What is differential between gynec pateint and obs pateint?
Reading File
Finding Sources
Searching the Web
difference between gynecology patient and obstetrics patient clinical
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here is a thorough breakdown of the differential between a gynecology (gynec) patient and an obstetrics (obs) patient:
Gynecology (Gynec) Patient vs. Obstetrics (Obs) Patient
1. Core Definition
| Feature | Gynecology Patient | Obstetrics Patient |
|---|---|---|
| Definition | A woman presenting with disorders/conditions of the female reproductive system, NOT related to pregnancy | A woman who is currently pregnant, in labor, delivering, or in the postpartum period (up to 6 weeks after delivery) |
| Pregnancy status | Not pregnant (or incidentally pregnant with a non-obs complaint) | Pregnant or recently delivered |
| Age range | Any female - from adolescence (menarche) to post-menopause | Reproductive age (typically 15-45 years) |
2. Chief Complaints
| Gynecology Patient | Obstetrics Patient |
|---|---|
| Abnormal uterine bleeding (AUB) | Missed period / confirmed pregnancy |
| Pelvic pain (chronic or acute) | Nausea/vomiting of pregnancy |
| Vaginal discharge / infections | Reduced fetal movements |
| Infertility / subfertility | Bleeding in pregnancy (APH/PPH) |
| Uterine fibroids / polyps | Hypertension in pregnancy / pre-eclampsia |
| Ovarian cysts / PCOS | Preterm labor or PROM |
| Endometriosis | Labor pains / contractions |
| Prolapse (uterine/vaginal) | Post-dates pregnancy |
| Cervical / ovarian / uterine cancer | Postpartum complications |
| Contraception needs | Gestational diabetes |
| Menopause symptoms | Intrauterine growth restriction (IUGR) |
| Sexual health / STIs | Fetal anomalies detected on scan |
3. Clinical Assessment Differences
| Parameter | Gynecology | Obstetrics |
|---|---|---|
| History focus | Menstrual history, sexual history, contraception, LMP, prior surgeries | LMP, gestational age (GA), EDD, ANC history, fetal movements, mode of previous deliveries |
| Examination | Per speculum (PS) exam, per vaginal (PV) exam, bimanual palpation | Abdominal palpation (fundal height, lie, presentation, engagement), FHR auscultation, PS/PV only when indicated |
| Key vital | BP, weight, temperature | BP (for pre-eclampsia), pulse, fetal heart rate (FHR) |
| Key investigation | Ultrasound (pelvic), Pap smear, hormone panels (FSH, LH, TSH), STI swabs | Obstetric ultrasound (fetal biometry, AFI, placental position), urine for protein, CBC, blood group |
| Two patients? | Only the woman | The woman AND the fetus (dual patient concept) |
4. Conditions Managed
| Gynecology | Obstetrics |
|---|---|
| PCOS, endometriosis, adenomyosis | Normal pregnancy surveillance (ANC) |
| Fibroids, polyps | Hyperemesis gravidarum |
| Ectopic pregnancy (unruptured/ruptured) | Ectopic pregnancy (before rupture, in some centers) |
| PID, vaginitis, cervicitis | APH (antepartum hemorrhage) - placenta previa, abruption |
| Cervical intraepithelial neoplasia (CIN) | PPH (postpartum hemorrhage) |
| Ovarian torsion, rupture | Pre-eclampsia, eclampsia |
| Uterovaginal prolapse | Gestational hypertension / gestational diabetes |
| Contraception (IUCD, implant, sterilization) | Preterm labor, PPROM |
| Menopause management | Intrapartum fetal monitoring |
| Gynecological cancers | Perineal tears, episiotomy repair |
| Pelvic floor disorders | Postpartum care (lactation, wound care) |
5. Management Philosophy
| Aspect | Gynecology | Obstetrics |
|---|---|---|
| Primary concern | The woman's reproductive / hormonal health | Safety of both the mother and the fetus |
| Drug safety | Standard drug prescribing | ALL drugs assessed for teratogenicity and fetal safety |
| Radiation / imaging | CT/X-ray freely used when indicated | Radiation minimized; MRI/ultrasound preferred |
| Surgery | Elective or urgent based on diagnosis | Surgery has added risks in pregnancy; timing and gestational age matter |
| Monitoring | Standard clinical follow-up | Fetal surveillance (CTG, BPP, Doppler) added |
6. Ward / Setting Differences
| Gynecology | Obstetrics | |
|---|---|---|
| Ward | Gynecology ward | Antenatal ward / Labour room / Postnatal ward |
| Equipment | Colposcope, hysteroscope, laparoscopy suite | CTG machine, delivery table, neonatal resuscitation trolley |
| Team involvement | Gynecologist, oncologist (if cancer) | Obstetrician, midwife, neonatologist/pediatrician |
| Consent specifics | Standard surgical/procedure consent | Consent covers maternal AND fetal risks |
Key Takeaway
The single most important differentiator is pregnancy. An obstetrics patient carries a fetus, making every clinical decision a dual-patient responsibility - the doctor must simultaneously protect the mother and the unborn baby. A gynecology patient is managed solely for her own reproductive health, and treatment decisions do not carry fetal considerations.
In most hospitals, OB/GYN is practiced as a combined specialty, but the clinical approach, ward setting, investigations, and management philosophy are distinctly different based on whether the patient is pregnant or not.
What is NST in gynecologist?
Finding Sources
Searching the Web
NST non-stress test obstetrics interpretation reactive nonreactive
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Here is a complete explanation of NST:
NST - Non-Stress Test
What is it?
The Non-Stress Test (NST) is a non-invasive antenatal fetal surveillance test that records fetal heart rate (FHR) and its response to fetal movements using an external cardiotocograph (CTG) monitor. It is called "non-stress" because no stress or risk is placed on the fetus - there are no contractions induced and no drugs given.
It was introduced in the USA in the early 1970s and remains the workhorse of antenatal fetal surveillance in obstetrics.
Pfenninger and Fowler's Procedures for Primary Care
Why is it Done? - Indications
NST is used to monitor high-risk pregnancies, generally from 32 weeks' gestation (some centers start at 26 weeks):
| Indication | Detail |
|---|---|
| IUGR (Intrauterine Growth Restriction) | First-line + umbilical artery Doppler |
| Gestational or pre-existing diabetes | Twice-weekly testing |
| Hypertensive disorders (GH, pre-eclampsia) | More frequent if severe |
| Post-term / prolonged pregnancy | Daily or twice-weekly |
| Decreased fetal movements | Immediate indication |
| Maternal renal disease | Ongoing monitoring |
| Multiple gestation | Regular surveillance |
| Prior fetal demise | Close monitoring |
| Maternal trauma | Acute assessment |
How is it Done? - Technique
- Patient sits in a semi-recumbent (semi-Fowler's) position, tilted slightly left to avoid supine hypotension
- External CTG monitors are applied:
- Tocodynamometer (records uterine contractions)
- Doppler probe (records fetal heart rate)
- Patient marks each fetal movement by pressing a button
- Monitoring runs for a baseline 30-minute period
- If non-reactive, extend to a second or third 30-minute period (up to 90 minutes total)
- If still insufficient movement, a vibroacoustic stimulator (VAS) - like an artificial larynx - can be applied to the maternal abdomen for 3 seconds (up to 3 times) to stimulate the fetus
Interpretation of Results
Reactive NST (NORMAL / REASSURING)
- 2 or more FHR accelerations within 20 minutes
- Each acceleration must peak at least 15 bpm above baseline
- Each must last at least 15 seconds
For fetuses <32 weeks: criteria are relaxed - 10 bpm above baseline lasting 10 seconds is considered reactive
Non-Reactive NST (ABNORMAL)
- No qualifying accelerations within 40 minutes of monitoring
- Most common cause: fetal sleep cycle (not pathological)
- Other causes: narcotics/sedatives, maternal hypoglycemia, maternal smoking, fetal anomalies, fetal hypoxia
NST Tracing - Reactive vs Non-Reactive
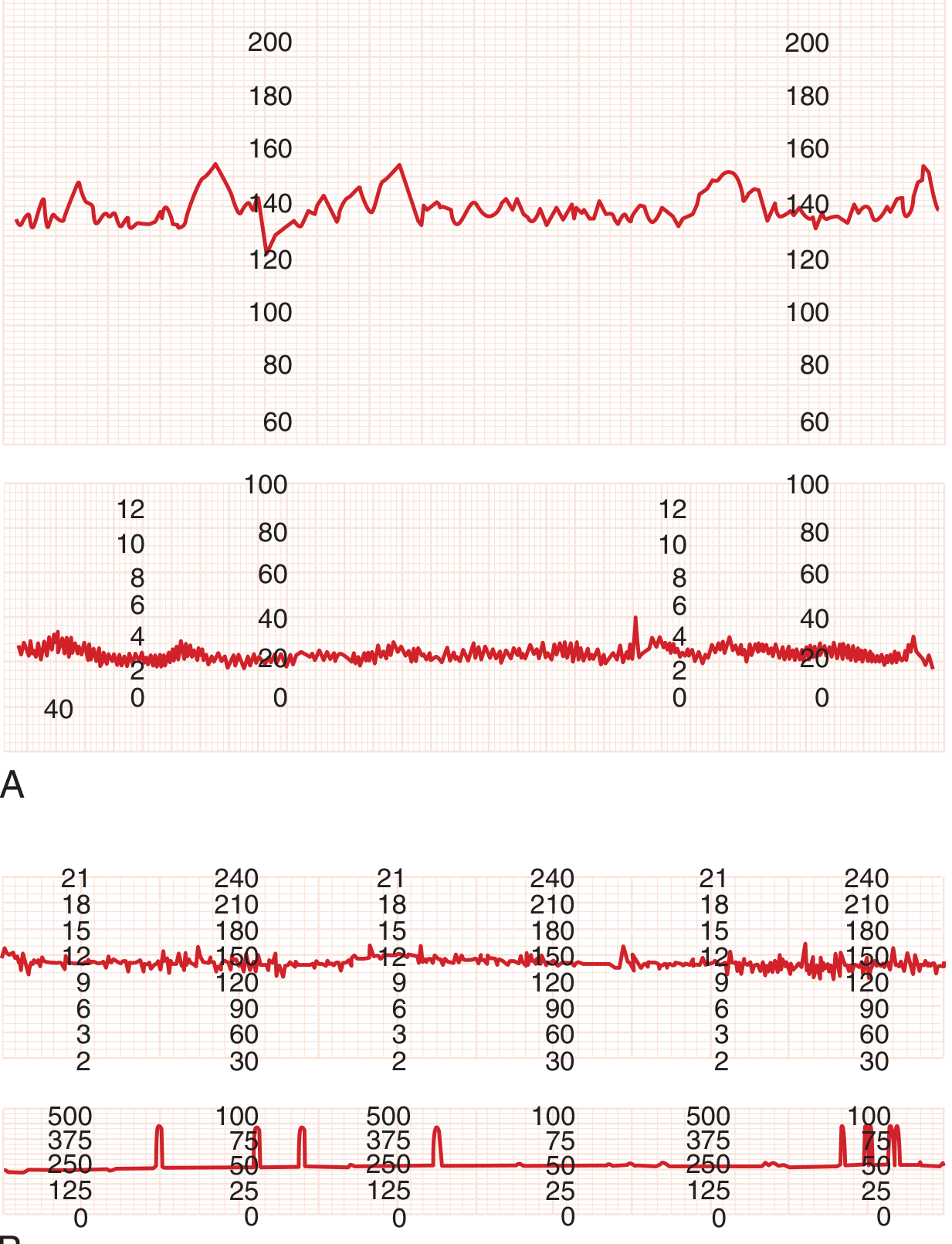
Panel A (top): Reactive NST - notice the FHR accelerations (peaks) corresponding to fetal movements. Panel B (bottom): Non-reactive NST - flat FHR with no significant accelerations.
What to Do Next - Management After NST
| Result | Action |
|---|---|
| Reactive | Reassuring; repeat as per clinical indication (weekly or twice weekly) |
| Non-reactive | Extend monitoring to 90 min; use VAS; check maternal BP |
| Still non-reactive | Proceed to Biophysical Profile (BPP) or Modified BPP (NST + AFI) |
| Non-reactive + oligohydramnios | High risk - consider delivery if mature |
| Variable decelerations on reactive NST | Measure amniotic fluid index (AFI) - risk of cord compromise |
Modified BPP
NST + Amniotic Fluid Index (AFI) = Modified BPP
- Takes only ~10 minutes
- False-negative rate: 0.8 per 1000 (very sensitive)
- ACOG-endorsed for antepartum monitoring
- Most centers perform this twice weekly in high-risk pregnancies
Key Points to Remember
| Feature | Value |
|---|---|
| Test type | Non-invasive, external CTG |
| Gestational age | From 32 weeks (or 26 weeks in some centers) |
| Duration | 20-90 minutes |
| Reactive criteria (>32 wks) | 2 accelerations, ≥15 bpm, ≥15 sec, in 20 min |
| Reactive criteria (<32 wks) | 2 accelerations, ≥10 bpm, ≥10 sec, in 20 min |
| False-positive rate | High (15-69% depending on indication) |
| False-negative rate (reactive) | Very low (2 per 1000) |
| Contraindications | None specific |
Bottom line: NST is a quick, safe, non-invasive test to assess fetal well-being. A reactive NST is reassuring that the fetus is well-oxygenated. A non-reactive NST requires further evaluation but does not automatically mean the baby is in danger - fetal sleep is the most common cause.
Different conditions in NST
Finding Sources
Searching the Web
NST non-stress test patterns conditions reactive nonreactive sinusoidal decelerations classification
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete breakdown of all the different conditions/patterns seen on NST (Non-Stress Test) and fetal heart rate (FHR) monitoring:
Different Conditions/Patterns on NST
NST traces are classified based on two main features:
- Baseline FHR (rate + variability)
- Periodic changes (accelerations and decelerations)
1. REACTIVE NST (Normal / Reassuring)
| Feature | Criteria |
|---|---|
| FHR accelerations | 2 or more in 20 minutes |
| Height | Peak ≥15 bpm above baseline |
| Duration | Last ≥15 seconds |
| Baseline | 110-160 bpm with moderate variability |
- Interpretation: Fetus is well-oxygenated; healthy autonomic nervous system
- Action: Continue routine monitoring
For fetuses <32 weeks: Criteria are 10 bpm above baseline for 10 seconds
2. NON-REACTIVE NST (Abnormal / Non-Reassuring)
| Feature | Description |
|---|---|
| Accelerations | Absent or fewer than 2 qualifying accelerations in 40 minutes |
| Most common cause | Fetal sleep cycle (normal, lasts 20-40 min) |
Other causes of non-reactive NST:
- Maternal narcotics / sedatives / barbiturates
- Maternal hypoglycemia
- Maternal smoking
- Extreme prematurity (<26 weeks)
- Fetal cardiac anomaly / heart block
- Fetal CNS anomaly
- Fetal hypoxia / acidemia
Action: Extend monitoring to 90 min; use vibroacoustic stimulator (VAS); if still non-reactive → proceed to BPP or CST
3. FHR VARIABILITY PATTERNS
Variability reflects the beat-to-beat irregularity of FHR - a sign of healthy autonomic nervous system function.
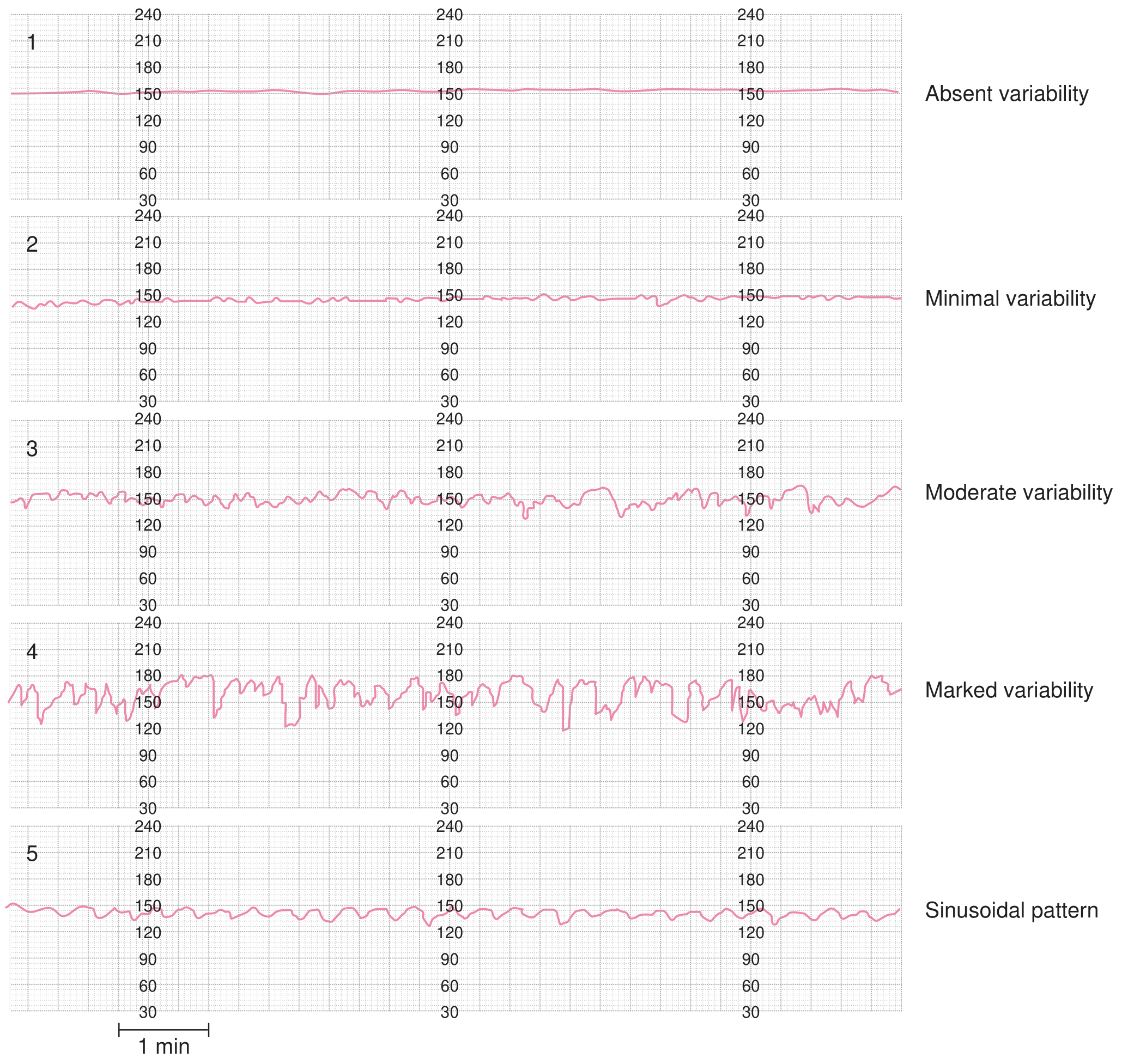
Patterns 1-5: Absent, Minimal, Moderate (normal), Marked variability, and Sinusoidal pattern
| Type | Amplitude | Meaning |
|---|---|---|
| Absent | Undetectable (0 bpm) | Most ominous - fetal hypoxia, acidemia |
| Minimal | 1-5 bpm | Concerning - hypoxia, drugs, sleep |
| Moderate (Normal) | 6-25 bpm | Reassuring - healthy fetus |
| Marked | >25 bpm | May indicate cord compression or early hypoxia |
4. FHR DECELERATION PATTERNS
A. Early Decelerations (Benign)
- Shape: Mirror image of contraction (U-shaped, gradual onset)
- Timing: Onset, nadir, recovery all coincide with the contraction
- Cause: Fetal head compression during uterine contraction → vagal reflex
- Clinical significance: Benign - not associated with hypoxia or acidemia
- Action: No intervention needed
B. Variable Decelerations (Most Common - Cord Compression)
- Shape: Abrupt drop - variable "V", "U" or "W" shapes
- Timing: Variable relationship to contractions
- Cause: Umbilical cord compression (nuchal cord, short cord, cord prolapse, oligohydramnios)
- Frequency: Most common deceleration type - 50-80% of all deliveries
Classification by severity:
| Severity | Depth | Duration |
|---|---|---|
| Mild | >80 bpm nadir | <30 seconds |
| Moderate | 70-80 bpm nadir | 30-60 seconds |
| Severe | <70 bpm nadir | >60 seconds |
- Reassuring sign: "Shoulders" (brief accelerations before and after the dip) = healthy response
- Action: Reposition patient; if recurrent with absent variability → Category III (urgent)
C. Late Decelerations (Ominous - Uteroplacental Insufficiency)
- Shape: Gradual, smooth descent and slow return
- Timing: Onset after the contraction peak; nadir comes after the contraction peak; return after contraction ends
- Cause: Uteroplacental insufficiency - reduced uterine blood flow or placental dysfunction
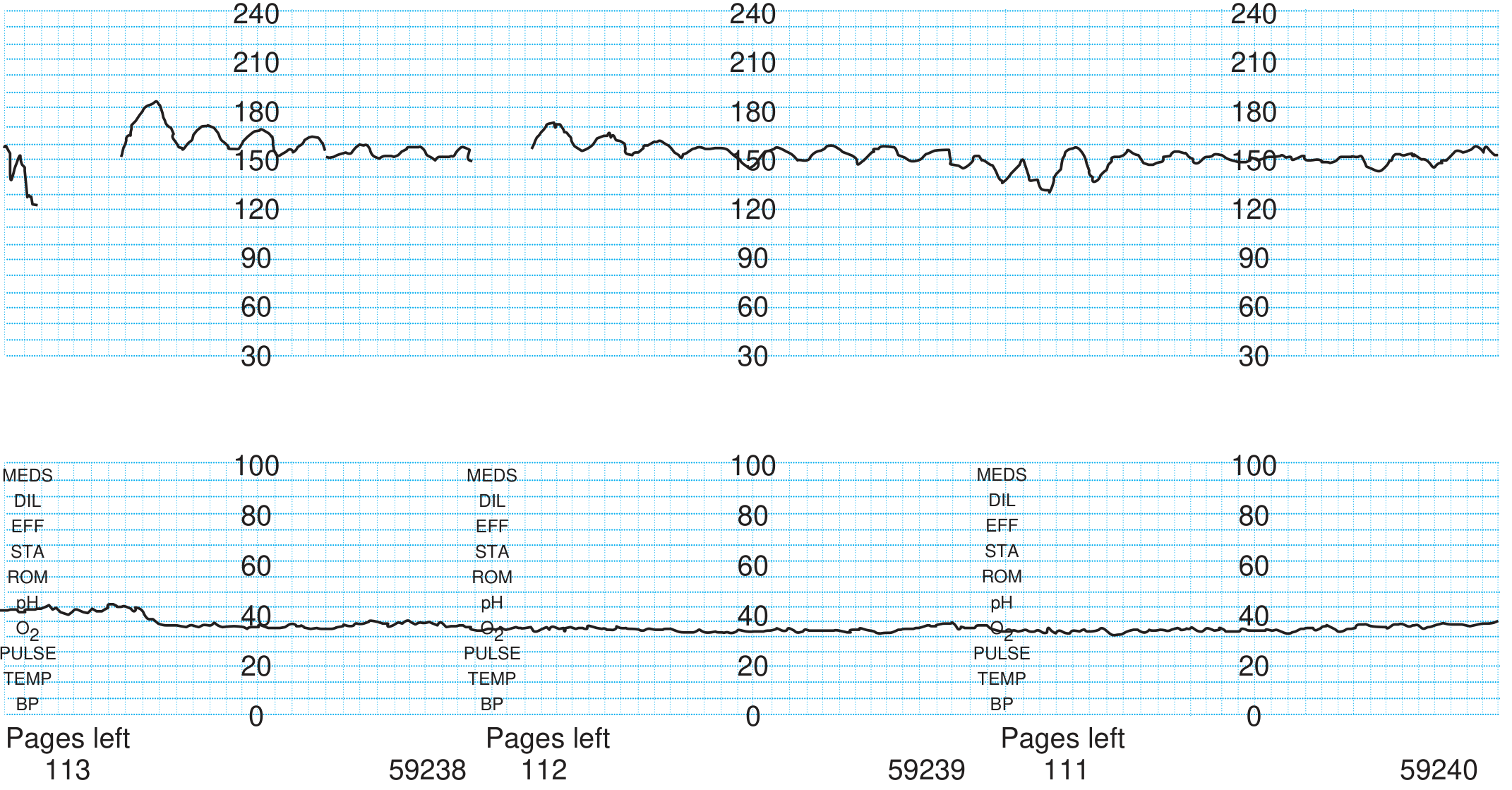
Sinusoidal FHR pattern - a smooth, undulating sine-wave; one of the most ominous findings
Common causes of late decelerations:
- Pre-eclampsia / chronic hypertension
- Gestational / Type 1 diabetes
- Post-dates pregnancy (placental aging)
- Maternal hypotension (e.g., after epidural/spinal)
- Oxytocin overstimulation (tachysystole)
Management:
- Turn patient to left lateral position
- IV fluids to correct hypotension
- Stop oxytocin
- Administer O2 by face mask
- If persistent → urgent delivery
D. Prolonged Deceleration
- FHR drop >15 bpm lasting >2 minutes but <10 minutes
- Beyond 10 minutes = new baseline (bradycardia)
- Causes: cord prolapse, tetanic contraction, maternal seizure, rapid fetal descent
- Action: Urgent assessment; intrauterine resuscitation
5. SINUSOIDAL PATTERN (Most Ominous)
- Shape: Smooth, uniform, undulating sine-wave
- Frequency: 2-6 cycles/min
- Amplitude: 5-30 bpm
- Duration: Persists for ≥20 minutes
- Key feature: Complete absence of beat-to-beat variability
Causes:
- Severe fetal anemia (Rh alloimmunization - fetal Hct <20%)
- Fetal hydrops
- Severe fetal hypoxia
- Also seen (pseudo-sinusoidal) after maternal narcotic administration (butorphanol, morphine) - benign
Action: Rapid intervention - fetal blood sampling, intrauterine transfusion, or emergency delivery
6. BASELINE RATE ABNORMALITIES
| Condition | Rate | Causes |
|---|---|---|
| Tachycardia | >160 bpm | Chorioamnionitis, maternal fever, fetal infection, hyperthyroidism, sympathomimetics (terbutaline), fetal hypoxia, prematurity |
| Bradycardia | <110 bpm | Cord compression/prolapse, heart block (structural anomaly), severe hypoxia, epidural/spinal, tetanic contractions |
NICHHD Three-Category Classification (Summary)
| Category | Features | Interpretation |
|---|---|---|
| I (Normal) | Baseline 110-160 bpm, moderate variability, no late/variable decelerations, accelerations present/absent | Reassuring - routine care |
| II (Indeterminate) | Everything not in Category I or III (e.g., tachycardia, minimal variability, absent accelerations after stimulation, recurrent variables with moderate variability) | Uncertain - close monitoring, further evaluation |
| III (Abnormal) | Absent variability + recurrent late/variable decelerations OR bradycardia; OR sinusoidal pattern | Non-reassuring - immediate intervention |
Quick Memory Summary
| Pattern | Key Feature | Cause | Urgency |
|---|---|---|---|
| Reactive | 2 accels ≥15 bpm × 15 sec | Healthy fetus | Reassuring |
| Non-reactive | No accels in 40 min | Sleep, drugs, hypoxia | Further evaluation |
| Early decel | Mirror of contraction | Head compression | Benign |
| Variable decel | Abrupt, V/U/W shape | Cord compression | Monitor severity |
| Late decel | After peak of contraction | Placental insufficiency | Urgent |
| Sinusoidal | Smooth sine wave, no variability | Severe anemia/hypoxia | Emergency |
| Absent variability | Flat line | Severe hypoxia/acidemia | Emergency |
Creasy & Resnik's Maternal-Fetal Medicine; Textbook of Family Medicine 9e; Pfenninger and Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.