglionic: Auriculotemporal nerve (branch of CN V3) carries the postganglionic fibers to the gland
Sensory
- Auriculotemporal nerve (branch of mandibular nerve CN V3)
Sympathetic
-
From the superior cervical ganglion (vasoconstrictor fibers)
-
Gray's Anatomy for Students, p. 1052
Accessory Parotid
A small accessory parotid lobe is present in approximately 20% of individuals, lying on the masseter muscle along the parotid duct. It is important to recognize as a source of benign or malignant tumors.
Parapharyngeal Space Relationship
The deep lobe of the parotid relates to the pretyloid (prestyloid) compartment of the parapharyngeal space. Deep lobe parotid tumors can present as a pharyngeal mass. The poststyloid compartment contains the carotid sheath structures (ICA, IJV, CN IX-XII).
Clinical Correlations
| Condition | Anatomy relevance |
|---|---|
| Parotid tumors | 80% in superficial lobe; facial nerve at risk during excision |
| Frey's syndrome | Post-parotidectomy gustatory sweating; aberrant regeneration of auriculotemporal parasympathetic fibers to sweat glands |
| Parotid calculi | Typically form in the duct or main ductal confluence; pain on salivation |
| Sensory loss post-surgery | Greater auricular nerve (C2, C3) injury causes numbness over angle of mandible and lower pinna |
| Facial palsy | Risk from parotid surgery; temporary neuropraxia resolves in 4-6 weeks; permanent palsy ~1-2% |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
- Gray's Anatomy for Students, p. 1051-1052
- K.J. Lee's Essential Otolaryngology, p. 642-643
This is a shared conversation. Sign in to Orris to start your own chat.