Necrotising enterocolitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"necrotizing enterocolitis"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative information from multiple major textbooks. Let me compile the full response.
Necrotising Enterocolitis (NEC)
Definition and Epidemiology
Necrotising enterocolitis (NEC) is the most common gastrointestinal surgical emergency in neonates. It is a devastating inflammatory condition causing intestinal necrosis, predominantly affecting premature infants.
- Affects 1-5% of all NICU admissions and 4-13% of very-low-birth-weight (VLBW) infants (<1500 g)
- Incidence is inversely proportional to gestational age - peak incidence at ~32 weeks corrected gestational age
- Approximately 2,500 cases per year in the United States (Robbins Pathologic Basis of Disease)
- Mortality: 10-30% overall; up to 50% in infants requiring surgery
- Occurs in about 10% of preterm babies on NICUs; virtually always after initiation of feeds (Bailey & Love's Surgery, 28th Ed.)
Pathophysiology
The exact aetiology remains incompletely understood. It is now accepted that NEC is not a single disease entity but a multifactorial condition. The three key pillars are:
Pathophysiology Diagram (Fischer's Mastery of Surgery)
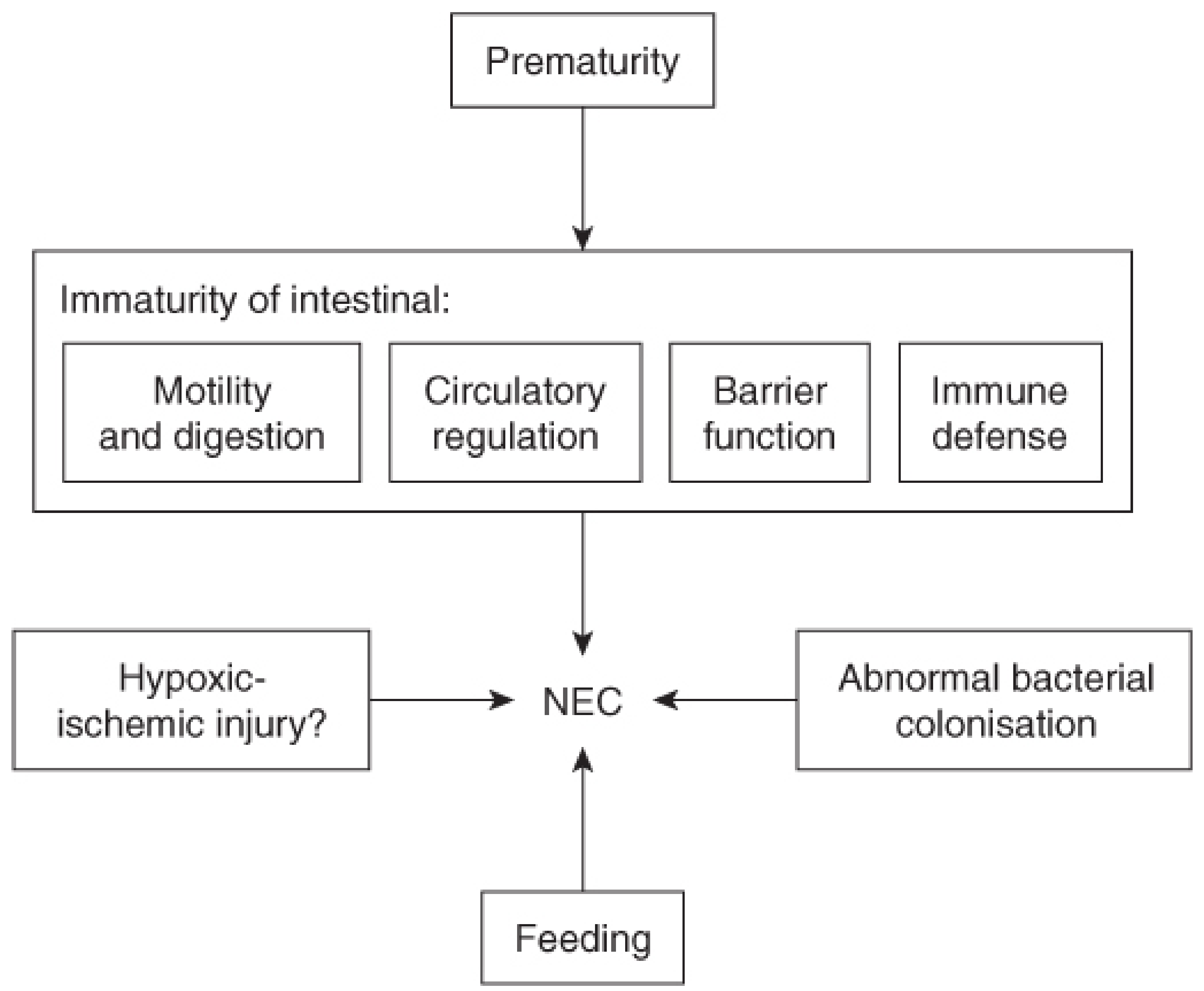
1. Intestinal immaturity (Robbins Basic Pathology):
- Immature mucosal barrier and immune system
- Poor motility and digestion
- Impaired circulatory regulation
2. Dysbiosis / abnormal bacterial colonisation:
- Alterations in the gut microbiome with overgrowth of pathogenic bacteria
- TLR4 (Toll-like receptor 4) activation on gut mucosa increases mucosal ischaemia in response to pathogenic bacteria
- No single bacterial pathogen has been definitively linked
3. Exaggerated inflammatory response:
- Release of pro-inflammatory cytokines and chemokines
- Platelet-activating factor (PAF) promotes enterocyte apoptosis, compromises tight junctions, and increases mucosal permeability
- ET-1 (endothelin-1) causes vasoconstriction; relative deficiency of NO (nitric oxide) contributes to ischaemia
- Once mucosal barrier breaks down: transluminal bacterial migration → vicious cycle of inflammation → necrosis → sepsis → shock
Additional proposed mechanism: A maladaptive "diving reflex" (hypoxia shunting blood from splanchnic to cerebral circulation) was an earlier hypothesis; now largely abandoned but ischaemia-reperfusion injury models continue to support some ischaemic component (Yamada's Gastroenterology, 7th Ed.).
Risk Factors
| Factor | Detail |
|---|---|
| Prematurity | Single most significant risk factor |
| Low birth weight | Especially VLBW (<1500 g) |
| Enteral feeding | NEC almost exclusively occurs after feeds; formula > breast milk |
| Antenatal indomethacin tocolysis | Controversial; possibly associated with early-onset NEC (adjusted OR ~7.2 in one cohort) |
| Hypoxia / birth asphyxia | Associated via ischaemic insult |
| Congenital heart disease | Particularly left-to-right shunts causing gut hypoperfusion |
| Antenatal steroids | Protective against NEC |
| Breast milk | Protective - meta-analysis shows ~4-fold decrease in NEC risk (RR 0.25, 95% CI 0.06-0.98) |
Anatomy of Involvement
- Most commonly: terminal ileum, caecum, and right colon (ascending colon)
- Less commonly: jejunum
- Rarely: duodenum
- In severe cases: NEC totalis - entire GI tract affected
Clinical Features
Presentation spans a spectrum from mild feed intolerance to fulminant multi-organ failure (Bell staging, see below).
Systemic signs:
- Temperature instability
- Lethargy, apnoea, bradycardia
- Hypotension, mottled skin (poor peripheral perfusion)
- Septic shock in advanced disease
GI signs:
- Feed intolerance, bilious aspirates, vomiting
- Abdominal distension
- Rectal bleeding (occult or gross)
- Abdominal wall erythema, oedema, discolouration (blue-grey in perforation due to thin abdominal wall)
- Palpable abdominal mass (matted ischaemic bowel)
Laboratory findings (non-specific, resemble sepsis):
- Thrombocytopenia
- Leukocytosis or leukopenia
- Elevated CRP, lactate
- Metabolic and/or respiratory acidosis
- Coagulopathy in late disease
Bell Staging (Modified Bell Criteria)
| Stage | Classification | Systemic Signs | GI Signs | Radiology | Treatment |
|---|---|---|---|---|---|
| IA | Suspected | Temp instability, apnoea, bradycardia, lethargy | Poor feeding, ↑ gastric residuals, mild distension, occult blood | Distension + mild ileus | NPO, antibiotics |
| IB | Suspected | Same | Bright red rectal blood | Normal or mild ileus | NPO, antibiotics |
| IIA | Definite - mildly ill | Mild systemic illness | Marked distension, absent bowel sounds, gross GI bleeding | Pneumatosis intestinalis | NPO, antibiotics, IV fluids |
| IIB | Definite - moderately ill | Metabolic acidosis, thrombocytopenia | Peritoneal signs, abdominal wall oedema | Pneumatosis, portal venous gas, ascites | Above + consider surgery |
| IIIA | Advanced - severely ill, bowel intact | Deteriorating vital signs, shock, DIC | Peritonitis, abdominal rigidity | Same as IIB | Surgical management |
| IIIB | Advanced - perforated bowel | Same | Perforated bowel | Pneumoperitoneum | Surgery |
(Fischer's Mastery of Surgery, 8th Ed.)
Investigations
Radiology (Plain X-ray - key findings)
- Pneumatosis intestinalis - pathognomonic finding; air within the intestinal wall from bacterial (hydrogen gas) fermentation of luminal substrates
- Portal venous gas - linear echogenicities in the liver on X-ray or USS; indicates severe disease
- Pneumoperitoneum - free intraperitoneal air; absolute indication for surgery; best seen on left lateral decubitus or cross-table lateral view
- Fixed loop - persistent dilation of a specific bowel loop suggests ischaemia/perforation
- Bowel loop separation - due to bowel wall oedema
Ultrasound
- Complex ascites (suggests perforation)
- Bowel wall thickening
- Portal venous gas (multiple linear echogenicities extending to liver periphery)
Macroscopic Pathology
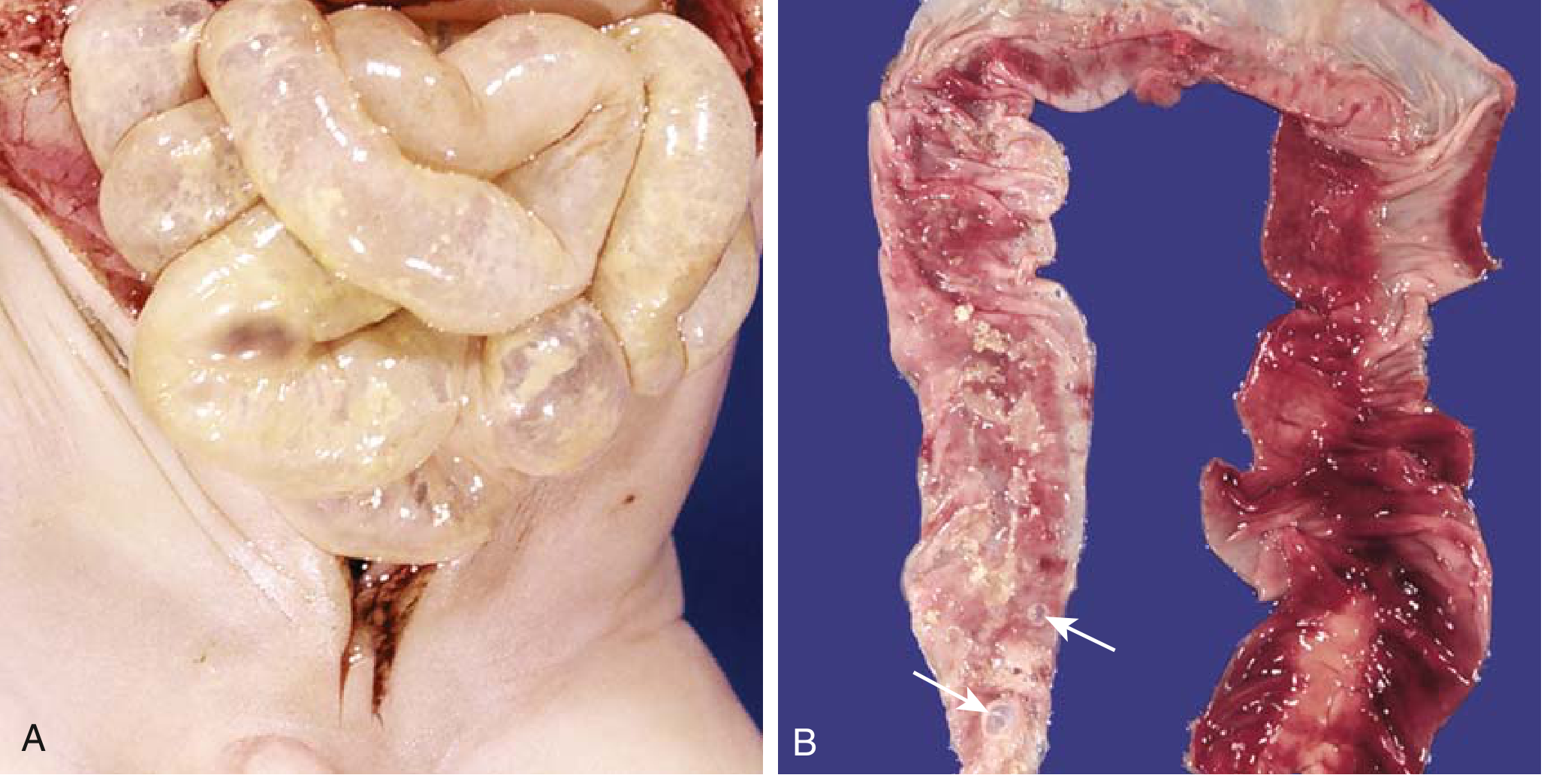
The involved segment is typically distended, friable, and congested - or frankly gangrenous. Intestinal perforation with peritonitis may occur (Robbins Basic Pathology & Robbins Pathologic Basis of Disease).
Microscopy:
- Mucosal or transmural coagulative necrosis
- Ulceration
- Bacterial colonisation
- Submucosal gas bubbles (pneumatosis intestinalis)
- Reparative changes: granulation tissue, fibrosis (post-acute phase)
Management
Medical (>50% of cases managed non-operatively)
- Nil by mouth (NBO) - bowel rest
- Orogastric tube decompression
- IV fluid resuscitation
- Broad-spectrum antibiotics (covering Gram-negative organisms, anaerobes)
- Total parenteral nutrition (TPN)
- Serial abdominal X-rays (every 6-8 hours initially)
- Close monitoring for deterioration
Mild NEC (Bell Stage I-IIA) with feed intolerance, bilious aspirates, and distension often responds to gut rest and antibiotics.
Surgical Indications
Absolute indication:
- Pneumoperitoneum (free air on plain X-ray)
Relative indications:
- Clinical deterioration despite medical management
- Persistent metabolic acidosis
- Abdominal wall cellulitis / erythema
- Palpable abdominal mass
- Fixed bowel loop on serial radiographs
- Portal venous gas
- Worsening obstruction
Surgical Options
-
Peritoneal drain (bedside):
- Especially in extremely low birth weight (<1500 g) premature infants too unstable for theatre
- Removes feculent ascites, decompresses abdomen, improves ventilation
- ~2/3 of infants subsequently require laparotomy
- A multicenter RCT established equivalence in survival, need for PN, and hospital stay vs. laparotomy for infants <1500 g
-
Laparotomy:
- Allows full assessment of disease extent
- General principles: resect all non-viable bowel, preserve maximum intestinal length
- Options for focal disease: repair, resection with anastomosis, or resection with stoma (preferred due to risk of anastomotic leak)
- For patchy/extensive disease: staged resection with second-look laparotomy (24-48 hours later)
- "Clip and drop": in the sickest neonates - resect dead bowel, close open ends with clips, leave abdomen open (laparostomy) with vacuum dressing on low suction; definitive surgery after stabilisation
- For pan-intestinal necrosis (NEC totalis): extremely poor prognosis, often palliation considered
-
Primary anastomosis is occasionally done in rare stable infants with focal isolated perforation and minimal contamination, though anastomotic leak and stricture risks limit enthusiasm.
Complications
| Complication | Detail |
|---|---|
| Intestinal stricture | ~10% of survivors (most commonly splenic flexure of colon); from fibrosis during healing; contrast enema recommended before stoma closure |
| Short bowel syndrome (SBS) | Major cause of SBS in paediatric population; need prolonged admissions or home PN if <40 cm small intestine remaining |
| Sepsis / multi-organ failure | Leading cause of death |
| Neurodevelopmental delay | High incidence in premature survivors |
| Cholestasis / liver disease | From prolonged TPN |
Survivors with >40 cm of small intestine usually adapt over months; those with less may need home PN indefinitely (Bailey & Love's Surgery).
Prevention
| Intervention | Evidence |
|---|---|
| Human breast milk | Strong - ~4-fold reduction in NEC (meta-analysis, RR 0.25) |
| Antenatal corticosteroids | Protective; promotes intestinal maturation |
| Gradual feeding regimens | Clinical pathway-based slow advancement reduces NEC |
| Probiotics | Being evaluated; show promise in reducing NEC (Robbins Pathologic Basis of Disease) |
| Avoiding indomethacin tocolysis | Controversial; may reduce early-onset NEC risk |
Key Points Summary
- NEC = most common GI surgical emergency in neonates; almost exclusive to premature, enterally-fed infants
- Pathognomonic finding: pneumatosis intestinalis (air in bowel wall on X-ray)
- Pneumoperitoneum = absolute surgical indication
- Staging: Bell criteria (I suspected → III advanced/perforated)
- Medical management succeeds in >50%; surgery reserved for deterioration or perforation
- Protective: breast milk, antenatal steroids, gradual feeding advancement
- Key long-term complication: intestinal stricture (commonest at splenic flexure) and short bowel syndrome
- Mortality: 10-30% overall, up to 50% in surgical cases
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Fischer's Mastery of Surgery 8th Ed. | Robbins Basic Pathology & Robbins Pathologic Basis of Disease | Sabiston Textbook of Surgery | Creasy & Resnik's Maternal-Fetal Medicine | Yamada's Textbook of Gastroenterology 7th Ed. | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.