✅ CORRECT ANSWER: C) Pyruvate Carboxylase
PART 1 - Decode the Question
What is the examiner actually asking?
"This question is asking which enzyme requires biotin as a cofactor - and which of the listed enzymes would be deficient when someone eats raw eggs (which block biotin absorption)."
Keywords that should immediately trigger your thinking:
| Keyword in Question | What it should make you think |
|---|
| "Raw eggs" | → Avidin → Blocks Biotin absorption |
| "Fatigue on moderate exercise" | → Hypoglycemia → Gluconeogenesis failing |
| "Bodybuilder" | → High protein diet, lots of raw eggs |
| "Enzyme deficient" | → Which enzyme NEEDS biotin to work? |
| "Recently started" | → Acquired deficiency, not genetic |
One-line trigger rule: Whenever you see "raw egg white" in any NEET PG question → immediately think Biotin deficiency → Pyruvate Carboxylase fails.
PART 2 - Explain Like a 10th Class Student
Let's start from absolute zero.
Step 1: What is energy?
Your body is like a car. A car needs petrol to run. Your body needs glucose (a type of sugar) to run. Every muscle, every organ, your brain - all of them run on glucose.
Step 2: Where does your glucose come from?
Normally, you eat food. The food gives glucose. Your body stores extra glucose in the liver and muscles as glycogen (think of glycogen as a fuel tank).
But what happens when you exercise for a long time and your glucose runs out? Your body has a clever backup plan.
Step 3: The backup plan - Gluconeogenesis
Gluconeogenesis - let's break this word:
- Gluco = glucose (sugar)
- Neo = new
- Genesis = creation/birth
So gluconeogenesis literally means "creating new glucose."
When you exercise and your sugar runs low, your liver acts like a factory and makes fresh glucose from other raw materials like:
- Lactic acid (from tired muscles)
- Amino acids (from proteins)
- Glycerol (from fat)
This factory process keeps your blood sugar up so you don't collapse.
Step 4: The factory needs a tool
Imagine you're building something. You need tools. The gluconeogenesis factory needs an enzyme called Pyruvate Carboxylase as its very first tool - its first step.
Enzyme = a protein that speeds up a chemical reaction. Think of it as a machine in a factory.
Pyruvate Carboxylase converts Pyruvate → Oxaloacetate (OAA).
Think of it like this:
- Pyruvate = raw material (scrap metal)
- Oxaloacetate = the first processed product
- From OAA, the factory eventually makes Glucose
Without this first step, the whole glucose factory shuts down.
Step 5: But this tool needs a power source - Biotin
Pyruvate Carboxylase CANNOT work without Biotin (Vitamin B7).
Biotin is like the battery of this enzyme. Without the battery, the machine won't start.
Biotin = a water-soluble vitamin (vitamin that dissolves in water). Also called Vitamin B7 or Vitamin H.
Step 6: Now enters the villain - Avidin from Raw Eggs
Avidin = a protein found in raw egg whites.
Think of avidin like a super-magnet that grabs onto biotin in your gut and holds it so tight that your intestine cannot absorb it.
So the sequence is:
Raw egg white eaten
↓
Avidin (in egg white) enters your gut
↓
Avidin grabs Biotin tightly
↓
Biotin cannot be absorbed into blood
↓
Blood has no Biotin
↓
Pyruvate Carboxylase has no battery → can't work
↓
Gluconeogenesis fails
↓
Blood glucose drops during exercise
↓
FATIGUE on moderate exercise ✓
Important: If you COOK the eggs, heat destroys avidin. So cooked eggs are safe! Bodybuilders who eat raw eggs get this problem.
PART 3 - Images During Every Explanation
The Pyruvate Carboxylase Reaction - How Biotin Works
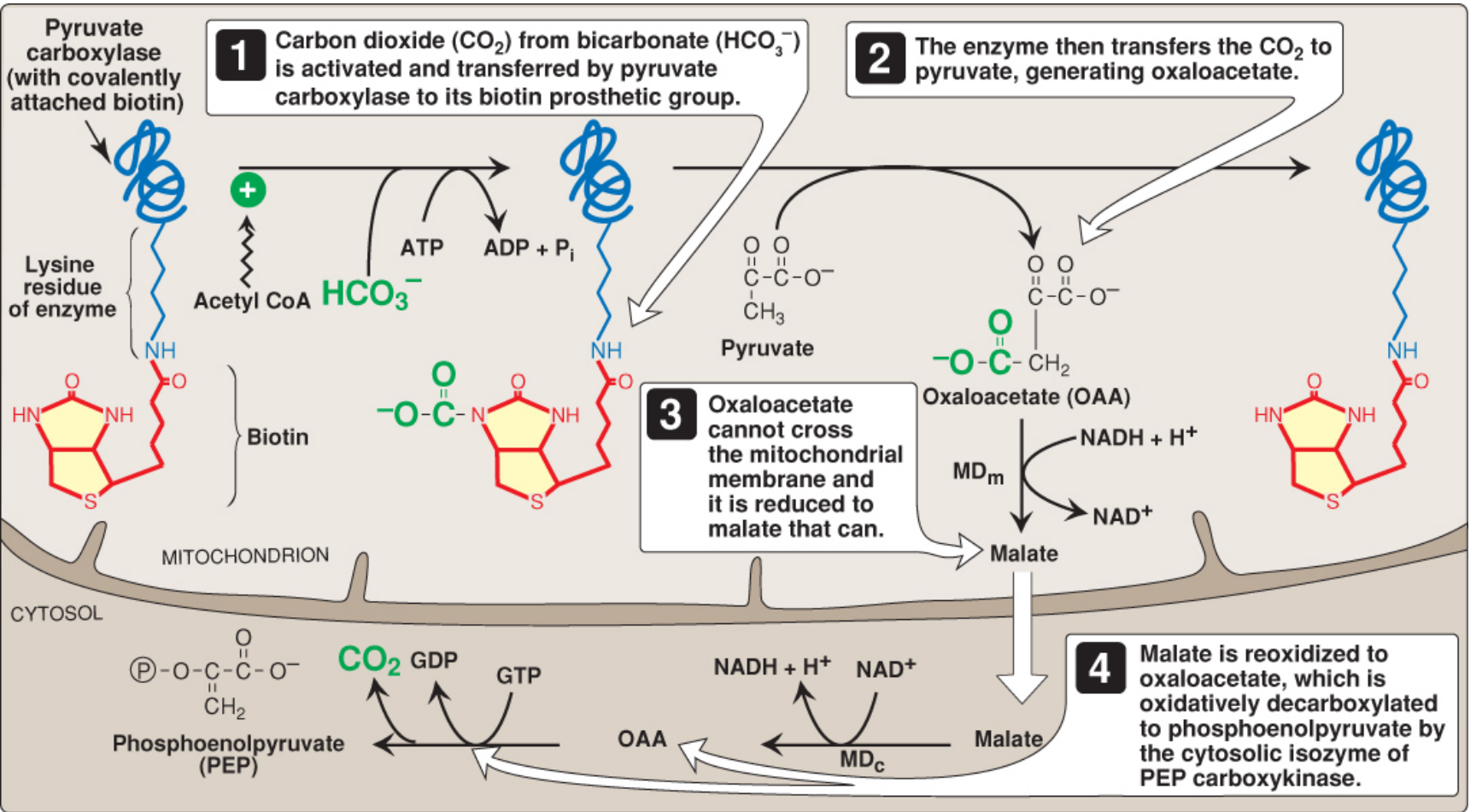
This diagram from Lippincott's Biochemistry shows exactly how biotin sits on the enzyme and transfers CO₂ to pyruvate:
Reading this diagram:
- Top left: Pyruvate carboxylase with biotin covalently (firmly) attached to a lysine residue (part of the enzyme)
- Step 1: CO₂ from bicarbonate (HCO₃⁻) is activated using ATP energy and attached to biotin
- Step 2: Biotin transfers that CO₂ to pyruvate → makes Oxaloacetate (OAA)
- Step 3: OAA cannot cross the mitochondrial wall, so it becomes malate
- Step 4: Malate exits, becomes OAA again in cytosol, then PEPCK converts it to PEP → eventually becomes Glucose
PART 4 - Build the Complete Concept
BIOTIN (Vitamin B7) - Complete Topic
Definition
Biotin is a water-soluble B-vitamin (also called Vitamin H or Vitamin B7) that functions as a coenzyme (cofactor) for 4 carboxylase enzymes in the human body.
Carboxylase = an enzyme that adds a CO₂ group to a molecule.
The 4 Biotin-Dependent Enzymes - THE MOST IMPORTANT TABLE IN THIS TOPIC
| # | Enzyme | Reaction | Pathway | Location |
|---|
| 1 | Pyruvate Carboxylase (PC) | Pyruvate → OAA | Gluconeogenesis | Mitochondria (liver, kidney) |
| 2 | Acetyl-CoA Carboxylase (ACC) | Acetyl-CoA → Malonyl-CoA | Fatty acid synthesis | Cytosol |
| 3 | Propionyl-CoA Carboxylase | Propionyl-CoA → Methylmalonyl-CoA | Odd-chain FA / amino acid catabolism | Mitochondria |
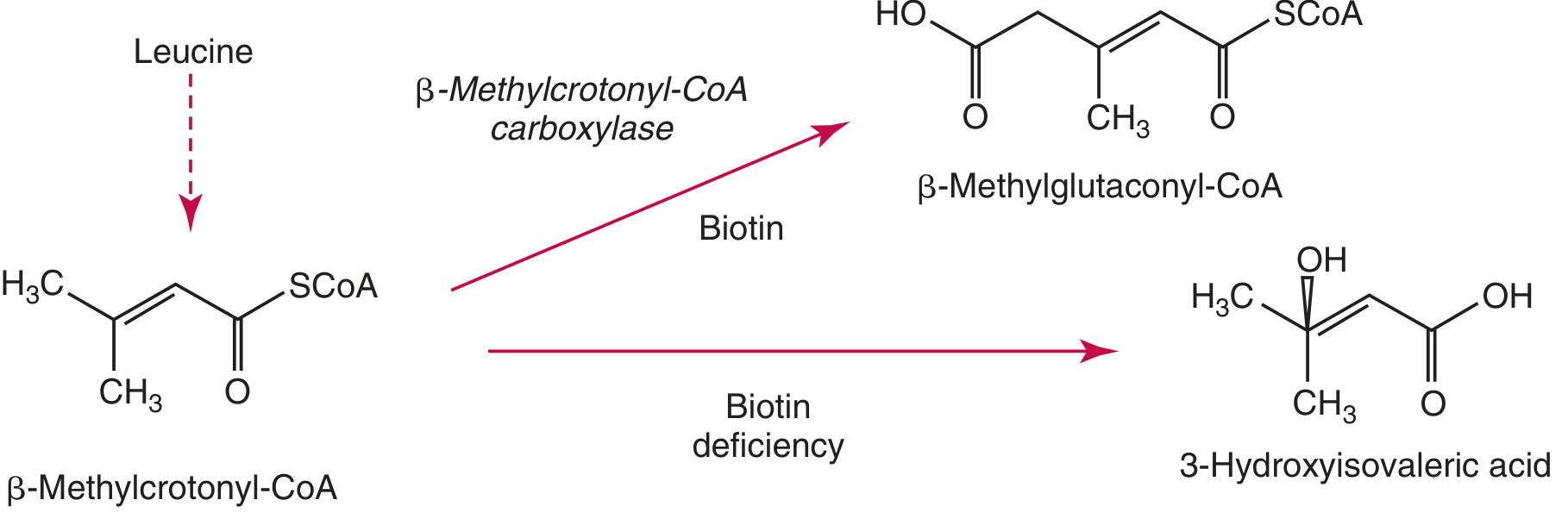
| 4 | 3-Methylcrotonyl-CoA Carboxylase | 3-Methylcrotonyl-CoA → 3-Methylglutaconyl-CoA | Leucine catabolism | Mitochondria |
NEET PG PEARL: All 4 use biotin. Biotin deficiency = ALL 4 fail. The one asked most in NEET PG = Pyruvate Carboxylase (because it causes fatigue/hypoglycemia).
Mnemonic for 4 biotin enzymes: "PPAM"
- Pyruvate carboxylase
- Propionyl-CoA carboxylase
- Acetyl-CoA carboxylase
- 3-Methylcrotonyl-CoA carboxylase
Gluconeogenesis - The Complete Pathway
Gluconeogenesis = Synthesis of glucose from non-carbohydrate sources.
Where: Mainly liver (90%), some in kidney (10%)
Precursors (raw materials):
- Lactate (from RBCs, exercising muscle)
- Glycerol (from fat breakdown)
- Glucogenic amino acids (especially alanine, glutamine)
- Odd-chain fatty acids → propionyl-CoA
The 3 Irreversible "Roadblocks" of Glycolysis (that gluconeogenesis must bypass):
| Glycolysis Step (irreversible) | Gluconeogenesis Bypass Enzyme |
|---|
| Pyruvate Kinase (PEP → Pyruvate) | Pyruvate Carboxylase + PEPCK (two-step bypass) |
| Phosphofructokinase-1 (F6P → F1,6-BP) | Fructose-1,6-bisphosphatase |
| Glucokinase/Hexokinase (Glucose → G6P) | Glucose-6-phosphatase |
Flow of gluconeogenesis:
Pyruvate
↓ [Pyruvate Carboxylase + BIOTIN] ← KEY STEP
Oxaloacetate (OAA)
↓ [PEPCK - uses GTP]
Phosphoenolpyruvate (PEP)
↓ [several reversible steps]
Fructose-1,6-bisphosphate
↓ [Fructose-1,6-bisphosphatase]
Fructose-6-phosphate
↓
Glucose-6-phosphate
↓ [Glucose-6-phosphatase - in liver ER]
FREE GLUCOSE → released into blood
Sources of Biotin
- Organ meats (liver, kidney)
- Egg YOLK (not white!)
- Nuts, legumes, mushrooms, yeast
- Gut bacteria also synthesize biotin
Absorption of Biotin
- Free biotin is absorbed in small intestine
- Intestinal biotinidase releases protein-bound biotin from food
Why Raw Egg White Causes Deficiency
- Raw egg white contains AVIDIN - a glycoprotein
- Avidin binds biotin with extremely high affinity (Kd ~10⁻¹⁵ M - one of the strongest non-covalent bonds in nature)
- This binding prevents intestinal absorption
- Heat (cooking) denatures avidin → cooked eggs are safe
Energy Requirement of Pyruvate Carboxylase
- Requires ATP (1 ATP consumed per reaction)
- Requires Mg²⁺ as cofactor
- Activated allosterically by Acetyl-CoA (high Acetyl-CoA = need more OAA = activate PC)
PART 5 - Explain Like a Medical Professor
High-Yield Professor Points
Regulation of Pyruvate Carboxylase
Pyruvate Carboxylase is ACTIVATED by Acetyl-CoA - this is a brilliant physiological design:
- When fasting: Fat is broken down → lots of Acetyl-CoA accumulates
- High Acetyl-CoA signals: "We have plenty of fat fuel, now make glucose too"
- Acetyl-CoA activates PC → gluconeogenesis starts
- Result: Blood glucose is maintained during fasting
Without biotin: PC cannot be activated even if Acetyl-CoA is high.
Location Details
- PC reaction occurs inside mitochondria
- OAA cannot cross inner mitochondrial membrane
- OAA is converted to Malate (by mitochondrial malate dehydrogenase using NADH)
- Malate crosses membrane → in cytosol, converted back to OAA
- Cytosolic OAA is acted on by PEPCK (using GTP) → PEP
This clever shuttle also moves NADH reducing equivalents from mitochondria to cytosol (needed for gluconeogenesis).
Pyruvate Carboxylase Deficiency - Clinical Disease
- Inherited (rare genetic): Autosomal recessive
- Presents in neonates with:
- Severe lactic acidosis (pyruvate backs up → lactate)
- Hypoglycemia
- Hyperammonemia
- Brain damage / developmental delay
- Treatment: Biotin supplementation (for acquired), special diet for genetic forms
PEPCK (Option D) - Important Distinctions
PEPCK = Phosphoenolpyruvate Carboxykinase
- Catalyzes: OAA → PEP + CO₂ (uses GTP)
- Does NOT require biotin - it uses GTP
- Is the rate-limiting step of gluconeogenesis in many contexts
- Induced by: Glucagon, glucocorticoids, fasting
- Inhibited by: Insulin
- PEPCK deficiency → hypoglycemia, lactic acidosis (but unrelated to biotin/raw eggs)
Von Gierke Disease (Option A connection)
- Glucose-6-phosphatase deficiency = Glycogen Storage Disease Type I
- Cannot release free glucose from G6P in liver
- Features: Severe hypoglycemia, MASSIVE hepatomegaly (enlarged liver), hyperlipidemia, hyperuricemia, lactic acidosis
- Key clue: Fasting hypoglycemia + huge liver in infant
McArdle Disease (Option B connection)
- Muscle Glycogen Phosphorylase deficiency = GSD Type V
- Cannot break down glycogen in muscles during exercise
- Features: Muscle cramps/pain during exercise, myoglobinuria (dark urine), no lactic acid rise on exercise (classic sign)
- Key clue: Exercise-induced muscle cramps + myoglobinuria + NO lactate rise on forearm ischemic exercise test
PART 6 - Break Down Every Option
Option A: Glucose-6-Phosphatase ❌
What is it?
An enzyme located in the endoplasmic reticulum of liver cells (and kidney). It removes the phosphate group from Glucose-6-Phosphate to release FREE glucose into the bloodstream.
Why is it wrong here?
- It does NOT require biotin
- It is not involved in the pyruvate carboxylase step
- Raw egg whites affect biotin absorption, which has no connection to glucose-6-phosphatase
- G6Pase deficiency is a genetic disease (Von Gierke) - not caused by diet
When would it be the correct answer?
- "Infant with severe fasting hypoglycemia + massively enlarged liver + lactic acidosis + hyperuricemia (gout)"
- "Which enzyme is deficient in Von Gierke disease?"
- "Glycogen Storage Disease Type I - enzyme deficient?"
How to distinguish from pyruvate carboxylase:
- G6Pase = liver/kidney enzyme, diet has no effect, causes hepatomegaly
- PC = mitochondrial enzyme, affected by biotin/raw egg diet, no hepatomegaly
Option B: Glycogen Phosphorylase ❌
What is it?
An enzyme that breaks down glycogen (stored glucose) by cleaving glucose units from the glycogen chain. There are two forms:
- Liver glycogen phosphorylase = releases glucose into blood
- Muscle glycogen phosphorylase (myophosphorylase) = provides fuel for muscle
Why is it wrong here?
- Does NOT require biotin
- Raw eggs have zero effect on glycogen phosphorylase
- McArdle disease (muscle GP deficiency) presents with cramps ONLY during exercise, not simple fatigue
- The question says "fatigue on moderate exercise" not "severe cramps + dark urine"
When would it be the correct answer?
- "A young patient develops painful muscle cramps during exercise with no rise in lactate on ischemic forearm test - enzyme deficient?"
- "GSD Type V - which enzyme?"
- "Myoglobinuria after exercise - which GSD?"
How to distinguish from pyruvate carboxylase:
- GP deficiency: Cramps, myoglobinuria, no lactate rise on exercise test - no dietary link
- PC deficiency: Simple fatigue, hypoglycemia, linked to raw egg/biotin issue
Option C: Pyruvate Carboxylase ✅ CORRECT
What is it?
A mitochondrial enzyme that converts Pyruvate → Oxaloacetate using biotin as cofactor and ATP as energy source. This is the first and committed step of gluconeogenesis.
Why is it correct?
- REQUIRES BIOTIN as its essential cofactor
- Raw egg white → Avidin → blocks biotin → PC has no cofactor → fails
- PC failure → gluconeogenesis fails → blood glucose cannot be maintained during exercise
- Result: Fatigue on moderate exercise = hypoglycemia
Complete chain of logic:
Raw eggs → Avidin → Biotin blocked → PC has no biotin →
Gluconeogenesis fails → Hypoglycemia → Fatigue ✓
Option D: Phosphoenolpyruvate Carboxykinase (PEPCK) ❌
What is it?
An enzyme in the cytosol (and mitochondria) that converts Oxaloacetate → Phosphoenolpyruvate (PEP) using GTP. It is the second step of gluconeogenesis (right after pyruvate carboxylase).
Why is it wrong?
- Does NOT require biotin - uses GTP as its energy/cofactor source
- Not affected by avidin or raw egg consumption
- PEPCK is stimulated by glucagon and cortisol, inhibited by insulin
The subtle TRAP the examiner set:
PEPCK is in the same gluconeogenesis pathway as pyruvate carboxylase! Both enzymes together bypass the pyruvate kinase irreversible step. A student who knows "gluconeogenesis is failing" but doesn't know which enzyme needs biotin might pick PEPCK.
The key differentiator: Biotin cofactor = Pyruvate Carboxylase. NOT PEPCK.
When would PEPCK be the correct answer?
- "Which enzyme is rate-limiting for gluconeogenesis and induced by glucagon?"
- "Which enzyme converts OAA to PEP and uses GTP?"
- "Insulin inhibits which gluconeogenic enzyme at the gene expression level?"
PART 7 - Comparison Table
| Feature | Pyruvate Carboxylase ✅ | Glucose-6-Phosphatase | Glycogen Phosphorylase | PEPCK |
|---|
| Pathway | Gluconeogenesis (Step 1) | Gluconeogenesis (last step) / Glycogenolysis | Glycogenolysis | Gluconeogenesis (Step 2) |
| Substrate → Product | Pyruvate → OAA | G6P → Glucose + Pi | Glycogen → G1P | OAA → PEP |
| Cofactor/Coenzyme | BIOTIN + ATP + Mg²⁺ | None (hydrolase) | Pyridoxal phosphate (B6) | GTP |
| Location in cell | Mitochondria | ER (liver, kidney) | Cytosol | Cytosol + Mitochondria |
| Organ | Liver, Kidney, Muscle | Liver, Kidney, Intestine | Liver + Muscle | Liver, Kidney |
| Activated by | Acetyl-CoA | - | Glucagon, Epinephrine | Glucagon, Glucocorticoids |
| Inhibited by | Low Acetyl-CoA | - | Insulin, Glucose | Insulin |
| Deficiency disease | Pyruvate carboxylase def. (neonatal acidosis) | Von Gierke (GSD I) | McArdle (GSD V) | PEPCK deficiency |
| Key clinical feature | Lactic acidosis, hypoglycemia | Hepatomegaly + severe hypoglycemia | Exercise cramps + myoglobinuria | Hypoglycemia + liver disease |
| Raw egg link? | YES - biotin dependent | No | No | No |
| NEET PG trigger | Raw eggs, biotin deficiency, fatigue | Infant, big liver, fasting hypoglycemia | Exercise cramps, no lactate rise | Insulin inhibits gluconeogenesis |
PART 8 - Memory Tricks
Mnemonic 1: The 4 Biotin Enzymes - "PPAM"
Pyruvate carboxylase
Propionyl-CoA carboxylase
Acetyl-CoA carboxylase
3-Methylcrotonyl-CoA carboxylase
Say it like: "PP-AM" (two P's, then AM)
Mnemonic 2: The Avidin Story
"Avidin is a VILLAIN in raw eggs who STEALS Biotin from your body"
Visual: Imagine a villain named AVID-IN (he's avid/greedy) who snatches your biotin vitamin pill right before you can swallow it.
Mnemonic 3: Pyruvate Carboxylase cofactors
"Biotin ATP Magnesium" = "BAM!" 🔨
Biotin + ATP + Magnesium = BAM (pyruvate gets "BAM"'d into oxaloacetate)
Mnemonic 4: Which enzyme goes with which GSD?
"Von Gierke's Got Gout and a Giant liver" = Glucose-6-Phosphatase (GSD I)
"McArdle Makes Muscles Mad during Marathon" = Muscle Glycogen Phosphorylase (GSD V)
Mnemonic 5: PEPCK cofactor
"PEPCK uses GTP - G for Glucagon loves it"
Glucagon → stimulates PEPCK → makes glucose
Visual Hook: The Raw Egg Chain
🥚 Raw Egg → 🦹 Avidin → 🔒 Locks Biotin →
💔 Pyruvate Carboxylase broken →
🏭 Gluconeogenesis factory shuts →
😓 Fatigue on exercise
PART 9 - Clinical Scenario
Case
A 22-year-old fitness enthusiast visits a gym 6 days a week. He drinks a protein shake every morning made with 6 raw egg whites. He has been doing this for 4 months. He now complains of weakness and fatigue even after mild workouts. He also has a scaly rash around his mouth and eyes, and his hair is thinning. He denies any medications.
Blood tests: Low blood glucose after exercise, low serum biotin, elevated urinary 3-hydroxyisovaleric acid.
What is happening?
He has biotin deficiency caused by chronic raw egg white consumption.
- Avidin in raw eggs chronically blocked biotin absorption
- Over 4 months, biotin stores depleted
- Now all 4 biotin-dependent carboxylases are failing:
- Pyruvate Carboxylase fails → gluconeogenesis impaired → hypoglycemia → fatigue
- 3-Methylcrotonyl-CoA carboxylase fails → elevated 3-hydroxyisovaleric acid in urine
- Acetyl-CoA carboxylase fails → fatty acid synthesis impaired → hair, skin affected
- Skin findings = scaly periorificial dermatitis (around mouth, eyes) - classic biotin deficiency rash
- Alopecia (hair loss) - classic biotin deficiency sign
Diagnosis
- Low serum biotin
- Elevated urinary 3-hydroxyisovaleric acid (functional marker - most sensitive)
- Clinical features: rash + alopecia + neurological fatigue
Management
- Stop raw eggs (cook them!)
- Oral biotin supplementation - 150 mcg/day for acquired deficiency
- Symptoms resolve within weeks
PART 10 - NEET PG Exam Strategy
How to solve this in under 30 seconds:
The 3-second rule:
- See "raw eggs" → immediately think Avidin → Biotin deficiency
- Ask yourself: "Which enzyme from the options needs Biotin?"
- Only ONE of the 4 options needs biotin = Pyruvate Carboxylase
- Mark C. Done.
The Trap the Examiner Set:
Trap 1: The question says "fatigue on moderate exercise" - beginners think of glycogen breakdown diseases (McArdle = Glycogen Phosphorylase). But the KEY differentiator is "RAW EGGS" - McArdle has nothing to do with diet.
Trap 2: PEPCK is in the same pathway (gluconeogenesis). A student who thinks "gluconeogenesis is failing → pick PEPCK" falls into this trap. Remember: PEPCK uses GTP, not biotin.
Trap 3: Glucose-6-phosphatase also affects glucose release, but it's a Von Gierke disease enzyme, has no biotin requirement, and presents in infants with hepatomegaly - not bodybuilders.
How similar questions can be framed:
- "A patient on long-term TPN (IV feeding) develops alopecia and fatigue - enzyme deficient?"
- "Which enzyme requires biotin and activates gluconeogenesis?" → Pyruvate Carboxylase
- "A neonate with lactic acidosis, hypoglycemia, hyperammonemia - enzyme deficient?" → Pyruvate Carboxylase
- "Avidin binds which vitamin?" → Biotin
- "Which vitamin is deficient in raw egg white consumers?" → Biotin (B7)
- "Biotin is cofactor for how many carboxylases?" → 4
PART 11 - Similar NEET PG Style MCQs
Q1. A patient on prolonged total parenteral nutrition develops alopecia, perioral dermatitis, and fatigue. The enzyme most likely deficient is:
- A) Pyruvate Dehydrogenase
- B) Pyruvate Carboxylase ✅
- C) Lactate Dehydrogenase
- D) Phosphoglycerate kinase
Answer: B - TPN without biotin → biotin deficiency → pyruvate carboxylase fails. Same mechanism as raw eggs, different cause.
Q2. Which of the following enzymes uses GTP as its energy source in gluconeogenesis?
- A) Pyruvate Carboxylase
- B) Glucose-6-Phosphatase
- C) Phosphoenolpyruvate Carboxykinase ✅
- D) Fructose-1,6-Bisphosphatase
Answer: C - PEPCK is the only gluconeogenic enzyme using GTP (not ATP). Pyruvate carboxylase uses ATP.
Q3. A 6-month-old infant presents with severe hypoglycemia, massively enlarged liver, lactic acidosis, and elevated triglycerides. Enzyme deficient:
- A) Glycogen Phosphorylase
- B) Glucose-6-Phosphatase ✅
- C) Pyruvate Carboxylase
- D) Aldolase B
Answer: B - Classic Von Gierke disease (GSD I). Infant + big liver + severe hypoglycemia + lactic acidosis = G6Pase deficiency.
Q4. A 19-year-old gets severe muscle cramps during a 400m race. Post-exercise urine is dark red. Forearm ischemic exercise test shows NO rise in blood lactate. Enzyme deficient:
- A) Pyruvate Carboxylase
- B) Glucose-6-Phosphatase
- C) Phosphoglycerate Kinase
- D) Muscle Glycogen Phosphorylase ✅
Answer: D - McArdle disease (GSD V). Exercise cramps + myoglobinuria (dark urine) + NO lactate rise = muscle GP deficiency. The muscle cannot break down glycogen → no lactate produced.
Q5. Biotin acts as a cofactor by carrying which group?
- A) Methyl group
- B) Carboxyl group (CO₂) ✅
- C) Amino group
- D) Phosphate group
Answer: B - Biotin is the "CO₂ carrier" of the body. It picks up CO₂ and transfers it to substrates in carboxylation reactions.
Q6. Which of the following is NOT a biotin-dependent enzyme?
- A) Acetyl-CoA carboxylase
- B) Propionyl-CoA carboxylase
- C) Pyruvate Carboxylase
- D) Phosphoenolpyruvate Carboxykinase ✅
Answer: D - PEPCK uses GTP, not biotin. All others are the 4 biotin-dependent carboxylases.
Q7. Pyruvate carboxylase is allosterically activated by:
- A) AMP
- B) ATP
- C) Acetyl-CoA ✅
- D) Malonyl-CoA
Answer: C - High Acetyl-CoA (during fasting/fat oxidation) activates PC to push gluconeogenesis forward.
Q8. A patient with biotin deficiency will have elevated urinary levels of which organic acid?
- A) Methylmalonic acid
- B) Pyruvic acid
- C) 3-Hydroxyisovaleric acid ✅
- D) Homocysteine
Answer: C - 3-HIVA is the best functional marker of biotin deficiency. It accumulates because 3-methylcrotonyl-CoA carboxylase (biotin-dependent) cannot work in leucine metabolism.
PART 12 - Final Revision Sheet (One Page)
⚡ BIOTIN DEFICIENCY - RAPID REVISION
The Story in One Line:
Raw egg → Avidin → Blocks Biotin → Pyruvate Carboxylase fails → No Gluconeogenesis → Hypoglycemia → Fatigue
4 Biotin-Dependent Enzymes (PPAM):
- Pyruvate Carboxylase → Gluconeogenesis
- Propionyl-CoA Carboxylase → Odd-chain FA / Val, Ile, Met catabolism
- Acetyl-CoA Carboxylase → Fatty acid synthesis
- 3-Methylcrotonyl-CoA Carboxylase → Leucine catabolism
Pyruvate Carboxylase Quick Facts:
- Cofactors: Biotin + ATP + Mg²⁺ (BAM!)
- Location: Mitochondria (liver, kidney)
- Reaction: Pyruvate → OAA
- Activated by: Acetyl-CoA
- Purpose: Step 1 of gluconeogenesis + replenish TCA cycle
PEPCK vs PC:
| Pyruvate Carboxylase | PEPCK |
|---|
| Cofactor | BIOTIN + ATP | GTP |
| Reaction | Pyruvate → OAA | OAA → PEP |
| Raw egg link | YES | No |
Key Disease Associations:
| Disease | Enzyme | Clue |
|---|
| Von Gierke (GSD I) | Glucose-6-Phosphatase | Baby + big liver + severe hypoglycemia |
| McArdle (GSD V) | Muscle Glycogen Phosphorylase | Exercise cramps + myoglobinuria + no lactate |
| Biotin deficiency | Pyruvate Carboxylase (+ 3 others) | Raw eggs + rash + alopecia + fatigue |
Urine Marker of Biotin Deficiency:
- 3-Hydroxyisovaleric acid ↑ (most sensitive)
Treatment:
- Acquired: 150 mcg biotin/day
- Biotinidase deficiency: 5-10 mg biotin/day
One Day Before Exam - Remember:
- ✅ Raw egg = Avidin = Biotin deficiency = Pyruvate Carboxylase
- ✅ PEPCK uses GTP not biotin
- ✅ 4 biotin enzymes = PPAM
- ✅ McArdle = exercise cramps + no lactate rise (NOT biotin)
- ✅ Von Gierke = big liver + severe hypoglycemia in baby (NOT biotin)
- ✅ Biotin marker in urine = 3-Hydroxyisovaleric acid
PART 13 - Difficulty Level
⭐⭐ Moderate
Why moderate?
- The raw egg → avidin → biotin link is a well-known fact
- The connection to pyruvate carboxylase (not PEPCK) requires knowing which enzymes use biotin
- The main challenge is distinguishing pyruvate carboxylase from PEPCK (both are in gluconeogenesis)
- Knowing the cofactor (biotin vs GTP) is the discriminating knowledge
A student who only memorized "gluconeogenesis" without knowing cofactors would get it wrong. That's what makes it moderate, not easy.
PART 14 - If You Remember ONLY 5 Things Forever
1. Raw egg white → Avidin → Steals Biotin → Pyruvate Carboxylase fails
2. Pyruvate Carboxylase cofactors = BAM (Biotin + ATP + Mg²⁺)
3. PEPCK uses GTP (NOT Biotin) - second step of gluconeogenesis bypass
4. 4 Biotin enzymes = PPAM (Pyruvate, Propionyl, Acetyl, 3-Methylcrotonyl carboxylases)
5. McArdle = Muscle cramps + no lactate rise on exercise (glycogen phosphorylase, NOT biotin)
Sources: Lippincott's Illustrated Reviews Biochemistry 8th Ed; Tietz Textbook of Laboratory Medicine 7th Ed; Harrison's Principles of Internal Medicine 22E; Robbins Pathology; Basic Medical Biochemistry 6th Ed