Cervicogenic headaches its pathology and muscle responsible and physiotherapy treatment in deatil
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cervicogenic headache" AND physiotherapy
Searching the Web
cervicogenic headache pathology muscles physiotherapy treatment 2024
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11063809
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the detailed response.
Cervicogenic Headache (CGH): Pathology, Muscles Involved, and Physiotherapy Treatment
Definition and Background
Cervicogenic headache (CGH) is a secondary headache - one that originates from pathology in the cervical spine and its related structures, with pain referred to the head. The term was introduced by Sjaastad and colleagues in 1983. The International Headache Society published its first diagnostic criteria in 1998, revised in 2004.
CGH is frequently misdiagnosed as migraine due to significant symptom overlap. It is estimated to affect 0.4-4% of the general population and up to 17.8% of chronic headache sufferers.
Pathology and Mechanism
Anatomical Basis
The core mechanism rests on the trigemino-cervical complex (TCC). Primary sensory afferents from cervical roots C1, C2, and C3 converge with afferents from the occiput and trigeminal afferents onto the same second-order neurons in the trigeminal nucleus caudalis of the upper cervical spinal cord. This anatomical convergence means that:
- Pain originating in the upper cervical structures is referred to the head and face
- Head pain can spread from occipital regions to trigeminal territories (frontal, temporal, orbital regions)
This is why, as Bradley and Daroff's Neurology explains, "the referral of pain observed in cervicogenic headache and migraine reflects the convergence of trigeminal and cervical afferents onto the same neurons in the trigeminal-cervical complex."
Pain-Generating Structures (Sources of CGH)
Per Scott-Brown's Otorhinolaryngology and Bradley & Daroff's Neurology, pain may arise from:
- Zygapophyseal (facet) joints - especially C2/C3 (most common), also atlanto-occipital and atlanto-axial joints
- Intervertebral discs (C2-C3, C3-C4)
- Upper cervical muscles and ligaments - suboccipital muscles, semispinalis capitis, splenius capitis, upper trapezius, SCM
- Apophyseal (facet) arthropathy - degeneration of upper cervical facets
- Greater and lesser occipital nerves - entrapment or irritation
- C2 dorsal root entrapment
- Atlantoaxial region pathology (e.g., rheumatoid arthritis)
- Ligamentum flavum calcification, hypertrophy of posterior longitudinal ligament
Central Sensitization
Prolonged nociceptive input from cervical structures leads to central sensitization within the trigemino-cervical complex. Sensitized neurons develop:
- Lower thresholds for activation
- Increased spontaneous activity
- Expanded receptive fields
This explains why CGH can produce widespread referred pain, autonomic features (nausea, photophobia), and why it can mimic migraine closely.
Muscles Responsible
The following muscles are primary contributors to CGH, either as direct pain generators (via trigger points, spasm, or myofascial pathology) or as secondary responders to underlying joint/nerve dysfunction:
Primary Muscles
| Muscle | Role in CGH |
|---|---|
| Suboccipital group (rectus capitis posterior major/minor, obliquus capitis inferior/superior) | Directly innervated by C1-C2; trigger points refer pain to the occiput and over the head; restrict upper cervical segmental motion (C0-C1, C1-C2) |
| Semispinalis capitis | Major C2/C3 innervated extensor; trigger points refer pain to the occiput, temporal, and frontal regions |
| Splenius capitis and cervicis | Trigger points refer pain unilaterally to the ipsilateral occiput and top of head |
| Upper trapezius | Trigger points in the upper fibers refer pain to the temple and retro-orbital area; consistently found to be stiff and hypertonic in CGH patients |
| Sternocleidomastoid (SCM) | Trigger points refer pain to the occiput, vertex, eye, and forehead; can mimic cluster headache |
| Levator scapulae | Secondary contributor; increased tension with prolonged poor posture |
| Deep neck flexors (longus colli, longus capitis) | Weakness leads to forward head posture and compensatory hyperactivation of posterior neck muscles, loading the upper cervical joints |
Why Muscle Dysfunction Matters
Weakness of the deep cervical flexors is a hallmark finding in CGH. These muscles (longus colli, longus capitis) are postural stabilizers of the cervical spine. Their impairment:
- Increases compressive load on posterior cervical structures (facets, discs)
- Forces the superficial global muscles (SCM, upper trapezius) into compensatory overactivation
- Perpetuates joint irritation and trigger point formation
Clinical Features
Key distinguishing features from migraine:
- Pain typically unilateral, starting in the neck/occiput and radiating to the forehead, temple, or orbital region
- Triggered or aggravated by neck movement or sustained neck postures
- Constant pain with episodic exacerbations (unlike episodic migraine)
- Tenderness over the greater/lesser occipital nerves, cervical facet joints, and upper/middle cervical muscles
- Does not respond to migraine-specific medications (triptans)
- History of head or neck trauma is common
May also have: nausea, vomiting, photophobia, phonophobia, blurred vision (making differentiation from migraine difficult).
Physiotherapy Treatment (Detailed)
Physiotherapy is the cornerstone of non-pharmacological CGH management. Evidence consistently supports a multimodal approach.
1. Manual Therapy
A. High-Velocity Low-Amplitude (HVLA) Spinal Manipulation
- Applied to upper cervical segments (C1-C2, C2-C3) and/or thoracic spine
- Reduces joint restriction, neurophysiological pain modulation via descending inhibitory pathways
- Evidence: Nuñez-Cabaleiro & Leirós-Rodríguez (2022, Headache) systematic review confirmed effectiveness in reducing headache frequency and intensity
B. Joint Mobilization (Maitland/Mulligan techniques)
- Grades I-IV cervical mobilization, especially at C2-C3 and C0-C1 levels
- Mulligan concept: Sustained Natural Apophyseal Glides (SNAGs) at upper cervical segments - patient performs active movement while therapist applies a gliding force; particularly effective when neck movement reproduces the headache
- Less risk than HVLA; appropriate for patients with contraindications to manipulation
- Systematic review (Bini et al., 2022, Chiropr Man Therap) showed combined manual therapy + exercise significantly reduces headache intensity and frequency
C. Soft Tissue Techniques / Myofascial Release
- Trigger point therapy targeting suboccipital muscles, upper trapezius, SCM, semispinalis capitis
- Suboccipital inhibition/release: sustained gentle pressure at the suboccipital triangle to release the rectus capitis and oblique capitis muscles - directly reduces compressive load on upper cervical structures
- A 2024 meta-analysis (Lu et al., Pain Res Manag, PMID 38585645) confirmed myofascial release significantly improves CGH
D. Muscle Energy Techniques (METs)
- Patient contracts the restricted muscle isometrically against the therapist's counterforce, followed by passive stretch
- Targets: suboccipital muscles, SCM, upper trapezius, levator scapulae
- Restores full segmental ROM and reduces muscle hypertonicity
2. Exercise Therapy
A. Deep Neck Flexor (DNF) Training - Craniocervical Flexion Exercise (CCFE)
- Targets longus colli and longus capitis using a pressure biofeedback unit (Stabilizer) or ultrasound feedback
- Patient performs nodding motion (craniocervical flexion) at 5 progressive pressure levels (20-30 mmHg)
- Considered the single most evidence-based exercise for CGH
- Improves neuromuscular control, reduces compressive load on upper cervical joints
- Jull et al.'s landmark RCT demonstrated that DNF training combined with manual therapy is superior to either intervention alone
B. Cervical Stabilization and Postural Exercises
- Progressive resistance exercises for deep and superficial cervical extensors
- Targets: semispinalis cervicis, multifidus (cervical), longissimus capitis
- Addresses the motor control impairment seen in CGH - reduced activation of cervical multifidus and altered muscle recruitment patterns
C. Scapular and Thoracic Exercises
- Serratus anterior and lower trapezius strengthening to normalize scapular position
- Thoracic extension exercises to counteract forward head posture
- A 2024 RCT (referenced in Nature Index) combining cervical mobilization with clinical Pilates showed greater improvements in headache intensity and muscle stiffness (suboccipital and trapezius) than mobilization alone
D. Cervical Stretching
- Suboccipital stretch, cervical lateral flexion and rotation stretches
- Particular emphasis on stretching upper trapezius and SCM
- Neural mobilization/upper cervical neurodynamic techniques for greater occipital nerve entrapment
E. Aerobic Exercise
- Low-impact aerobic conditioning (walking, swimming, cycling) reduces central sensitization through endogenous opioid release and improved cardiovascular function
3. Dry Needling
- Insertion of fine needles into active myofascial trigger points in suboccipital muscles, upper trapezius, SCM, semispinalis capitis
- Reduces local trigger point irritability, improves muscle extensibility
- The APTA 2024 network meta-analysis identified spinal manipulation combined with dry needling as one of the most effective intervention combinations for reducing CGH intensity and frequency
4. Postural Correction and Ergonomics
- Assessment and correction of forward head posture (FHP) - the most common biomechanical perpetuating factor
- For every 1 inch of forward head translation, the effective weight on the cervical spine increases by approximately 10 lbs
- Ergonomic modifications: workstation setup, screen height, chair support
- Sleep posture: appropriate pillow height to maintain neutral cervical alignment
5. Electrophysical Agents (Adjunctive)
- TENS (Transcutaneous Electrical Nerve Stimulation): Pain modulation via gate control; applied to upper cervical paraspinals or over the greater occipital nerve
- Therapeutic ultrasound: Deep tissue heating to suboccipital and upper cervical muscles
- Low-level laser therapy (LLLT): Reduces inflammation and trigger point activity in superficial cervical muscles
- Heat therapy: Reduces muscle spasm and improves tissue extensibility before manual therapy
6. Taping Techniques
- Kinesio taping of upper trapezius and cervical paraspinals for muscle facilitation/inhibition
- Postural taping to facilitate thoracic extension and correct FHP
7. Education and Self-Management
- Pain neuroscience education (PNE): explaining central sensitization mechanisms reduces fear-avoidance and improves outcomes
- Home exercise program: DNF exercises, cervical stretching, posture correction
- Activity modification and pacing strategies
- Relaxation techniques: diaphragmatic breathing, progressive muscle relaxation
Evidence Summary
| Intervention | Evidence Level | Effect |
|---|---|---|
| Manual therapy (manipulation + mobilization) | Systematic Review (Nuñez-Cabaleiro 2022) | Reduces frequency and intensity |
| Manual therapy + exercise (combined) | Meta-Analysis (Bini et al. 2022) | Superior to either alone |
| Myofascial release | Meta-Analysis (Lu et al. 2024, PMID 38585645) | Significant improvement |
| Dry needling + manipulation | Network meta-analysis (APTA 2024) | Most effective combination |
| DNF training (Craniocervical flexion) | Multiple RCTs | Reduces disability and frequency |
| Spinal manipulation alone | Systematic Review | Effective vs sham |
| Mulligan SNAGs | Systematic Review (Aslyuce 2022) | Positive effects on CGH |
Physiotherapy Clinical Pathway
- Assessment: C0-C3 segmental mobility testing, DNF endurance test, postural assessment, trigger point palpation, provocative testing (manual pressure reproducing headache), diagnostic nerve blocks if needed
- Acute phase (weeks 1-3): Manual therapy (mobilization/manipulation), soft tissue release, pain education, TENS/heat
- Rehabilitation phase (weeks 3-8): DNF training, cervical stabilization exercises, postural correction, ergonomic advice, Mulligan SNAGs
- Maintenance phase (8+ weeks): Progressive loading, aerobic conditioning, self-management, return to activity
Key References
- Bradley and Daroff's Neurology in Clinical Practice - Section on Cervicogenic Headache, p. 1101
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Cervical Spine Degenerative Disease and Cervicogenic Headache, p. 1309
- Adams and Victor's Principles of Neurology - Headache Related to Diseases of the Cervical Spine, p. 208
- Nuñez-Cabaleiro P & Leirós-Rodríguez R. Effectiveness of manual therapy in CGH: Systematic review. Headache. 2022 [PMID: 35294051]
- Bini P et al. Effectiveness of manual and exercise therapy on CGH: systematic review and meta-analysis. Chiropr Man Therap. 2022 [PMID: 36419164]
- Lu Z et al. Myofascial Release for CGH: Systematic Review and Meta-Analysis. Pain Res Manag. 2024 [PMID: 38585645]
- Reynolds B et al. Manual physical therapy for neck disorders: umbrella review. J Man Manip Ther. 2025 [PMID: 39607420]
Vertigo and physiotherapy exercises in detail with doses
Reading File
Finding Sources
Finding Sources
Searching PubMed
"vestibular rehabilitation" AND vertigo AND exercises
Searching the Web
vertigo physiotherapy exercises BPPV vestibular rehabilitation dosage 2024 2025
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative content. Let me compile the full detailed response.
Vertigo: Types, Pathology, and Physiotherapy Exercises with Doses
1. What is Vertigo?
Vertigo is the false sensation of movement - the illusion that the self or the environment is spinning, rotating, or tilting - caused by a mismatch between vestibular, visual, and proprioceptive sensory inputs. It is distinct from general dizziness, lightheadedness, or presyncope.
Classification:
- Peripheral vertigo: Arises from the inner ear (labyrinth) or vestibular nerve (CN VIII). Generally more intense, with a latency before nystagmus onset, nystagmus that fatigues, and prominent nausea.
- Central vertigo: Arises from brainstem or cerebellum. Often milder spinning sensation, nystagmus begins immediately without latency, does NOT fatigue, may have vertical nystagmus.
2. Common Causes of Vertigo
| Cause | Characteristics |
|---|---|
| BPPV (Benign Paroxysmal Positional Vertigo) | Brief (<1 min) episodes triggered by head position change |
| Vestibular neuritis | Acute severe vertigo lasting days; no hearing loss |
| Labyrinthitis | Like neuritis but WITH hearing loss |
| Meniere's disease | Recurrent attacks: vertigo + tinnitus + fluctuating hearing loss + aural fullness |
| Vestibular migraine | Episodic vertigo (minutes to hours) with migraine features |
| Central (cerebellar/brainstem) | Stroke, MS, tumor - no fatigue of nystagmus |
3. Pathophysiology
BPPV - the most common cause of vertigo - results from calcium carbonate crystals (otoconia/otoliths) dislodged from the utricular macula migrating into one of the semicircular canals (most commonly the posterior canal in 80-90% of cases). When the head moves, gravity causes these free-floating particles to move within the canal, creating abnormal endolymph flow and cupular deflection, generating nystagmus and vertigo (Harrison's Principles of Internal Medicine, 22nd ed., p. 207).
Vestibular neuritis/hypofunction: Inflammation (often viral) of the vestibular ganglion/nerve causes sudden unilateral loss of vestibular input. The asymmetric tonic firing between the two labyrinths produces the sensation of rotation toward the affected side and compensatory nystagmus.
Central vestibular compensation - the principle behind all vestibular rehabilitation: After a peripheral lesion, the CNS undergoes neuroplastic adaptation through three main mechanisms:
- Adaptation - the vestibulo-ocular reflex (VOR) gain is recalibrated
- Habituation - repeated exposure to provocative stimuli reduces CNS response
- Sensory substitution - the CNS learns to rely on visual and proprioceptive inputs to substitute for impaired vestibular function
4. Physiotherapy (Vestibular Rehabilitation) - Full Detail with Doses
Vestibular rehabilitation was pioneered by Cooksey and Cawthorne in the 1940s for post-operative dizziness. Modern programs are individualized based on diagnosis, as established by Cummings Otolaryngology.
A. BPPV - Canalith Repositioning Maneuvers (CRMs)
These are the primary treatment for BPPV and work by using gravity to move displaced otoconia out of the semicircular canals back into the vestibule.
1. Epley Maneuver (Modified) - For Posterior Canal BPPV
Most used and most evidence-supported maneuver. Success rate: 50-90% per single session; up to 90%+ with repetition.
Here is the step-by-step procedure (illustrated below from Harrison's Principles of Internal Medicine, 22nd ed.):
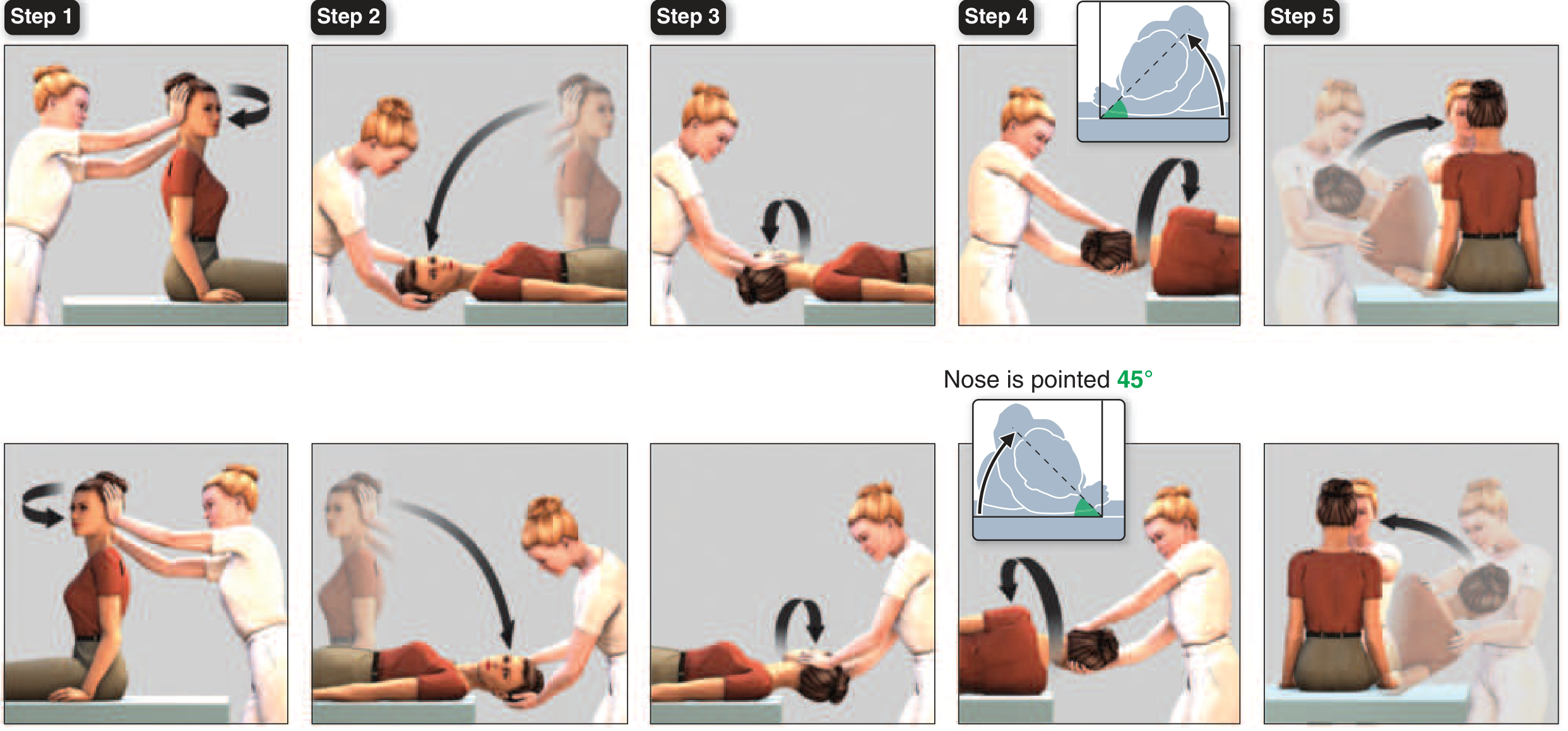
For RIGHT posterior canal BPPV:
| Step | Position | Hold Time |
|---|---|---|
| 1 | Patient sits upright, head turned 45° toward the RIGHT (affected) ear | Briefly |
| 2 | Therapist supports head; patient lies back rapidly to supine with head extended 20-30° below the table edge (head still turned 45° right) - Dix-Hallpike position. Wait for nystagmus. | 30 seconds (or until nystagmus stops) |
| 3 | Without lifting the head, rotate it 90° to the LEFT (nose now points left at 45°) | 30 seconds |
| 4 | Roll the entire body to the left side, simultaneously rotating the head another 90° so the nose points 45° downward toward the floor | 30 seconds |
| 5 | Patient is slowly brought to sitting upright | Rest briefly, then repeat to confirm resolution |
Dose: Repeat maneuver until no nystagmus is elicited. Typically 1-3 repetitions per session. One session is often sufficient; if not, repeat at the next visit.
Post-maneuver instructions (traditional): Some clinicians advise patients to remain upright for 48 hours and avoid sleeping on the affected side for 1-2 days to prevent re-entry of debris into the canal. However, recent evidence does not firmly support strict post-maneuver positioning restrictions.
For LEFT posterior canal BPPV: All directions are mirrored.
2. Semont (Liberatory) Maneuver - For Posterior Canal BPPV
Alternative to Epley, with similar efficacy. Preferred when patient has cervical spine restrictions.
| Step | Position | Hold Time |
|---|---|---|
| 1 | Patient sits upright on the edge of the table, head turned 45° AWAY from the affected ear | Briefly |
| 2 | Rapidly move the patient to lie on the side of the AFFECTED ear (the one causing vertigo), with head maintained in the rotated position | 30 seconds (or until nystagmus resolves) |
| 3 | Rapidly swing the patient (in one fast, sweeping motion) to lie on the OPPOSITE side, keeping the head in the same relative position (nose now points toward the floor) | 30 seconds |
| 4 | Slowly return to seated upright | - |
Dose: 1-3 repetitions per session. Repeat sessions as needed over 1-2 weeks.
3. Horizontal Canal BPPV - Log Roll (Barbecue/Lempert Maneuver)
For the less common horizontal canal variant. Nystagmus is horizontal and changes direction with each side.
| Step | Position | Hold Time |
|---|---|---|
| 1 | Patient lies supine, head turned toward the affected ear | 30 seconds |
| 2 | Turn head to face straight up (supine) | 30 seconds |
| 3 | Turn head 90° toward the UNAFFECTED ear | 30 seconds |
| 4 | Roll body and head further so patient is face-down (prone) | 30 seconds |
| 5 | Roll to lie on unaffected side | 30 seconds |
| 6 | Return to sitting | - |
Alternatively, forced prolonged positioning: lying on the UNAFFECTED side for 12 hours can resolve geotropic horizontal canal BPPV in many cases.
4. Brandt-Daroff Exercises - For BPPV (Habituation-Based)
Designed to habituate the CNS to the provocative position and can also mechanically dislodge debris. Used as a home exercise or as adjunct when repositioning maneuvers are not fully effective.
Technique:
- Start in sitting position on the edge of a bed
- Turn head 45° toward the affected side
- Rapidly lie down sideways onto the AFFECTED ear (body goes down to the opposite side) - head remains turned 45° up relative to the bed
- Hold until vertigo resolves + an additional 30 seconds (minimum)
- Return to sitting, wait until dizziness subsides
- Turn head 45° toward the OTHER side, lie down on the OTHER side
- Hold 30 seconds, return to sitting
Dose:
- 5-10 repetitions per set
- 3 sets per day (morning, afternoon, evening)
- If severe nausea: reduce to 3 repetitions × 3/day until tolerance improves
- Continue until 2 consecutive days with no vertigo
- Typical duration: 2 weeks
Evidence: A 2024 systematic review (Alashram AR, Eur Arch Otorhinolaryngol, PMID 38341824) confirmed Brandt-Daroff exercises are effective for BPPV, though repositioning maneuvers remain superior.
B. Vestibular Adaptation Exercises (VOR Rehabilitation)
Used primarily for unilateral vestibular hypofunction (UVH) - after vestibular neuritis, labyrinthitis, acoustic neuroma resection, or chronic uncompensated vestibular loss. These exercises drive neuroplastic VOR recalibration through retinal slip signals.
Recovery time: 6-8 weeks average with active vestibular rehabilitation.
1. VOR X1 (Times 1) - Gaze Stabilization
Goal: Improve the vestibulo-ocular reflex gain and reduce oscillopsia (blurred vision with head movement).
Technique:
- Patient holds a business card or a fixed target (letter/word) at arm's length
- Focuses on the target
- Oscillates the head horizontally (left-right) as fast as possible while keeping the letter clear and in focus
- If target blurs, the patient slows down
- Then repeat in the vertical plane (up-down)
Starting Dose:
- 1-2 minutes per direction (horizontal + vertical)
- 3 times per day
- Target must remain in focus - the key requirement
Progression:
- Increase to 5 minutes per direction
- Add a distracting background (checkerboard, venetian blinds pattern behind the card)
- Vary head speed and amplitude
- Progress from sitting → standing → walking
2. VOR X2 (Times 2) - Advanced Gaze Stabilization
Goal: Greater VOR gain improvement than X1.
Technique:
- Same as X1 but the target moves in the OPPOSITE direction to the head
- Head moves right → target moves left; head moves left → target moves right
- Eyes must keep focus on the moving target despite double the retinal demand
Dose:
- Begin only after X1 is well tolerated
- 1-3 minutes × 3/day
- Progress in the same manner as X1
3. Imaginary Target (Head Impulse) Exercise
For patients who cannot tolerate physical target tracking:
- Patient closes eyes, imagines a fixed target
- Rapidly rotates head side to side for 1-2 minutes
- Builds VOR pathway independent of visual input
C. Habituation Exercises (Cawthorne-Cooksey Exercises)
Used when specific movements or positions consistently provoke dizziness. The principle is controlled, repeated exposure to the provocative stimulus, causing the brain to progressively reduce its response. Used for vestibular neuritis, chronic vestibular dysfunction, and post-concussion vestibular symptoms.
The classic Cawthorne-Cooksey program progresses through three stages:
Stage 1 - Lying Down (Bed Exercises)
| Exercise | Repetitions | Frequency |
|---|---|---|
| Eye movements: up-down, side-side (slow then fast) | 5-10 reps each direction | 3-4×/day |
| Eye movements: focus on moving finger near to far (20 cm to arm's length) | 10 reps | 3-4×/day |
| Head movements: bend forward, backward, side-to-side (slow, then fast - eyes open, then closed) | 5 reps each, slowly increasing | 3-4×/day |
| Head rotation (ear to shoulder) | 5-10 reps | 3-4×/day |
Hold each position that provokes dizziness for 20-30 seconds. The dizziness should habituate.
Stage 2 - Sitting (Chair Exercises)
| Exercise | Repetitions | Frequency |
|---|---|---|
| All Stage 1 eye and head movements | Same dosing | 3-4×/day |
| Shoulder shrugging and circling | 10 reps | 3×/day |
| Bending forward and picking up objects from the floor | 10 reps | 3×/day |
| Head turning side to side with a target (gaze stabilization) | 1-2 min | 3×/day |
Stage 3 - Standing and Gait Exercises
| Exercise | Repetitions/Duration | Frequency |
|---|---|---|
| Standing feet together, eyes open then closed (Romberg) | 30 seconds each | 3-5×/day |
| Tandem stance (heel-toe) eyes open then closed | 20-30 seconds | 3×/day |
| Single-leg stance eyes open then closed | 10-20 seconds each leg | 3×/day |
| Walking across the room eyes open (then closed against a wall for safety) | 10 passes | 3×/day |
| Walking with head turning side to side (VOR-gait integration) | 2-5 minutes | 3×/day |
| Turning around while walking (180° turns) | 5-10 turns | 3×/day |
| Throwing a ball from hand to hand while walking | 2-3 minutes | 2×/day |
| Walking on foam/uneven surfaces | 2 minutes | 2×/day |
| Stair climbing | 2-3 flights | Daily |
General Dose for Cawthorne-Cooksey: Each exercise should be performed to the point of mild-to-moderate symptom provocation (rated 2-5/10 on dizziness scale). Symptoms should resolve within minutes of stopping. If symptoms persist >20 minutes after exercise, reduce intensity.
D. Balance and Postural Control Exercises
Used across all vestibular diagnoses to reduce fall risk and improve functional stability.
Modified CTSIB (Clinical Test of Sensory Integration in Balance)
Progressively challenges the three sensory systems (vestibular, visual, proprioceptive):
| Condition | Surface | Vision | Challenge Level |
|---|---|---|---|
| 1 | Firm | Eyes open | Easy (all three systems) |
| 2 | Firm | Eyes closed | Removes vision |
| 3 | Firm | Visual conflict (dome) | Disrupts vision |
| 4 | Foam | Eyes open | Removes proprioception |
| 5 | Foam | Eyes closed | Removes vision + proprioception |
| 6 | Foam | Visual conflict | Maximum challenge |
Dose: Each condition for 20-30 seconds, repeated 3 times per condition. Progress from condition 1 to 6 over weeks.
Weight Shifting and Perturbation Training
- Anterior-posterior and mediolateral weight shifts on stable and unstable surfaces
- Dose: 10-15 repetitions, 2-3 sets, 3×/day
E. Gait Rehabilitation Exercises
Specifically for patients with functional gait impairment from chronic vestibular dysfunction:
| Exercise | Dose |
|---|---|
| Walking with head turns (horizontal then vertical) | 5-10 minutes, 2-3×/day |
| Tandem (heel-toe) walking | 3-5 passes × 3 sets/day |
| Walking with eyes closed (near a wall for safety) | 5-10 passes × 2/day |
| Obstacle course walking | 5-10 minutes/session, daily |
| Figure-of-8 walking | 5 circles × 3 sets/day |
| Dual-task gait (e.g., counting backward while walking) | 2-5 minutes/session |
5. Exercise Progression Principles
From Cummings Otolaryngology and VestibularFirst guidelines (2025):
- Change one variable at a time (surface, speed, head movement, cognitive load)
- Progress when symptoms are brief and recover quickly - not when they are prolonged beyond 20 minutes
- Start with stable surface → foam → uneven ground
- Start seated → standing → walking → dynamic tasks
- Eyes open → eyes closed → visual conflict environments
- Single task → dual task (cognitive + motor simultaneously)
6. Diagnosis-Specific Program Summary
| Condition | Primary Intervention | Duration |
|---|---|---|
| BPPV (posterior canal) | Epley or Semont maneuver | 1-3 sessions, with home Brandt-Daroff ×3/day ×2 weeks |
| BPPV (horizontal canal) | Log roll / barbecue maneuver | 1-3 sessions |
| Vestibular neuritis (acute) | Rest 24-48h then VR begins: X1 VOR exercises + Cawthorne-Cooksey | 6-8 weeks |
| Unilateral hypofunction (chronic) | VOR X1/X2 + gaze stability + balance training | 8-12 weeks |
| Bilateral hypofunction | Balance/gait training; NO habituation exercises (no functional vestibular system to habituate) | Long-term/lifelong |
| Meniere's disease (stable phase) | Sensory substitution + fall prevention training | Individualized |
| Vestibular migraine | VR (2026 systematic review PMID 41840297 confirms efficacy) + migraine prophylaxis | 8-12 weeks |
| Central vertigo (post-stroke) | Task-specific gait + dual-task training; caution with VOR exercises | 12+ weeks |
7. Contraindications / Precautions
- Acute BPPV during a vertigo episode: wait until acute phase (nausea/vomiting) passes before rehabilitation
- Unstable or actively progressing central lesion: avoid aggressive VOR exercises until stabilized
- Cervical spine instability: modify or avoid Epley/Semont - use Brandt-Daroff instead
- Vestibular suppressant medications (diazepam, meclizine): reduce or stop before VR - they delay CNS compensation by suppressing the very asymmetric signal needed for recalibration (Cummings Otolaryngology)
- Meniere's disease (unstable/fluctuating phase), superior canal dehiscence, perilymphatic fistula: may NOT benefit from VR and require specialist management first
8. Outcome Measures Used
- Dizziness Handicap Inventory (DHI) - 25-item self-report
- Activities-Specific Balance Confidence (ABC) Scale - fall fear
- Dynamic Gait Index (DGI) - gait with head turns
- Timed Up and Go (TUG) - functional mobility
- Video Head Impulse Test (vHIT) - objective VOR gain
Key References
- Harrison's Principles of Internal Medicine, 22nd ed. - BPPV and Epley Maneuver, p. 207
- Cummings Otolaryngology Head and Neck Surgery - Vestibular Rehabilitation, p. 3262-3264
- Shambaugh Surgery of the Ear - Physical Therapy Intervention in Vestibular Disorders, p. 334-336
- Neuroanatomy through Clinical Cases, 3rd ed. - Dizziness and Vertigo, p. 556
- Scott-Brown's Otorhinolaryngology Vol 2 - Vestibular Rehabilitation Management, p. 8838
- Alashram AR. Brandt-Daroff exercises in BPPV: systematic review. Eur Arch Otorhinolaryngol. 2024 [PMID: 38341824]
- Sfakianaki I et al. Vestibular Rehabilitation in Vestibular Migraine: Systematic Review. J Assoc Res Otolaryngol. 2026 [PMID: 41840297]
- Joshi D et al. Gans repositioning maneuver for posterior canal BPPV: meta-analysis. Eur Arch Otorhinolaryngol. 2022 [PMID: 35460377]
This is a shared conversation. Sign in to Orris to start your own chat.