I am orthopaedics post graduate trainee. I am preparing for my university exams. So kindly make a good notes from standard orthopaedics textbooks, recent and classic articles. Please include good images, tables and flow charts for better understanding and easily i can revise and write in exam. Please write answer about the topic in detailed
Asking for Preferences
Please type the specific topic you'd like notes on! For example:
- "Developmental Dysplasia of the Hip"
- "Colles' fracture"
- "Osteomyelitis"
- "Compartment syndrome"
- "Carpal tunnel syndrome"
What topic shall I prepare?
Compartment syndrome
Reading File
Finding Sources
Searching PubMed
"compartment syndrome" AND fasciotomy
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Searching PubMed
"acute compartment syndrome" diagnosis management
COMPARTMENT SYNDROME
Comprehensive Orthopaedic Exam Notes
Sources: Campbell's Operative Orthopaedics 15th Ed (2026), Bailey & Love's Short Practice of Surgery 28th Ed, Miller's Review of Orthopaedics 9th Ed, Current Surgical Therapy 14th Ed, Recent PubMed Reviews (2021-2026)
1. DEFINITION
Compartment syndrome is an elevation of interstitial pressure within a closed osteofascial compartment to a level that compromises tissue perfusion (microvascular compromise), resulting in ischaemia and irreversible muscle and nerve damage.
"Compartment syndrome is raised pressure in a fascial compartment to a level that compromises tissue perfusion." - Bailey & Love, 28th Ed
2. CLASSIFICATION
COMPARTMENT SYNDROME
│
├── ACUTE Compartment Syndrome (ACS)
│ ├── Post-traumatic (most common)
│ ├── Post-ischaemia / Reperfusion
│ └── Non-traumatic
│
└── CHRONIC / EXERTIONAL (CECS)
└── Recurrent exertion-related pressure increase
3. ANATOMY - COMPARTMENTS
3a. LEG (4 compartments) - MOST COMMON SITE
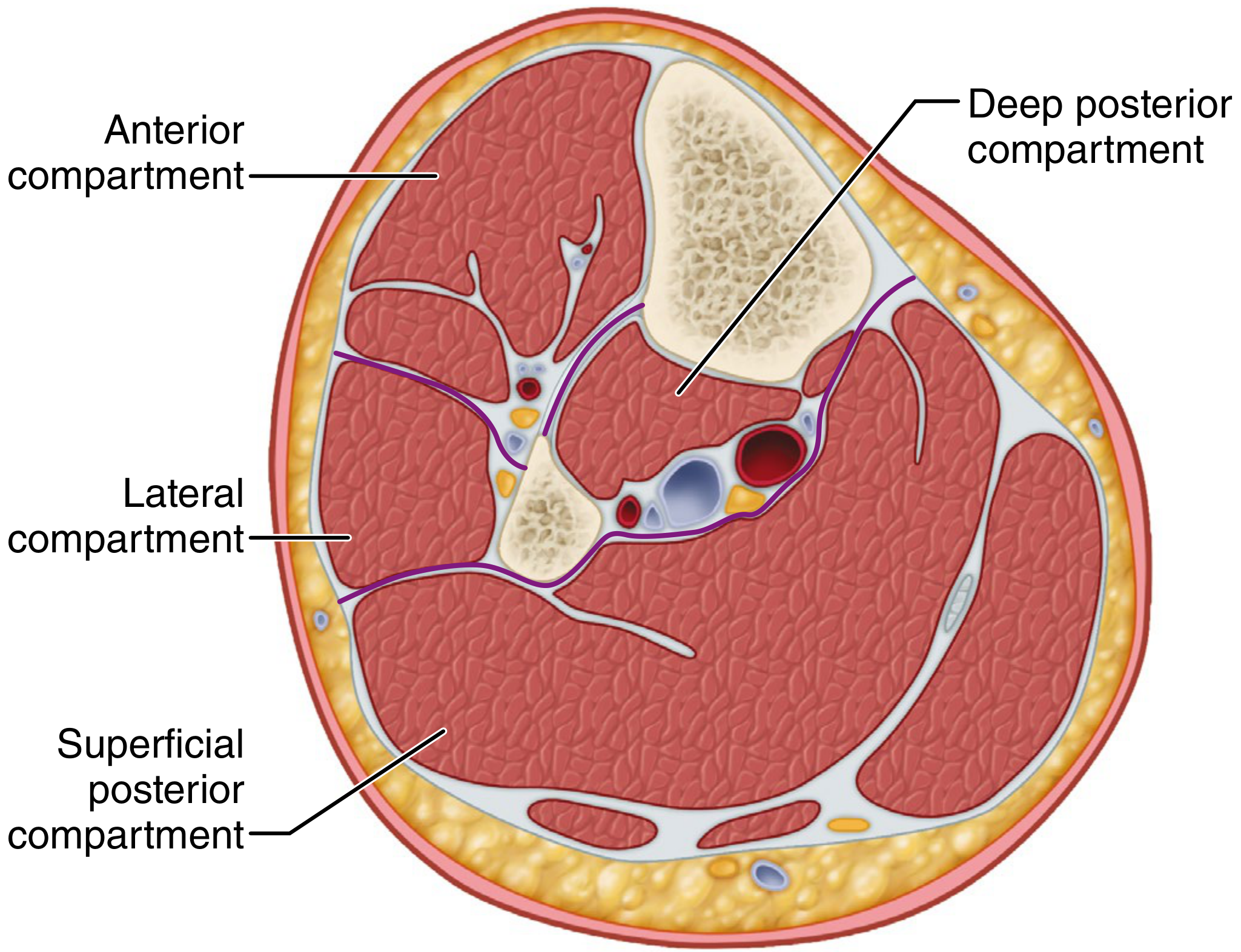
| Compartment | Contents | Nerve at Risk | Clinical Signs if Affected |
|---|---|---|---|
| Anterior | Tibialis anterior, EHL, EDL, peroneus tertius | Deep peroneal nerve | Foot drop, numbness 1st web space |
| Lateral | Peroneus longus & brevis | Superficial peroneal nerve | Weak eversion, numbness dorsum foot |
| Superficial Posterior | Gastrocnemius, soleus, plantaris | Sural nerve | Weak plantarflexion |
| Deep Posterior | FHL, FDL, tibialis posterior | Posterior tibial nerve | Numbness sole, weak toe flexion |
The anterior and deep posterior compartments are the most commonly involved.
3b. FOREARM (3 compartments)
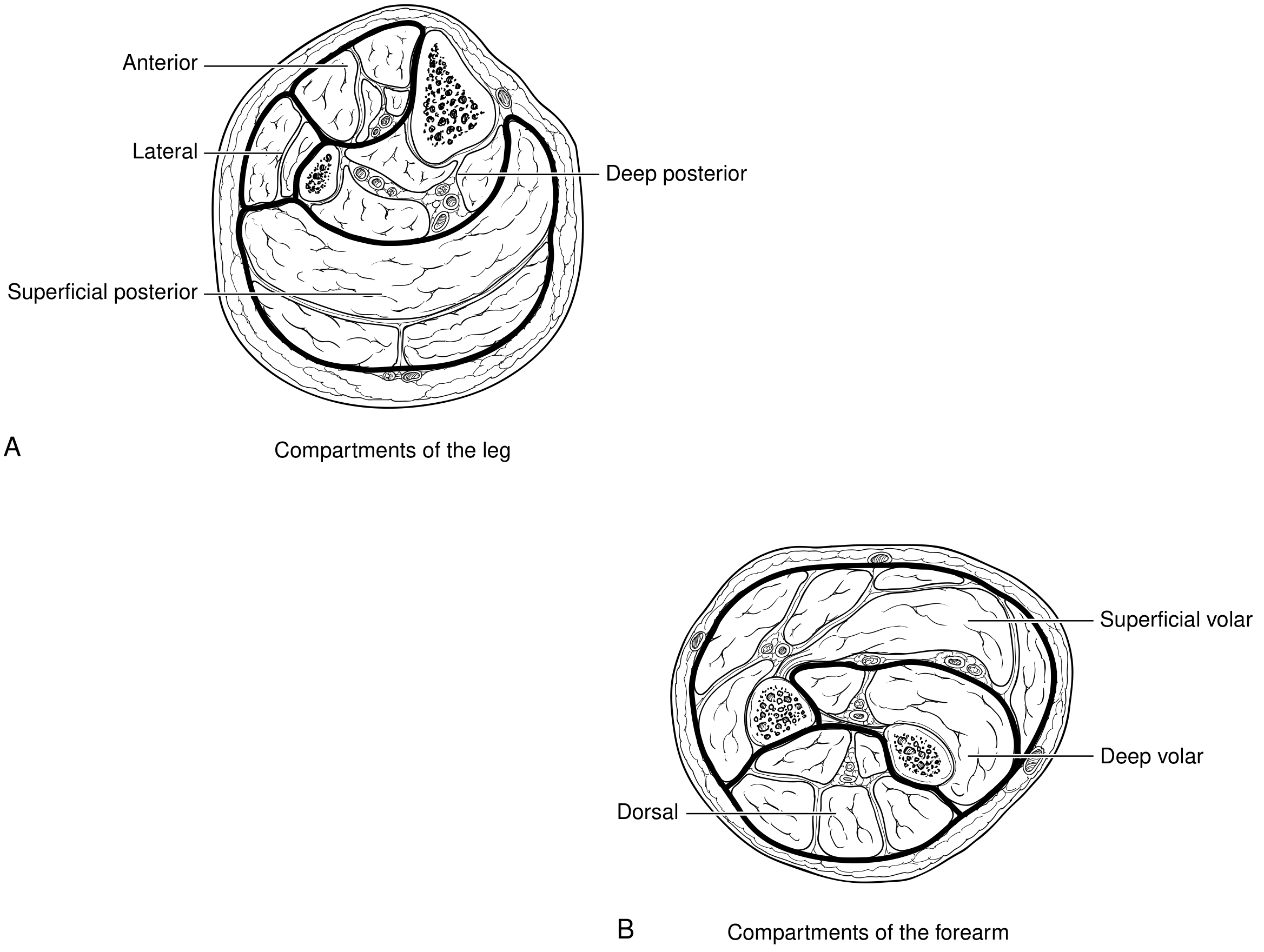
| Compartment | Contents |
|---|---|
| Superficial volar | Wrist and finger flexors (FCR, FCU, FDS) |
| Deep volar | FDP, FPL, pronator quadratus |
| Dorsal | Wrist and finger extensors |
3c. THIGH (3 compartments)
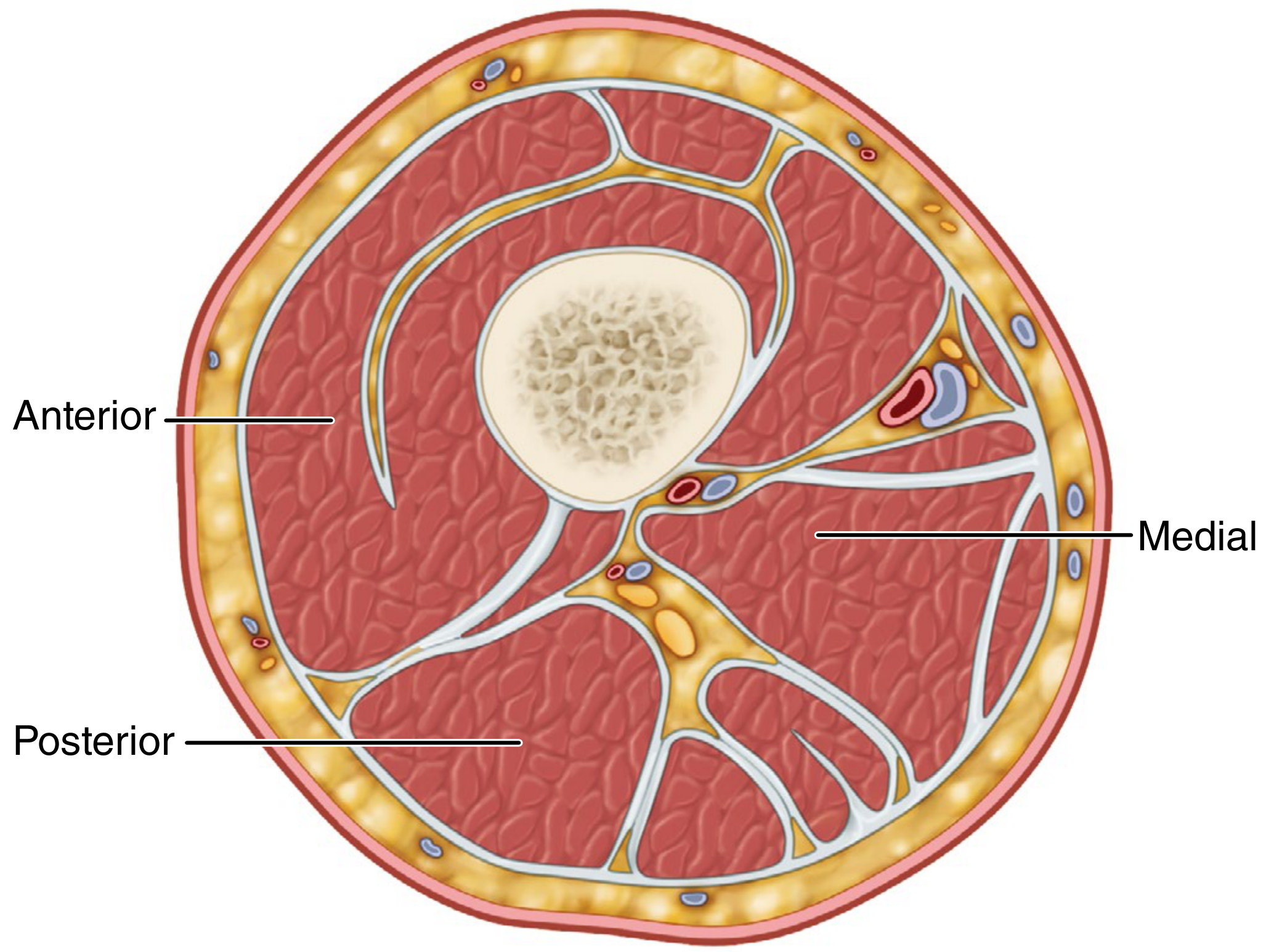
| Compartment | Contents |
|---|---|
| Anterior | Quadriceps, sartorius; femoral nerve + artery + vein |
| Medial | Adductors; profunda femoris, obturator artery, obturator nerve |
| Posterior | Hamstrings; sciatic nerve, branches of profunda femoris |
3d. OTHER SITES
- Foot (9 compartments - most commonly from calcaneus fractures, incidence ~17%)
- Hand
- Buttock/Gluteal
- Arm
- Shoulder
- Lumbar paraspinous muscles
4. AETIOLOGY / CAUSES
Causes by Mechanism
CAUSES OF COMPARTMENT SYNDROME
│
├── DECREASED COMPARTMENT SIZE (external compression)
│ ├── Tight plaster casts or dressings
│ ├── Circumferential burns (especially 3rd degree)
│ ├── Tight closure of fascial defects
│ └── Pneumatic antishock garments
│
└── INCREASED COMPARTMENT CONTENT (volume increase)
├── Fractures ← Most common cause (70%)
├── Soft-tissue trauma / contusions (23%)
├── Arterial injury / ischaemia-reperfusion
├── IV fluid extravasation (IV contrast under pressure)
├── Spontaneous haematoma (anticoagulants/bleeding disorders)
├── Limb compression during altered consciousness
└── Burns (oedema)
Key fact for exams: Fractures are the most common cause (70%), with tibial shaft fractures being the single highest-risk fracture type. Compartment syndrome CAN occur with open fractures - do not be falsely reassured.
5. PATHOPHYSIOLOGY
INITIAL INSULT
(trauma / compression / ischaemia)
↓
Increased tissue pressure in closed compartment
↓
↓ Capillary perfusion pressure
(perfusion = MAP - compartment pressure)
↓
Local tissue hypoxia → Cellular anoxia
↓
Histamine release → ↑ Capillary permeability
↓
Protein-rich fluid leaks into interstitium → MORE OEDEMA
↓
VICIOUS CYCLE: More pressure → More ischaemia
↓
Irreversible muscle necrosis (begins at 4-6 hours)
Nerve ischaemia (type C fibres most sensitive first)
↓
Rhabdomyolysis → Myoglobinuria → Acute Tubular Necrosis
↓
Late: Volkmann's ischaemic contracture (untreated)
Critical thresholds (Campbell's, 2026):
- Significant muscle necrosis occurs when intracompartmental pressure (ICP) >30 mmHg sustained for >8 hours
- Higher pressures cause irreversible damage in shorter timeframes
- Exercise alone can increase muscle volume by 20%, raising CECS risk
6. CLINICAL FEATURES - THE "6 Ps"
Mnemonic: 6Ps (in order of appearance)
| Sign | Description | Timing |
|---|---|---|
| Pain (out of proportion) | Disproportionate to the injury; not relieved by adequate analgesia | EARLY |
| Pain on Passive Stretch | Key early sign - passive stretch of muscles within the compartment causes pain | EARLY |
| Paraesthesia | Numbness/tingling in distribution of nerves in the compartment (Type C non-myelinated fibres most sensitive) | EARLY-MID |
| Pressure | Tense, woody compartment on palpation | EARLY-MID |
| Paralysis | Motor weakness | LATE |
| Pallor | Skin pallor | LATE |
| Pulselessness | Absent distal pulses | EXTREMELY LATE |
Critical exam point: Pain out of proportion + Pain on passive stretch = hallmark early signs. Paralysis, pallor, and pulselessness are LATE signs - if you wait for these, irreversible damage has occurred.
Pulses are PRESENT in compartment syndrome - their absence is a sign of arterial occlusion, which is a different diagnosis. Do not use presence of pulses to exclude compartment syndrome.
Specific Compartment Signs
| Compartment | Muscle tested (passive stretch) | Sensory loss |
|---|---|---|
| Anterior (leg) | Passive plantarflexion stretches tibialis anterior → pain | 1st web space (deep peroneal) |
| Deep posterior (leg) | Passive toe extension stretches FHL, FDL → pain | Sole of foot (posterior tibial) |
| Volar forearm | Passive finger/wrist extension | Median nerve distribution |
7. DIAGNOSIS
7a. Clinical Diagnosis
Compartment syndrome is primarily a clinical diagnosis:
- Pain out of proportion
- Increasing pain despite adequate analgesia
- Pain on passive stretch of muscles in the compartment
- Tense, woody compartment
7b. Compartment Pressure Measurement
Indications for pressure measurement:
- Diagnostic uncertainty
- Altered level of consciousness (head injury, sedation, intubation)
- Polytrauma victims
- Uncooperative or unreliable patients
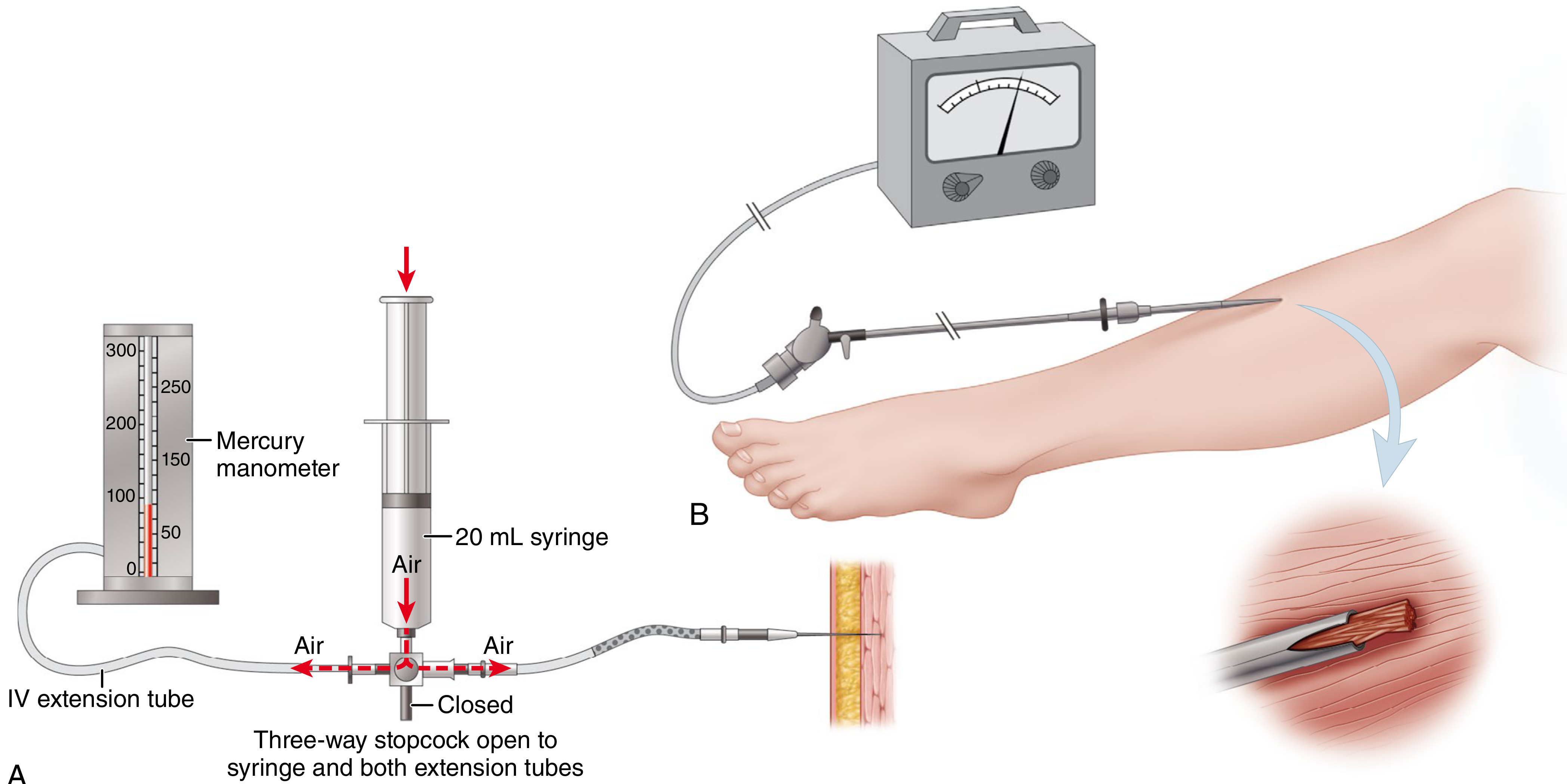
Techniques:
| Method | Description |
|---|---|
| Whitesides technique | Needle + mercury manometer + IV extension tubing - simple bedside technique |
| Wick catheter | Continuous monitoring |
| Slit catheter (Mubarak) | Most accurate for continuous monitoring |
| Stryker STIC device | Commercial handheld pressure monitor - most widely used |
7c. Pressure Thresholds for Fasciotomy
| Criterion | Threshold | Notes |
|---|---|---|
| Absolute ICP | ≥ 30 mmHg | Simple but less accurate in hypotensive patients |
| Delta pressure (ΔP) = DBP - ICP | ≤ 30 mmHg | AAOS recommended criterion - accounts for systemic BP |
| Delta pressure (ΔP) strict | ≤ 10-20 mmHg | Some use 20 mmHg; most conservative threshold |
AAOS Clinical Practice Guidelines: Fasciotomy when ΔP (diastolic BP - compartment pressure) is ≤ 30 mmHg.
Measure multiple sites near (but not in) the fracture, in all compartments of the affected limb.
CPK elevation and myoglobinuria are late markers of tissue destruction - should NOT be used to establish diagnosis.
8. ALGORITHM FOR MANAGEMENT
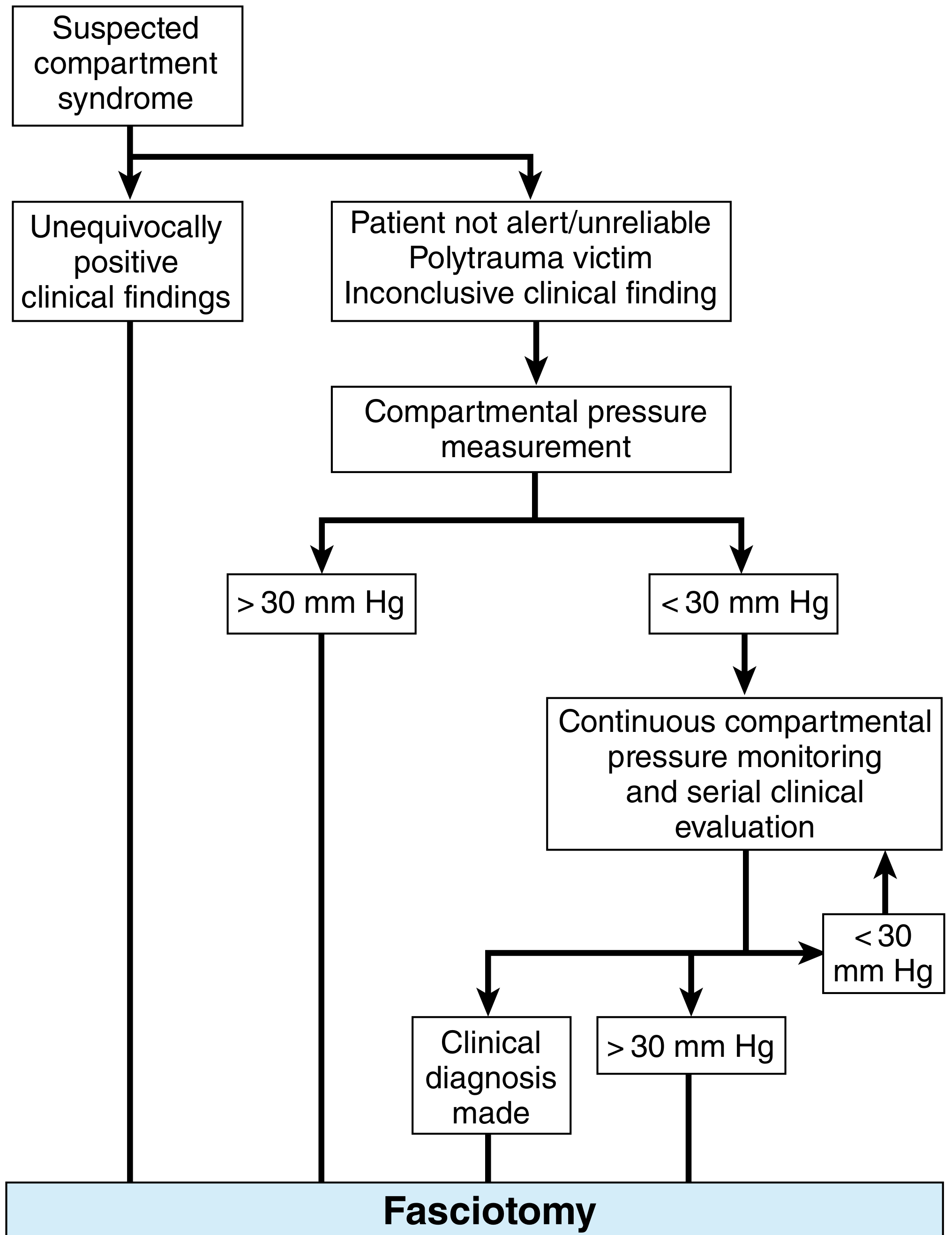
SUSPECTED COMPARTMENT SYNDROME
│
┌─────┴──────────────────────────┐
↓ ↓
Unequivocally Patient not alert /
positive clinical Polytrauma /
findings Inconclusive findings
│ │
│ Compartment pressure measurement
│ │ │
│ > 30 mmHg < 30 mmHg
│ │ │
│ │ Continuous monitoring
│ │ + serial examination
│ │ ↓ (if ΔP ≤ 30 → ↓)
└─────────────────────────┘
│
FASCIOTOMY
│
┌────────┴────────┐
Within 6-8 h > 12 h
Best outcomes ↑ Complications
9. TREATMENT
9a. Initial / Emergency Measures
- Remove all constrictive dressings and split casts to the skin - reduces ICP by 50-85%
- Position limb at level of heart (NOT elevated) - elevation reduces arterial inflow without improving venous drainage, worsening ischaemia
- Maintain systemic BP (optimise perfusion)
- High-flow O2
- Do NOT delay - if clinical diagnosis is clear → immediate fasciotomy
Do NOT elevate the limb above heart level in compartment syndrome - this is a common mistake.
9b. Fasciotomy - Definitive Treatment
Timing: Within 6-8 hours for best outcomes. After 12 hours → significantly higher complication rates. Fasciotomy after 12 hours is not contraindicated but outcomes are worse.
LOWER LEG FASCIOTOMY
Two approaches:
Option 1: DOUBLE-INCISION (Mubarak & Hargens) - PREFERRED
- Releases all 4 compartments
- Anterolateral incision: 20-25 cm, between fibular shaft and tibial crest
- Anterior compartment released first
- Then lateral compartment through same incision
- Posteromedial incision: 20-25 cm, 1-2 cm posterior to medial border of tibia
- Superficial posterior compartment released
- Detach soleus from tibia to release deep posterior compartment
Option 2: SINGLE-INCISION (Davey et al.)
- Lateral incision in line with fibula, from fibular head to 3-4 cm proximal to lateral malleolus
- Releases all 4 compartments but technically more demanding
- Risk of injury to superficial peroneal nerve
| Technique | Incisions | Advantage |
|---|---|---|
| Double-incision (Mubarak) | Anterolateral + Posteromedial | Safer, most reliable 4-compartment release |
| Single-incision (Davey) | Lateral (fibular) | Fewer incisions, technically demanding |
FOREARM FASCIOTOMY
- Volar: Curved incision from antecubital fossa to palm (Henry's approach) - releases superficial + deep volar
- Dorsal: Straight dorsal incision - releases dorsal compartment
- Carpal tunnel release if hand involved
- Consider mobile wad (BR, ECRL, ECRB) release
THIGH FASCIOTOMY (Tarlow et al.)
- Lateral incision from intertrochanteric line to lateral epicondyle
- Incise iliotibial band
- Release lateral intermuscular septum → releases anterior and posterior compartments
- Medial incision only if medial compartment pressure elevated
9c. Post-Fasciotomy Wound Management
Fasciotomy wound LEFT OPEN
↓
Vacuum-Assisted Closure (VAC) device applied
(reduces oedema, promotes granulation)
↓
Re-inspect at 48-72 hours
↓
Delayed Primary Closure (when swelling subsides) OR
Split-Thickness Skin Graft (if cannot close primarily)
Never attempt early primary closure - this may cause recurrence of compartment syndrome.
10. CHRONIC EXERTIONAL COMPARTMENT SYNDROME (CECS)
Features
| Feature | Details |
|---|---|
| Who? | Young athletes, military recruits, long-distance runners, weightlifters/rowers (forearm) |
| Pattern | Reproducible pain/tightness during exercise, resolves at rest within 15-30 min |
| Mechanism | Exercise increases muscle volume by 20% → pressure in non-compliant compartment |
| Sites | Anterior > Deep posterior leg; less commonly forearm |
| Association | 15-40% have fascial hernias |
Diagnostic Criteria (Pedowitz Criteria)
| Criterion | Threshold |
|---|---|
| Resting pre-exercise pressure | ≥ 15 mmHg |
| Pressure 1 minute post-exercise | ≥ 30 mmHg |
| Pressure 5 minutes post-exercise | ≥ 20 mmHg |
Diagnosis made if one or more criteria are met.
Differential Diagnosis of CECS
- Stress fracture
- Nerve entrapment syndrome
- Popliteal artery entrapment syndrome
- Vascular claudication
- Lumbosacral radiculopathy
- Neurogenic claudication
- Myopathy / infection / tumour
Treatment of CECS
CECS TREATMENT
│
├── NONOPERATIVE (1st line)
│ ├── Activity modification / relative rest
│ ├── NSAIDs
│ ├── Physiotherapy (stretching, strengthening)
│ ├── Orthotics
│ ├── Forefoot running technique (↓ ICP, 65-75% success)
│ └── Manual therapy
│
└── OPERATIVE (if non-op fails)
├── Fasciotomy of affected compartment(s)
├── Anterior fasciotomy: 80-90% success rate
└── Deep posterior fasciotomy: 50-70% success rate
11. COMPLICATIONS
If Compartment Syndrome is Missed / Delayed Treatment
| Complication | Description |
|---|---|
| Volkmann's Ischaemic Contracture | Classic late sequel - fibrosis of forearm flexors → fixed flexion deformity hand/wrist |
| Rhabdomyolysis | Muscle breakdown → myoglobinuria |
| Acute Renal Failure (ATN) | Myoglobin-induced acute tubular necrosis |
| Infection / Sepsis | Necrotic muscle → sepsis |
| Neurological deficit | Permanent nerve damage |
| Amputation | Severe cases |
Complications of Fasciotomy Itself
- Wound infection
- Haematoma
- Nerve injury (superficial peroneal nerve at risk in single-incision technique) | Hypertrophic / ugly scarring
- Skin graft morbidity
- Inadequate decompression (missed compartments)
12. SPECIAL SITUATIONS
Reperfusion Compartment Syndrome
- After revascularisation of acutely ischaemic limb (prolonged ischaemia >6 hours)
- Prophylactic fasciotomy recommended at time of revascularisation
- More severe the ischaemia, more likely reperfusion CS to develop
- Monitor CPK; if rhabdomyolysis: aggressive IV fluids targeting urine output >100 mL/hr until CPK <5000 U/L; urine alkalisation with bicarbonate
Compartment Syndrome with Open Fractures
- Do not assume fasciotomy is unnecessary with open fractures
- Skin opening does NOT decompress fascial compartments
- High index of suspicion required
Compartment Syndrome in Tibial Plateau Fractures
- High-energy patterns (Schatzker V/VI) carry high risk
- Monitor closely post-op
- Recent review 2022 (PMID: 34799021) highlights tibial plateau fractures as a high-risk group
Compartment Syndrome After Arthroplasty
- Uncommon but well-described after knee and hip arthroplasty
- Review 2022 (PMID: 34799019) in Orthop Clin North Am
13. VOLKMANN'S ISCHAEMIC CONTRACTURE
This is the classic end-stage complication of untreated forearm/hand compartment syndrome - very high-yield for exams.
Pathology
Ischaemia of forearm musculature (especially deep flexors) → necrosis → fibrous replacement → contracture
Clinical Grading (Seddon's Classification)
| Grade | Features | Treatment |
|---|---|---|
| Mild | Slight finger flexion contracture; correctable | Physiotherapy, splinting |
| Moderate | Wrist and finger flexion contracture; uncorrectable passively | Muscle slide (flexor-pronator slide) |
| Severe | Wrist, finger, and thumb flexion contracture + neurological deficit | Excision of infarcted muscle, neurolysis, tendon lengthening |
14. QUICK REVISION TABLE - HIGH-YIELD FACTS
| Fact | Value/Answer |
|---|---|
| Most common site | Leg (anterior + deep posterior compartment) |
| Most common cause | Fractures (70%) |
| Earliest signs | Pain out of proportion + Pain on passive stretch |
| Latest sign | Pulselessness |
| Nerve most sensitive | Type C non-myelinated sensory fibres |
| ICP threshold (absolute) | ≥ 30 mmHg |
| ΔP threshold (AAOS) | DBP - ICP ≤ 30 mmHg |
| Best fasciotomy timing | Within 6-8 hours |
| Do NOT elevate limb | ↓ Arterial inflow without ↑ venous drainage |
| Cast splitting reduces ICP by | 50-85% |
| CECS Pedowitz: post-exercise 1 min | ≥ 30 mmHg |
| CECS Pedowitz: post-exercise 5 min | ≥ 20 mmHg |
| CECS Pedowitz: resting | ≥ 15 mmHg |
| Anterior fasciotomy success (CECS) | 80-90% |
| Deep posterior fasciotomy success | 50-70% |
| Fascial hernia association (CECS) | 15-40% |
| Calcaneus fracture CS incidence | ~17% |
| Classic late complication | Volkmann's ischaemic contracture |
15. RECENT EVIDENCE (2021-2026)
| Study | PMID | Relevance |
|---|---|---|
| Bouklouch et al. (2025), Injury - "Diagnosis of acute compartment syndrome: current diagnostic parameters" | 41173558 | Reviews ΔP vs absolute thresholds; supports ΔP ≤ 30 mmHg as primary criterion |
| Farah et al. (2023), Clin Sports Med - "Acute Compartment Syndrome in the Athlete" | 37208063 | Specific considerations in athletic population |
| Schneiderman & O'Toole (2022), Orthop Clin NA - "CS in High-Energy Tibial Plateau Fractures" | 34799021 | High-risk fracture pattern - need early monitoring |
| Shaikh et al. (2026), J Hand Surg Am - "Acute CS of the Upper Extremity" | 40853300 | Comprehensive review of forearm/hand CS |
| Tapia-Nanez et al. (2025), Int Orthop - "Foot compartment syndrome treatment: systematic review" | 40461896 | Systematic review on foot CS fasciotomy outcomes |
16. EXAM WRITING TIPS
For a long-answer question:
- Define → Classify → Anatomy
- Aetiology → Pathophysiology
- Clinical features (early vs late) + special clinical tests
- Diagnosis (clinical + pressure measurement + thresholds)
- Management (emergency measures → fasciotomy technique → wound care)
- Complications (of the syndrome and of fasciotomy)
- Special scenarios (CECS, reperfusion, open fractures)
- Volkmann's contracture
Examiner favourites:
- "Why do we NOT elevate the limb?" - Elevation decreases arterial inflow without significantly increasing venous outflow
- "Which nerve is most sensitive to compartment ischaemia?" - Type C non-myelinated fibres (sensory)
- "Can compartment syndrome occur with open fractures?" - YES
- "What is the ΔP formula?" - Diastolic BP minus Compartment Pressure ≤ 30 mmHg = fasciotomy
- "What are Pedowitz criteria?" - For CECS diagnosis
Sources: Campbell's Operative Orthopaedics 15th Edition 2026 (Ch 53) | Bailey & Love's Short Practice of Surgery 28th Ed (Ch 32, 61) | Miller's Review of Orthopaedics 9th Ed | Current Surgical Therapy 14th Ed | PubMed 2021-2026
Please turek, rock wood and tuli textbooks. Please make notes on scfe
Finding Sources
Finding Sources
Searching PubMed
"slipped capital femoral epiphysis" treatment outcomes
Finding Sources
Finding Sources
Searching PubMed
"slipped capital femoral epiphysis" AND "in situ pinning"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Note on requested textbooks: Turek's Orthopaedics and Tuli's Textbook of Orthopaedics are not currently in the digital library. The notes below are compiled from Campbell's Operative Orthopaedics 15th Ed 2026, Bailey & Love's Short Practice of Surgery 28th Ed, Grainger & Allison's Diagnostic Radiology, Schwartz's Principles of Surgery, and Rockwood & Green's Fractures in Adults 10th Ed 2025, supplemented with classic and recent PubMed literature.
SLIPPED CAPITAL FEMORAL EPIPHYSIS (SCFE / SUFE)
Comprehensive Orthopaedic Exam Notes
1. DEFINITION
SCFE is a Salter-Harris Type I physeal injury of the proximal femoral growth plate in which the capital (proximal femoral) epiphysis displaces posteromedially and inferiorly relative to the femoral neck/metaphysis.
Correct anatomical terminology: It is technically the metaphysis (femoral neck) that displaces anterolaterally and superiorly relative to the fixed epiphysis - since the epiphysis is held in the acetabulum. The term "slipped epiphysis" is therefore a misnomer, but universally used.
- Commonest hip disorder of adolescence
- Incidence: ~5 per 100,000 population
- Peak age: 10-16 years, puberty
- Boys more than girls (2:1), though peak occurs earlier in girls (due to earlier puberty)
2. AETIOLOGY AND RISK FACTORS
Mechanical / Physiological Factors
GROWTH SPURT
↓
Physeal changes during puberty:
• ↑ Obliquity of physis (more vertical → ↑ shear forces)
• Thinning of perichondrial ring
• Widening of physis
• ↓ Neck-shaft angle
• ↓ Size of epiphyseal tubercle
• ↑ Growth hormone → weakens hypertrophic zone of physis
↓
Weakened physis subjected to torsional/shear forces
↓
SCFE
Risk Factors (Campbell's Box 38.8)
| Category | Risk Factor |
|---|---|
| Demographic | Age 10-16, puberty; Male sex; African/Afro-Caribbean ancestry (2x more common); Open triradiate cartilage |
| Metabolic | Obesity (single most important predisposing factor) |
| Endocrine | Hypothyroidism, growth hormone deficiency/excess, hypogonadism, hypopituitarism, panhypopituitarism, chronic renal failure |
| Other | Previous local radiotherapy; Down syndrome; Genetics |
Endocrine rule for exams: If SCFE occurs in an atypical patient (age <10 or >16, underweight, bilateral), always investigate for an endocrine cause (especially hypothyroidism).
3. PATHOLOGY
- The slip occurs through the hypertrophic zone of the physis (zone of provisional calcification) - same as Salter-Harris Type I fracture
- The epiphysis displaces posteromedially and inferiorly
- Metaphysis (neck) moves anterolaterally and superiorly
- Results in:
- Increased anteversion lost → retroversion
- "Cam" type femoroacetabular impingement (FAI) in chronic slips
- Disruption of blood supply in severe/unstable slips → AVN
4. CLINICAL FEATURES
Symptoms
| Symptom | Notes |
|---|---|
| Pain | Groin, medial thigh, or knee (referred via obturator nerve - Hilton's law). Many children present to orthopaedics with knee pain → do not miss the hip |
| Limp | Antalgic or Trendelenburg gait |
| Duration | Weeks to months in chronic slips; sudden onset in acute slips |
Signs
| Sign | Description |
|---|---|
| External rotation deformity | Leg lies in ER at rest |
| Drehmann sign (PATHOGNOMONIC) | When the hip is FLEXED, the leg AUTOMATICALLY EXTERNALLY ROTATES - due to the posteriorly displaced epiphysis hitting the posterior acetabular wall |
| Restricted internal rotation | Most sensitive early sign |
| Restricted flexion | Reduced hip flexion |
| Limb shortening | Mild |
| Wasting of thigh | In chronic cases |
Key exam point: Drehmann's sign - obligatory external rotation of hip on flexion - is pathognomonic of SCFE.
5. INVESTIGATIONS
X-Rays (Mandatory)
Two views required: AP Pelvis + Frog-leg Lateral
Critical point: Frog-leg lateral is more sensitive than AP. Do NOT accept only an AP view in a child with hip/knee pain.
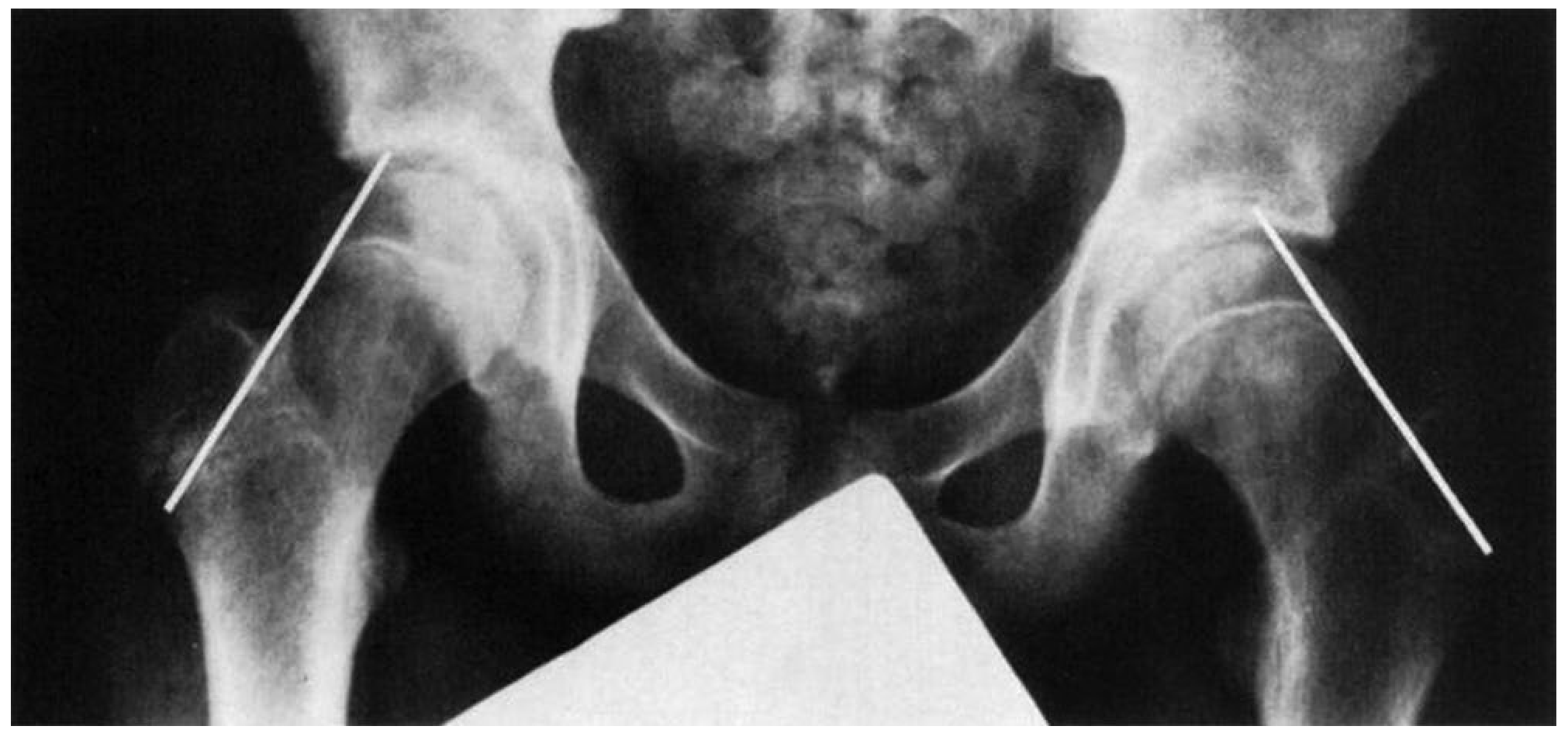
Key Radiological Signs on AP Pelvis
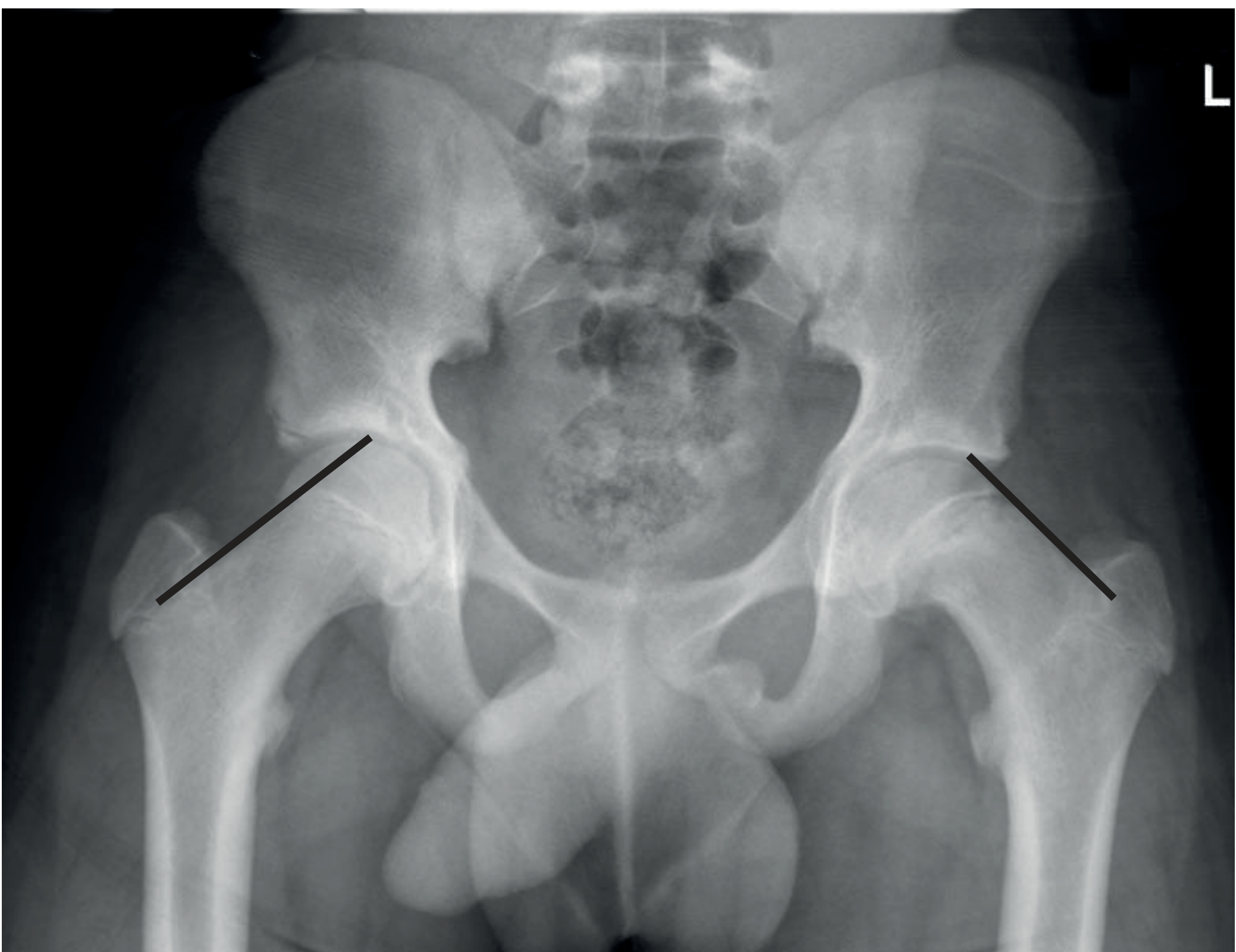
1. Klein's Line (Trethowan's sign)
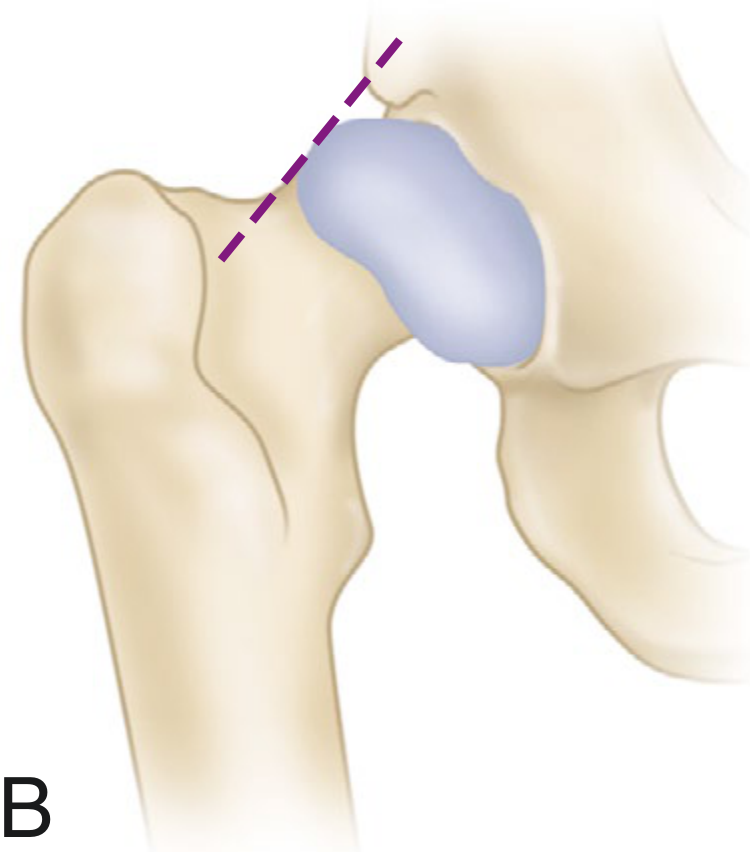
- A line drawn along the superior border of the femoral neck (Klein's line) normally intersects the lateral part of the femoral epiphysis
- In SCFE, the epiphysis is displaced medially/inferiorly → Klein's line fails to intersect the epiphysis (or intersects less than normal)
2. Steel's "Metaphyseal Blanch Sign"
- Double density (sclerosis) at the metaphysis on AP view
- Due to overlap of the posteriorly displaced epiphysis with the neck
3. Widening and irregularity of the physis
4. Decreased epiphyseal height on AP view
5. Decreased head-neck offset (loss of normal convexity)
Southwick Slip Angle (Lateral view)
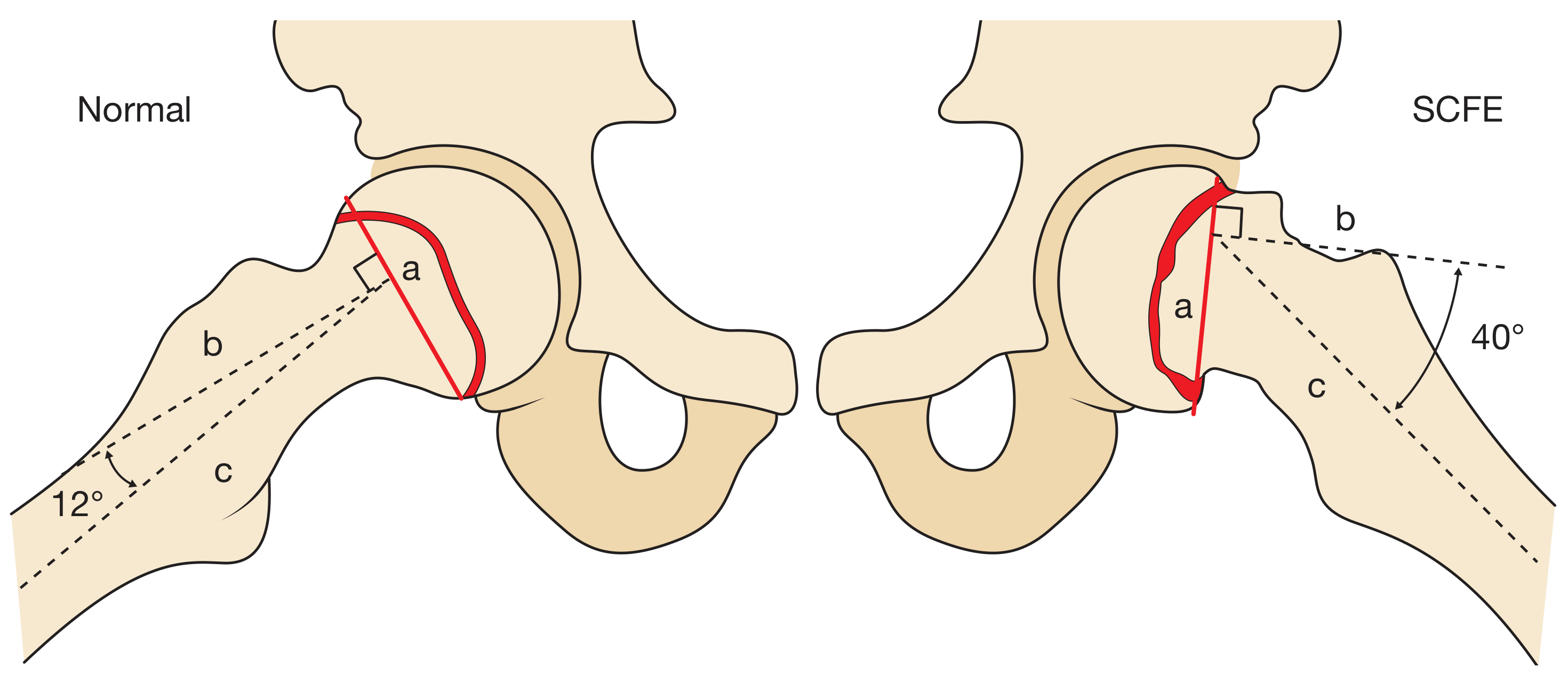
- Measured on frog-leg lateral view
- Normal neck-shaft angle ~12°
- Mild: <30°, Moderate: 30-60°, Severe: >60°
AP Pelvis showing Klein's line bilaterally
MRI
- Useful for preslip (physeal oedema before visible displacement)
- Also for diagnosis in inconclusive X-rays
- Can diagnose contralateral preslip
CT
- Useful to assess degree of slip and plan osteotomy
6. CLASSIFICATION
6a. By Duration of Symptoms (Traditional)
| Type | Duration | Features |
|---|---|---|
| Acute | Symptoms <3 weeks | Sudden onset; may be following trivial trauma |
| Chronic | Symptoms >3 weeks | Most common (60-90%); gradual onset |
| Acute-on-Chronic | Chronic symptoms + sudden worsening |
Traditional classification is descriptive but has limited prognostic value (Campbell's).
6b. By Stability - Loder Classification (Most Important)
| Type | Definition | AVN Risk |
|---|---|---|
| Stable | Patient CAN walk, with or without crutches | ~0% |
| Unstable | Patient CANNOT walk, even with crutches | ~47% |
Most widely used and prognostically important classification. An unstable SCFE is a surgical emergency.
Satisfactory results: 96% stable vs 47% unstable (Loder et al.).
6c. By Severity of Slip
| Grade | % Metaphysis Uncovered | Southwick Angle |
|---|---|---|
| Mild (Grade I) | <33% | <30° |
| Moderate (Grade II) | 33-66% | 30-60° |
| Severe (Grade III) | >66% | >60° |
6d. Preslip
- Symptomatic physeal weakening without visible displacement
- Widening/irregularity of physis on X-ray
- Physeal oedema on MRI
7. MANAGEMENT
Algorithm
SCFE CONFIRMED
│
┌────┴────┐
STABLE UNSTABLE (emergency - cannot walk)
│ │
↓ ↓
In Situ Urgent surgery within 24 h
Fixation Gentle repositioning under GA
(1 cannulated + Capsulotomy to reduce tamponade
screw) + Fixation with 1-2 cannulated screws
│
↓
MILD SLIP (Stable) MODERATE/SEVERE SLIP (Stable)
│ │
In situ fixation In situ fixation OR
(90%+ success) Modified Dunn procedure
(controversial - risk of AVN)
│
If deformity causes FAI after healing:
Osteochondroplasty / Osteotomy
7a. In Situ Pinning (Standard Treatment)
Technique (Canale et al. - Campbell's Technique 38.21):
- Patient supine on fracture table
- Fluoroscopic guidance (C-arm)
- Percutaneous single cannulated screw (4.5 or 7.3 mm)
- Entry point on anterior thigh, adjusted for degree of slip
- Screw placed perpendicular to physis, in center-center position of femoral head
- Screw tip should be ≥4 mm from subchondral bone (prevents penetration)
- Capsulotomy for acute/unstable slips (reduces intracapsular tamponade on blood supply)
- Confirm non-penetration with multiple fluoroscopic views
Key points:
- Single screw fixation is standard (Aronson & Carlson)
- 2 screws for acute unstable slips
- Screw perpendicular to physis (not to femoral neck axis) - this is important
- Do NOT attempt forceful reduction in stable/chronic slips
| Complication | Description |
|---|---|
| Screw penetration | Leads to chondrolysis, synovitis, degenerative OA |
| AVN | ~0% in stable, ~47% in unstable |
| Chondrolysis | Narrowing of joint space; worse prognosis |
| Femoral neck fracture | Rare complication of pinning |
7b. Modified Dunn Procedure (Leunig, Slongo & Ganz - Technique 38.22)
Indications: Moderate to severe slips (especially unstable); to reduce risk of FAI and achieve anatomical reduction
Procedure:
- Lateral decubitus position; Gibson approach
- Trochanteric flip osteotomy
- Surgical dislocation of the femoral head (safe dislocation preserving blood supply via MFCA - deep branch)
- Neck osteotomy and realignment of epiphysis
- Fixation with K-wires/screws
- Trochanteric reattachment
Advantage: Anatomical correction, reduces FAI, preserves blood supply
Disadvantage: Technically demanding; high AVN risk if done incorrectly; only by experienced hip surgeons
7c. Other Surgical Options
| Procedure | Indication | Notes |
|---|---|---|
| Base-of-neck osteotomy (Dunn) | Moderate/severe slips | Higher AVN risk than modified Dunn |
| Intertrochanteric osteotomy (Southwick) | Severe deformity after physeal closure | Lower AVN risk but at a distance from CORA |
| Subtrochanteric osteotomy (Imhauser) | Severe chronic deformity | Most distant from deformity |
| Osteochondroplasty (FAI surgery) | After healing with residual FAI | Arthroscopic or open |
The closer the osteotomy is to the deformity (CORA = at the physis), the better the correction but higher the AVN risk. Intertrochanteric osteotomy trades some correction for lower risk.
8. BILATERAL SCFE
| Fact | Data |
|---|---|
| Overall incidence | 25-40% of all SCFE patients |
| Caucasian patients | ~25% bilateral |
| Afro-American/Caribbean | Up to 50% bilateral |
| Left vs right | Left side more commonly affected (65%) |
| Timing of 2nd slip | Usually within 12-18 months of first |
Prophylactic Pinning of Contralateral Hip
Indications (Campbell's Box - Prophylactic pinning indicated when):
- Age: females <10 years; males <12 years
- Endocrine abnormalities
- Unreliable follow-up
- Posterior sloping angle >12 degrees (Fig 38.119)
- Open triradiate cartilage
- Low vitamin D
- Hypothyroidism / Severe obesity / Diabetes mellitus
- History of human growth hormone use
Kocher decision analysis: observation is optimal in most, but prophylactic fixation in high-risk patients or poor follow-up.
9. COMPLICATIONS
Complications of SCFE Itself
| Complication | Notes |
|---|---|
| Avascular Necrosis (AVN) | Most devastating. Rare in stable (0%), common in unstable (~47%). Due to injury to lateral epiphyseal vessels. |
| Chondrolysis | Acute dissolution of articular cartilage → joint space narrowing. May be idiopathic or pin penetration-related. More common in Black patients, females, severe slips. |
| Femoroacetabular Impingement (FAI) | "Cam" type - most common late complication. Residual deformity causes impingement → early OA |
| Osteoarthritis | Long-term consequence of FAI, chondrolysis, or AVN |
| Leg length discrepancy | Mild shortening |
| Femoral neck fracture | After pinning (rare) |
Complications of Surgery
| Complication | Notes |
|---|---|
| Screw penetration | Chondrolysis, synovitis, OA |
| Osteonecrosis post-op | In unstable slips, esp. after reduction attempts |
| Femoral nerve injury | Anterior approach |
| Infection | Post-operative |
10. BLOOD SUPPLY OF FEMORAL HEAD (Key for understanding AVN)
Main blood supply to femoral head in adolescent:
→ LATERAL EPIPHYSEAL VESSELS
(terminal branches of MEDIAL FEMORAL CIRCUMFLEX ARTERY - deep branch)
These vessels run:
- Posterior and superior to femoral neck
- Enter epiphysis at the epiphyseal tubercle
- Supply the lateral 2/3 of femoral head
In SCFE:
- Stable slips: vessels stretch but remain intact → low AVN risk
- Unstable slips: vessels avulsed/compressed → high AVN risk (~47%)
- Forced reduction: can further compromise these vessels → DO NOT REDUCE
11. SCFE AND FAI
- Residual deformity after SCFE → prominent anterior femoral neck (metaphysis) = cam-type FAI
- During flexion and internal rotation: cam lesion impinges on acetabular rim → cartilage damage → early OA
- Management: Osteochondroplasty (after physeal closure) - arthroscopic or open
- Modified Dunn procedure aims to prevent this by anatomical realignment
12. QUICK REVISION TABLE
| Feature | Key Fact |
|---|---|
| Definition | Salter-Harris Type I injury; epiphysis (head) stays put, metaphysis (neck) moves anterosuperiorly |
| Commonest adolescent hip disorder | Yes |
| Peak age | 10-16 years |
| Sex | Boys > Girls (2:1) |
| Incidence | ~5 per 100,000 |
| Atypical if | Age <10 or >16, thin patient → investigate endocrine cause |
| Bilateral occurrence | 25-40%; up to 50% in Afro-Caribbean |
| Commonest site of pain | Knee (referred!) |
| Pathognomonic sign | Drehmann sign (ER on hip flexion) |
| Klein's line | Drawn along superior femoral neck - fails to intersect head in SCFE |
| Blanch sign (Steel) | Double density at metaphysis on AP |
| Most sensitive view | Frog-leg lateral |
| Southwick angle | Lateral view; mild <30°, mod 30-60°, severe >60° |
| Loder stable | Can walk; AVN 0% |
| Loder unstable | Cannot walk; AVN 47%; surgical EMERGENCY |
| Standard treatment | Single cannulated screw in situ fixation |
| Screw position | Centre-centre, ≥4 mm from subchondral bone |
| Capsulotomy | Yes, for acute/unstable (reduces tamponade) |
| Do NOT do | Forceful reduction of stable/chronic slips |
| Modified Dunn | For moderate/severe; surgical dislocation + realignment; only experienced surgeons |
| Late complication | Cam FAI → OA |
| Most feared complication | AVN |
13. EXAM WRITING TIPS
For a long-answer question on SCFE:
- Definition + anatomy (what actually slips and why the name is a misnomer)
- Incidence + epidemiology
- Aetiology (mechanical + endocrine/predisposing factors)
- Pathology (which zone of physis, direction of slip)
- Classification (Duration: acute/chronic/acute-on-chronic; Loder: stable/unstable; Grade: mild/mod/severe)
- Clinical features (pain at knee - Hilton's law, Drehmann sign, ER deformity)
- Investigations (AP + frog lateral; Klein's line; Blanch sign; Southwick angle)
- Treatment (based on Loder classification + severity)
- Complications (AVN, chondrolysis, FAI, OA)
- Bilateral SCFE and prophylactic pinning
Examiner favourites:
- "A 12-year-old boy presents with knee pain - what do you do?" → Examine the hip; take AP + frog lateral pelvis
- "What is Drehmann's sign?" → Obligatory ER on hip flexion
- "What is Klein's line?" → Line along superior femoral neck; fails to transect head in SCFE
- "What is the single most important classification?" → Loder (stable vs unstable)
- "What is the AVN risk in unstable SCFE?" → ~47%
- "Why not reduce a chronic stable slip?" → High AVN risk with manipulation; outcomes of in situ fixation are good
- "What is the modified Dunn procedure?" → Surgical dislocation + neck osteotomy + realignment; preserves MFCA blood supply
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 (Ch 38) | Bailey & Love's Short Practice of Surgery 28th Ed (Ch 44) | Grainger & Allison's Diagnostic Radiology (Ch 73) | Schwartz's Principles of Surgery 11th Ed | Rockwood & Green's Fractures in Adults 10th Ed 2025 | PubMed 2021-2026
Note: Turek's Orthopaedics and Tuli's Textbook of Orthopaedics were not available in the digital library. Classic concepts from these texts are well incorporated in Campbell's and are covered throughout these notes. If you have specific Tuli or Turek content in mind, please let me know and I can address those points from my knowledge base.
This is a shared conversation. Sign in to Orris to start your own chat.