Xray of chest
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
I now have all the key content and images. Let me compile a comprehensive answer.
Chest X-Ray (CXR) - A Complete Guide
Standard Views
A chest radiograph is the most widely used and cost-effective initial imaging test for thoracic disease. Two standard projections are obtained:
- PA (posteroanterior) - patient stands erect, X-ray beam passes back-to-front. This is the standard view.
- Lateral - taken alongside the PA; better shows posterior lung bases, retrocardiac region, anterior mediastinum, and thoracic spine.
- AP (anteroposterior) - portable/bedside view, used in ICU or immobile patients. Magnifies mediastinal structures and is less sensitive for pneumothorax and effusions.
Supplementary views: lordotic (lung apices), expiratory (small pneumothorax), lateral decubitus (mobile vs. loculated effusion).
- Fishman's Pulmonary Diseases and Disorders, p.465
Normal PA Chest Radiograph

Figure: Normal PA radiograph - Fishman's Pulmonary Diseases
Normal Lateral Chest Radiograph

Figure: Normal lateral radiograph - Fishman's Pulmonary Diseases
Cardiac Anatomy on Lateral CXR (with overlay)
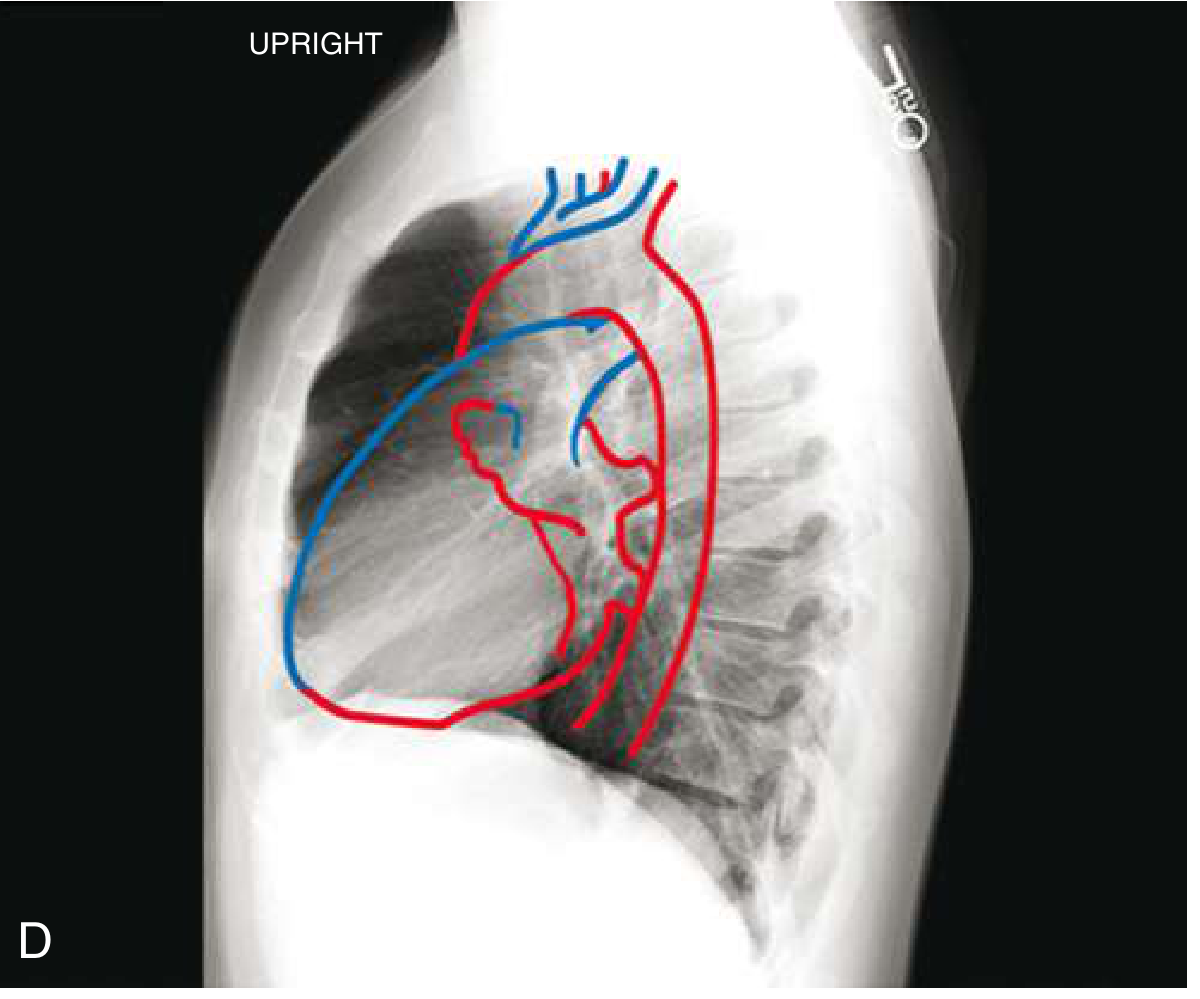
Figure: Lateral CXR with cardiac chambers overlaid - red = right-sided structures; blue = left-sided + pulmonary vasculature - Goldman-Cecil Medicine
Bronchial Anatomy Visible on CXR
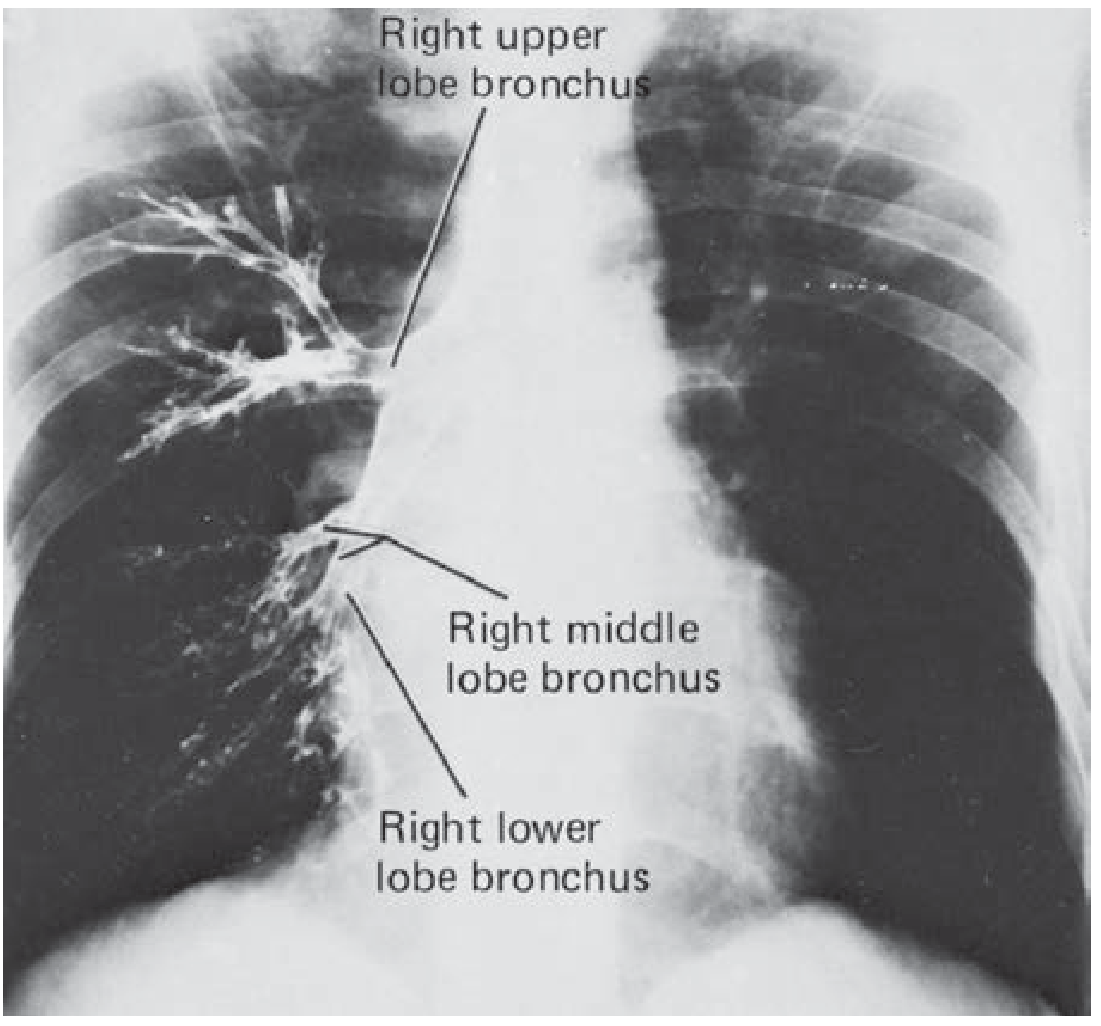
Figure: Right upper, middle, and lower lobe bronchi labeled on PA CXR - Fishman's Pulmonary Diseases
What to Look at on a Chest X-Ray - Systematic Approach
A good approach uses the mnemonic ABCDE (or similar structured scan):
| Zone | What to Assess |
|---|---|
| Airway | Trachea - midline? Carina angle (<70°)? |
| Bones | Ribs, clavicles, scapulae, spine - fractures, lytic lesions |
| Cardiac | Cardiothoracic ratio (<0.5 on PA), shape, chamber borders |
| Diaphragm | Right higher than left by ~1.5 cm, costophrenic angles sharp |
| Everything else | Lung fields, hila, mediastinum, soft tissues |
Cardiac Silhouette
The cardiothoracic (CT) ratio = maximum transverse cardiac diameter / internal thoracic diameter at the level of the right hemidiaphragm. Normal is <0.5 on PA film.
Right heart border (from top to bottom):
- Superior vena cava (SVC)
- Right atrium (RA)
Left heart border (from top to bottom):
- Aortic knuckle (aortic arch)
- Pulmonary artery (PA)
- Left atrial appendage
- Left ventricle (LV) - forms most of the left border
Left ventricular dilation: concave mid-left border, downward-pointing apex below the diaphragm. On lateral film, LV extension >2 cm posterior to the inferior vena cava = LV enlargement.
- Goldman-Cecil Medicine, p.444
Key CXR Abnormalities
1. Pleural Effusion
- Small: blunted posterior then lateral costophrenic angles (requires ~200-500 mL)
- Classic sign: homogeneous basal opacity with a concave upper border (meniscus sign) higher laterally
- Large: dense hemithoracic opacity + contralateral mediastinal shift
- Absent mediastinal shift with a large effusion suggests lung collapse or pleural malignancy (mesothelioma)
- ~1000 mL required to reach level of the 4th anterior rib
- Grainger & Allison's Diagnostic Radiology, p.61
2. Cardiac Failure
| Feature | Type |
|---|---|
| Cardiomegaly, central/basilar opacities, peribronchial cuffing, vascular congestion | Cardiogenic pulmonary edema |
| Normal heart size, peripheral distribution, air bronchograms (80%) | ARDS/non-cardiogenic |
| Cephalization of pulmonary vessels, Kerley B lines, pleural effusion | Elevated wedge pressure (>18 mmHg) |
- Goldman-Cecil Medicine
3. Pneumothorax
- Visible lung edge with absent lung markings peripheral to it
- Erect PA most sensitive; expiratory film may help in small cases
- Tension pneumothorax: tracheal deviation away from affected side
4. Consolidation
- Air space opacity, often with air bronchograms
- Lobar distribution suggests bacterial pneumonia; bilateral perihilar "bat-wing" pattern suggests pulmonary edema
5. Collapse (Atelectasis)
- Tracheal and mediastinal shift toward the affected side
- Elevation of hemidiaphragm, crowding of ribs
6. Trauma Findings
- Rib fractures 1-2 (first/second) → suspect aortic injury
- Lower rib fractures → liver/spleen injury
- Supine AP: hemothorax appears as homogeneous haze; pneumothorax appears more radiolucent
- Up to 300 mL blood can pool behind the diaphragm and not be visible
- Bailey & Love's Surgery, p.895
Technical Adequacy - Before Reading Any CXR
Always check:
- Rotation - medial clavicular heads equidistant from spinous processes
- Inspiration - 5-6 anterior ribs or 9-10 posterior ribs should be visible above the diaphragm
- Penetration/Exposure - vertebral bodies just visible behind cardiac shadow
Advantages of CXR vs Advanced Imaging
| Feature | CXR | CT |
|---|---|---|
| Cost | Low | High |
| Radiation | Low | Higher |
| Availability | Universal, portable | Limited/fixed |
| Detail | Good overview | Superior (3D reconstruction) |
| Small pneumothorax | Lower sensitivity | High sensitivity |
| Mediastinal detail | Limited | Excellent |
The CXR remains the cornerstone of initial imaging for most thoracic conditions. CT is required when CXR findings are ambiguous or more precise characterization of disease is needed.
Sources: Fishman's Pulmonary Diseases & Disorders; Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology; Bailey & Love's Surgery
This is a shared conversation. Sign in to Orris to start your own chat.