Oral antidiabetic drugs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from the Lippincott Pharmacology textbook. Let me compile the full answer.
Oral Antidiabetic Drugs
Oral antidiabetic (hypoglycemic) agents are used primarily in type 2 diabetes mellitus, which is characterized by insulin resistance and insufficient insulin secretion. Patients who have had diabetes for less than 5 years are most likely to respond well to oral agents. Long-standing disease may require combination therapy.
Classes of Oral Antidiabetic Agents
I. Biguanides - Metformin
Metformin is the preferred initial agent for type 2 diabetes and should be started at diagnosis.
| Property | Details |
|---|---|
| Mechanism | Reduces hepatic gluconeogenesis (primary); slows intestinal glucose absorption; improves peripheral insulin sensitivity |
| Does NOT | Stimulate insulin secretion - so very low risk of hypoglycemia alone |
| PK | Well absorbed orally; not protein bound; not metabolized; excreted unchanged in urine |
| Adverse effects | GI: diarrhea, nausea, vomiting (take with meals, titrate slowly); weight loss/appetite suppression; lactic acidosis (rare but serious) |
| Contraindications | Severe renal impairment (eGFR <30 mL/min), acute heart failure, hepatic failure - all due to lactic acidosis risk |
| Other uses | Polycystic ovary syndrome (PCOS), prediabetes prevention |
Also useful in PCOS by reducing insulin resistance. - Lippincott Illustrated Reviews: Pharmacology
II. Sulfonylureas (Insulin Secretagogues)
Examples: Tolbutamide, glipizide, glyburide (glibenclamide), glimepiride, glibenclamide (1st gen: chlorpropamide)
| Property | Details |
|---|---|
| Mechanism | Bind ATP-sensitive K⁺ channels on pancreatic B cells → close channels → membrane depolarization → Ca²⁺ influx → insulin exocytosis |
| Requirement | Some residual B cell function; ineffective in type 1 diabetes or post-pancreatectomy |
| Adverse effects | Hypoglycemia (main concern), weight gain |
| Other | Low cost; effective; second-line after metformin |
Tolbutamide and other sulfonylureas only work in patients with some remaining B cells and are ineffective after pancreatectomy or in type 1 diabetes. - Ganong's Review of Medical Physiology
III. Meglitinides (Short-acting Secretagogues)
Examples: Repaglinide, nateglinide
| Property | Details |
|---|---|
| Mechanism | Same as sulfonylureas (close K⁺-ATP channels) but short-acting - taken before meals |
| Benefit | Better postprandial glucose control with flexible dosing |
| Adverse effects | Hypoglycemia (less than sulfonylureas), weight gain |
IV. Thiazolidinediones (TZDs) - "Glitazones"
Examples: Pioglitazone, rosiglitazone
| Property | Details |
|---|---|
| Mechanism | Activate PPAR-γ (peroxisome proliferator-activated receptor gamma) in adipose tissue → increased insulin sensitivity in muscle, fat, and liver |
| Effect | Do not stimulate insulin secretion; reduce insulin resistance |
| Adverse effects | Weight gain, fluid retention/edema, increased risk of heart failure (avoid in HF), increased fracture risk |
| Pioglitazone note | Associated with bladder cancer risk (long-term use) |
V. Alpha-Glucosidase Inhibitors
Examples: Acarbose, miglitol
| Property | Details |
|---|---|
| Mechanism | Inhibit intestinal alpha-glucosidase enzymes → delay carbohydrate digestion and absorption → reduce postprandial glucose spikes |
| Adverse effects | GI disturbance: flatulence, diarrhea, abdominal cramps (very common) |
| Benefit | No hypoglycemia alone; weight neutral |
VI. DPP-4 Inhibitors ("Gliptins")
Examples: Sitagliptin, saxagliptin, alogliptin, linagliptin
| Property | Details |
|---|---|
| Mechanism | Inhibit dipeptidyl peptidase-4 (DPP-4), the enzyme that degrades incretin hormones (GLP-1, GIP) → increased GLP-1 levels → glucose-dependent insulin secretion and glucagon suppression |
| Benefit | Low hypoglycemia risk; weight neutral |
| Adverse effects | Nasopharyngitis, risk of pancreatitis (rare) |
| Cardiovascular | Generally neutral; saxagliptin associated with increased HF hospitalization |
VII. SGLT2 Inhibitors ("Gliflozins")
Examples: Empagliflozin, dapagliflozin, canagliflozin, ertugliflozin
| Property | Details |
|---|---|
| Mechanism | Inhibit sodium-glucose cotransporter 2 (SGLT2) in the proximal renal tubule → block glucose reabsorption → glucosuria |
| Benefits | Weight loss, blood pressure reduction, cardiovascular mortality reduction (empagliflozin, dapagliflozin), renal protection in CKD |
| Adverse effects | Urinary tract infections, genital mycotic infections, polyuria, rare diabetic ketoacidosis (euglycemic DKA) |
| Contraindication | eGFR <45 mL/min for most agents (reduced efficacy + safety concerns) |
VIII. Oral GLP-1 Receptor Agonist
Example: Semaglutide (oral formulation - Rybelsus)
| Property | Details |
|---|---|
| Mechanism | GLP-1 receptor agonist - glucose-dependent insulin secretion, glucagon suppression, delayed gastric emptying, satiety |
| Benefits | Weight loss, cardiovascular protection |
| Adverse effects | Nausea, vomiting, diarrhea |
Adverse Effects Summary
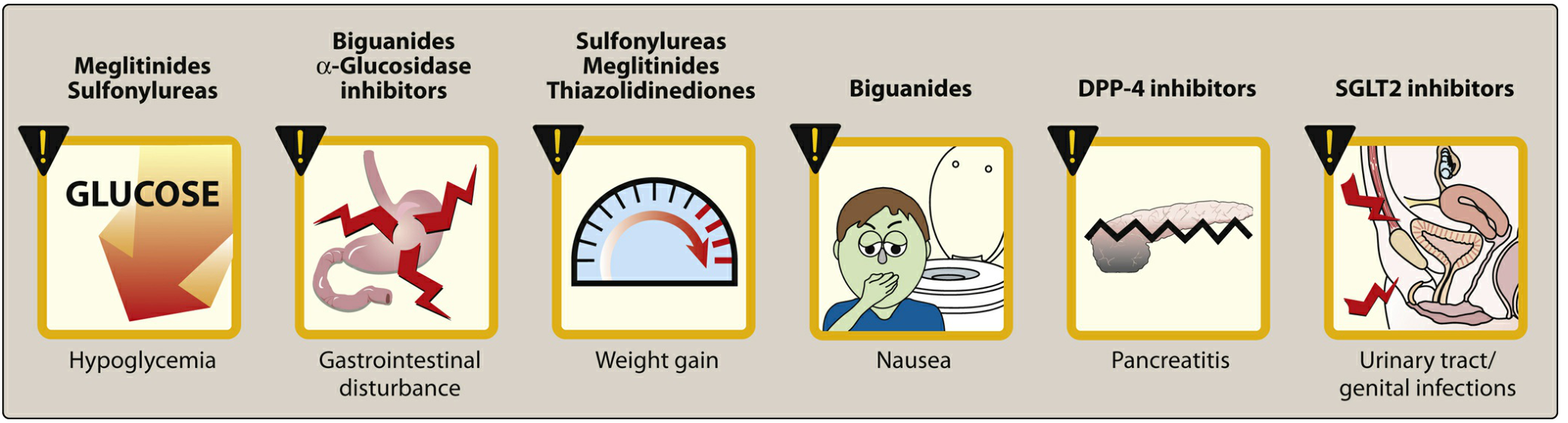
Figure: Key adverse effects by drug class - Lippincott Illustrated Reviews: Pharmacology
Treatment Algorithm for Type 2 Diabetes
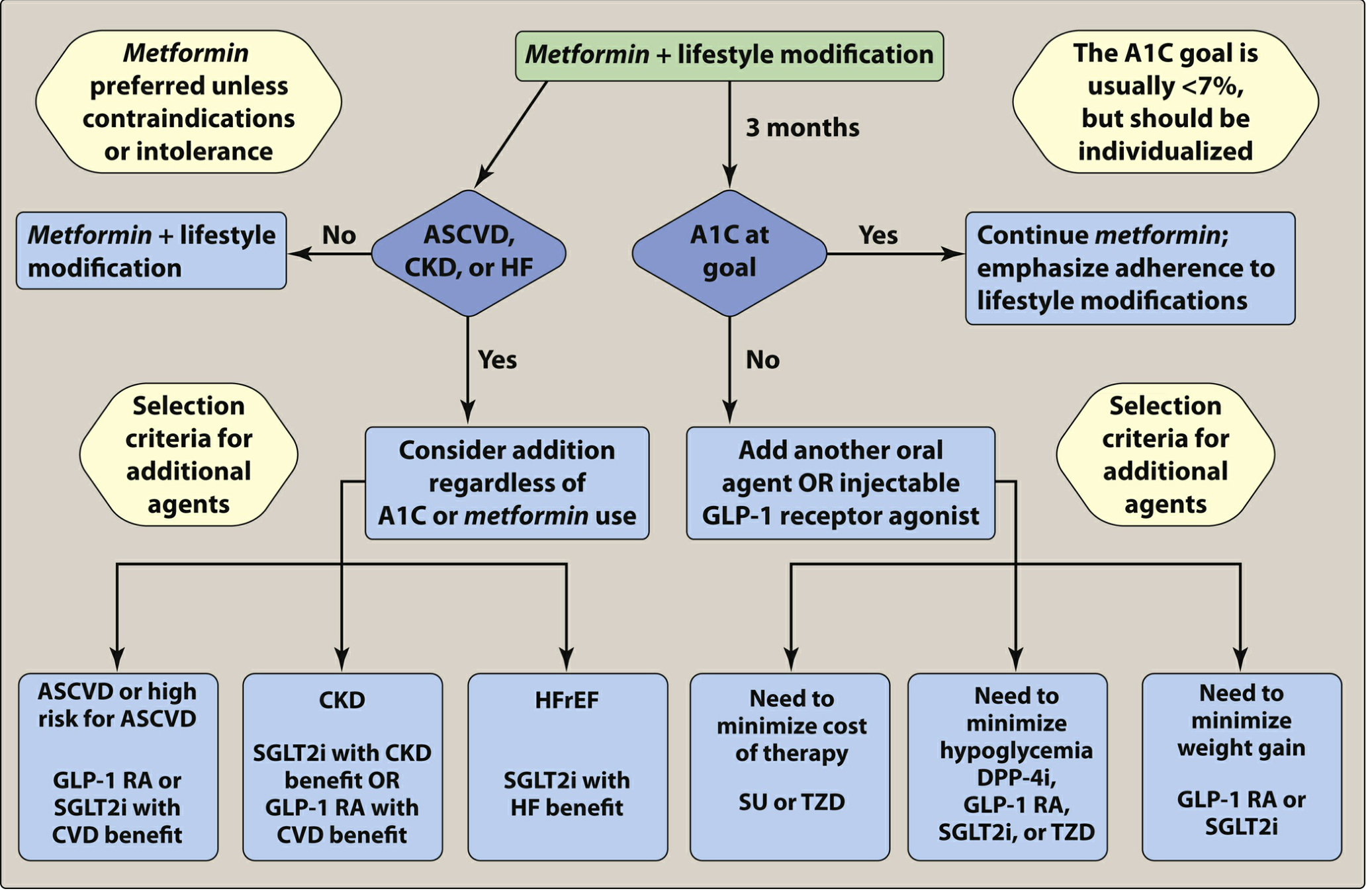
Figure: Recommendations for management of type 2 diabetes - Lippincott Illustrated Reviews: Pharmacology
Key decision points:
- Start with metformin + lifestyle (unless contraindicated)
- If A1C not at goal after 3 months, add a second agent
- If ASCVD or high CV risk: add GLP-1 RA or SGLT2i with proven CV benefit
- If CKD: add SGLT2i (renal benefit) or GLP-1 RA
- If HFrEF: add SGLT2i with heart failure benefit
- If minimizing hypoglycemia: prefer DPP-4i, GLP-1 RA, SGLT2i, or TZD
- If minimizing weight gain: prefer GLP-1 RA or SGLT2i
Quick Comparison Table
| Drug Class | MOA | Hypoglycemia | Weight | CV Benefit | Notes |
|---|---|---|---|---|---|
| Metformin | ↓ hepatic gluconeogenesis | Low | Loss | Neutral | First-line; avoid in severe renal/hepatic failure |
| Sulfonylureas | Close K⁺-ATP channels → ↑ insulin | High | Gain | Neutral | Cheap; 2nd line |
| Meglitinides | Close K⁺-ATP channels (short) | Moderate | Gain | Neutral | Pre-meal dosing |
| TZDs | PPAR-γ activation | Low | Gain | Pioglitazone neutral | Avoid in HF |
| Alpha-glucosidase inhibitors | Delay GI absorption | Low | Neutral | Neutral | Mainly postprandial |
| DPP-4 inhibitors | ↑ incretin half-life | Low | Neutral | Neutral | Well tolerated |
| SGLT2 inhibitors | ↑ renal glucose excretion | Low | Loss | Yes (CV + renal) | Genital infections |
| Oral semaglutide | GLP-1 RA | Low | Loss | Yes | Nausea common |
Sources: Lippincott Illustrated Reviews: Pharmacology; Ganong's Review of Medical Physiology, 26th Edition
This is a shared conversation. Sign in to Orris to start your own chat.