HEART FAILURE: Pathophysiology, Diagnosis & Management
Harrison's Principles of Internal Medicine, 22E - Chapters 264 & 265
CHAPTER 264: HEART FAILURE - PATHOPHYSIOLOGY AND DIAGNOSIS
I. CLINICAL DEFINITIONS, EPIDEMIOLOGY, AND PHENOTYPES
DEFINITIONS
Heart Failure (HF) = A complex clinical syndrome with symptoms and signs resulting from any structural or functional impairment of ventricular filling or ejection of blood. (AHA/ACC/HFSA)
ESC Definition emphasizes: cardinal symptoms (breathlessness, ankle swelling, fatigue) + signs (elevated JVP, pulmonary crackles, peripheral edema) due to structural/functional abnormality causing elevated intracardiac pressures and/or inadequate cardiac output.
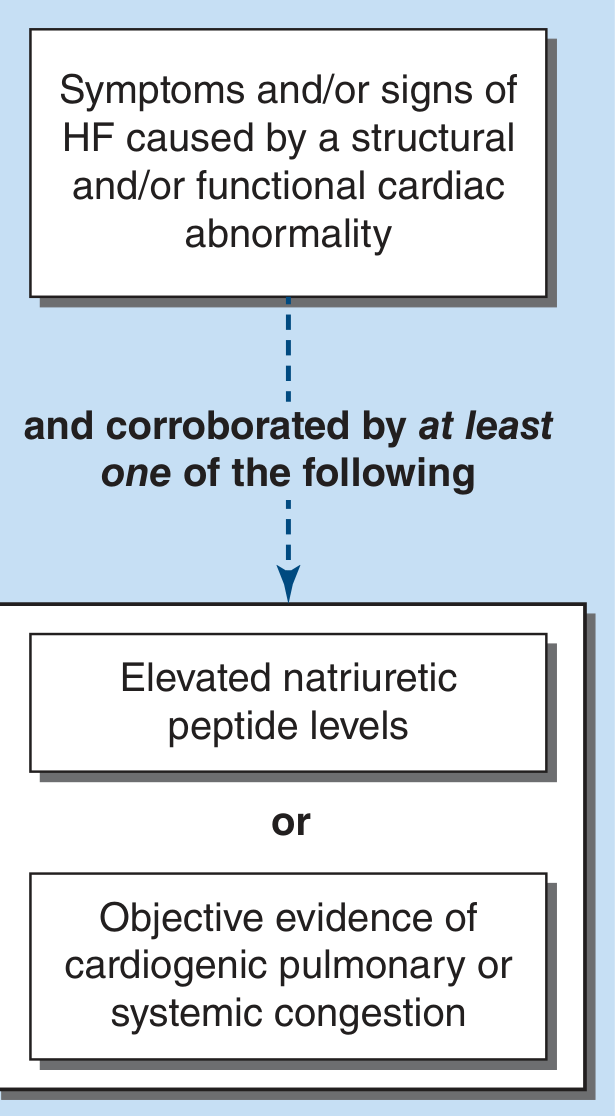
Universal Definition (2021): Symptoms and/or signs caused by a structural and/or functional cardiac abnormality, corroborated by at least ONE of:
- Elevated natriuretic peptide levels
- Objective evidence of cardiogenic pulmonary or systemic congestion
Figure 264-1: The contemporary universal definition of HF. Diagnosis requires symptoms/signs of HF caused by a cardiac abnormality, corroborated by elevated natriuretic peptides OR objective evidence of congestion.
Key terminological distinctions:
- Chronic HF = Longstanding (months-years) symptoms, on medical/device therapy; episodes of worsening = "decompensation"; resolution = "remission" (NOT stable, as risk persists)
- Acute HF (previously ADHF) = Rapid onset or worsening of symptoms; 80% = worsening chronic HF, ~20% = new-onset (ACS, acute valvular dysfunction, hypertensive urgency, postcardiotomy)
- Acute pulmonary edema = Rapidly worsening signs/symptoms of pulmonary congestion due to severe elevation of left heart filling pressures
- Prefer "heart failure" over "congestive heart failure"; "cardiomyopathy/LV dysfunction" are broader terms
EPIDEMIOLOGY
- US: ~6.7 million adults treated for HF; >600,000 new cases/year
- Global: ~56.2 million people affected worldwide
- Lifetime risk: ~20% for adults >45 years
- Prognosis: ~50% 5-year mortality despite advances; significant morbidity and healthcare costs
- HF is the leading cause of hospitalization in adults >65 years in the US
- PAR by race/ethnicity (HFpEF): Hypertension predominates in all groups; obesity and diabetes are increasing contributors especially in Hispanic/African American populations
TABLE 264-1: INDEPENDENT PREDICTORS OF ADVERSE OUTCOMES IN HEART FAILURE
| Category | Predictor |
|---|
| Demographic | Older age, male sex, non-white race |
| Clinical | NYHA class III-IV, prior HF hospitalization, low 6-minute walk distance |
| Vital Signs | Hypotension, tachycardia, low pulse pressure |
| Hemodynamic | Low cardiac index, elevated PCWP, low mixed venous O₂ saturation |
| Laboratory | Hyponatremia, worsening renal function (BUN/creatinine elevation), elevated bilirubin, anemia, hyperuricemia |
| Biomarkers | Elevated BNP/NTproBNP, elevated troponin, elevated ST2, elevated galectin-3 |
| Imaging | Reduced LVEF, dilated LV, RV dysfunction, severe MR, pulmonary hypertension |
| ECG | Wide QRS (LBBB), atrial fibrillation |
| Comorbidities | Diabetes mellitus, CKD, sleep apnea, depression |
PHENOTYPES: HFrEF vs. HFpEF vs. HFmrEF vs. HFrecEF
HFrEF (Heart Failure with Reduced Ejection Fraction)
- LVEF ≤40%
- Systolic dysfunction is predominant
- Evidence-based therapy most established
- Causes: ischemic (most common), dilated, myocarditis, toxic
HFpEF (Heart Failure with Preserved Ejection Fraction)
- LVEF ≥50%
- Normal or near-normal systolic function; diastolic dysfunction predominant
- Multiple pathophysiologic mechanisms: vascular stiffness, renal dysfunction, inflammation, oxidative stress, insulin resistance
- Comorbidities (HTN, obesity, DM, CKD, AF, sleep apnea) play major role
- ~50% of all HF; prognosis comparable to HFrEF
- Limited evidence-based therapy (SGLT-2i now proven beneficial)
HFmrEF (Heart Failure with Mildly Reduced Ejection Fraction)
- LVEF 41-49%
- Intermediate zone; heterogeneous population
- Some may recover EF (overlap with HFrecEF)
- SGLT-2i, ARNi show benefit in clinical trials
HFrecEF (Heart Failure with Recovered Ejection Fraction)
- Previously HFrEF, now LVEF >40% (often ≥50%)
- Following treatment (e.g., tachycardiomyopathy, peripartum CMP, toxic CMP)
- Despite recovery, continued GDMT is recommended - discontinuation risks relapse
- Better prognosis but NOT benign; residual risk persists
TABLE 264-2: SELECTED CAUSES OF HEART FAILURE
ACQUIRED CAUSES
| Category | Examples |
|---|
| Ischemic | CAD, MI, coronary microvascular disease |
| Hypertensive | Systemic hypertension, hypertensive CMP |
| Valvular | MR, AR, MS, AS, tricuspid disease |
| Inflammatory/Infectious | Viral myocarditis (Coxsackievirus B, COVID-19, HIV), Chagas disease, Lyme disease, sepsis-related CMP |
| Toxic/Drug-Induced | Alcohol, cocaine, methamphetamine, anthracyclines, trastuzumab, tyrosine kinase inhibitors, checkpoint inhibitors, radiation |
| Metabolic/Endocrine | Thyroid disease (hypo/hyper), acromegaly, Cushing's, diabetes |
| Nutritional Deficiency | Thiamine (beriberi), selenium, carnitine |
| Tachycardia-Induced | AF, incessant SVT, frequent PVCs |
| Peripartum | Peripartum cardiomyopathy |
| Stress-Induced | Takotsubo (stress) cardiomyopathy |
| Infiltrative (Acquired) | Amyloidosis (AL), sarcoidosis, hemochromatosis |
FAMILIAL/GENETIC CAUSES
| Category | Examples |
|---|
| Dilated CMP (familial) | TTN (titin) mutations (most common), LMNA, SCN5A, MYH7 |
| Hypertrophic CMP | MYH7, MYBPC3, TNNT2 (sarcomere genes) |
| ARVC | Desmosomal gene mutations (PKP2, DSP) |
| Muscular dystrophies | Duchenne, Becker (X-linked dystrophinopathy) |
| Channelopathies | Long QT, Brugada syndrome |
| Storage/Infiltrative (Familial) | ATTR amyloidosis (TTR mutations), Fabry's disease (GLA), Pompe disease |
CONGENITAL AND OTHER DISORDERS
| Category | Examples |
|---|
| Congenital Heart Disease | VSD, ASD (shunts), Ebstein's anomaly, complex CHD |
| High-Output States | Severe anemia, AV fistula, thyrotoxicosis, Paget's disease, wet beriberi, pregnancy |
| Pericardial Disease | Constrictive pericarditis (mimics HF) |
| RV Failure | Pulmonary arterial hypertension, pulmonary embolism, RV infarction |
II. PATHOPHYSIOLOGY
PROGRESSIVE DISEASE
HFrEF is a progressive disease involving an index event followed by months-to-years of structural and functional cardiovascular remodeling.
Index events may be:
- Sudden (acute MI)
- Gradual (chronic pressure/volume overload)
- Inherited (genetic CMP)
- Congenital
Patients may remain asymptomatic for prolonged periods due to compensatory mechanisms that ultimately contribute to disease progression.
VENTRICULAR REMODELING
Two patterns based on stimulus:
| Feature | Concentric Hypertrophy | Eccentric Hypertrophy |
|---|
| Stimulus | Pressure overload (HTN, AS) | Volume overload (AR, MR) |
| Mass vs Volume | Mass > chamber volume | Chamber volume increases |
| Purpose | Reduces wall stress | Accommodates increased volume |
| Outcome | Risk of diastolic dysfunction | Risk of systolic dysfunction, dilated CMP |
Cellular changes in remodeling:
- Myocyte hypertrophy and interstitial fibrosis
- Alterations in calcium-handling proteins and cytoskeletal proteins
- Molecular: re-expression of fetal genes
- Cell loss: necrosis, apoptosis (programmed cell death)
- Afterload mismatch from systemic vasoconstriction + loss of neurohormonal adaptation
- Feeds back on remodeling stimuli - vicious cycle
HFpEF mechanisms (beyond diastolic dysfunction):
- Vascular stiffness, renal dysfunction, sodium avidity
- Inflammation related to regional adiposity
- Oxidative stress, impaired nitric oxide signaling (nitrosative stress)
- Insulin resistance
- Autophagy dysfunction (autophagosomes - normally cytoprotective but unchecked = maladaptive)
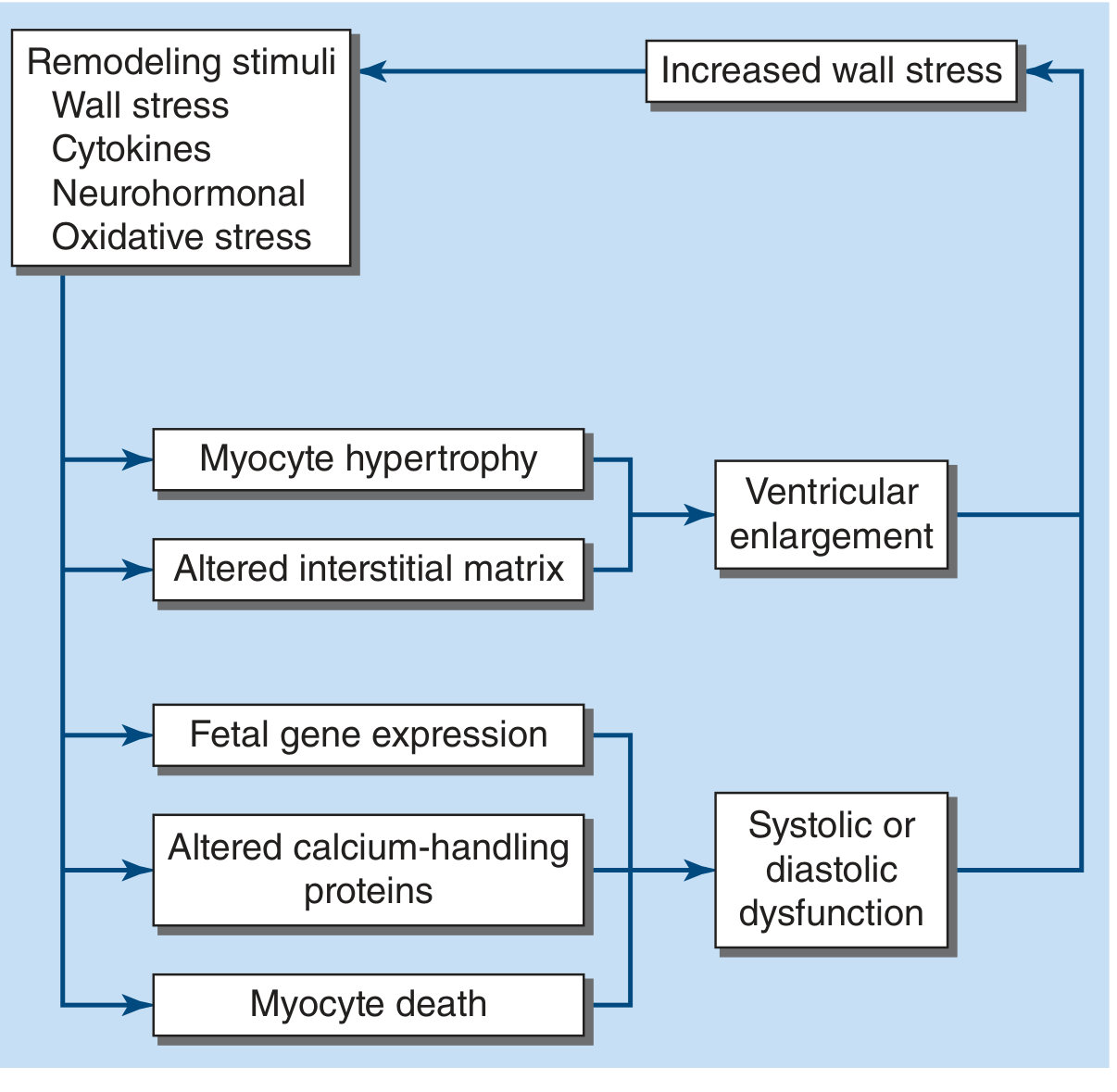
FIGURE 264-6: REMODELING STIMULI IN HEART FAILURE
Remodeling stimuli (wall stress, cytokines, neurohormonal signals, oxidative stress) lead to myocyte hypertrophy, altered interstitial matrix, fetal gene expression, altered calcium-handling proteins, and myocyte death. These produce ventricular enlargement and systolic/diastolic dysfunction, which increases wall stress - completing a vicious cycle.
MECHANISMS OF DISEASE PROGRESSION
Neurohormonal Activation
Sympathetic Nervous System (SNS) and RAAS are central drivers.
Initial compensation:
- Increased HR, BP, contractility
- Sodium/water retention to augment preload
- Maintains CO at rest and during exercise
Chronic unchecked activation leads to:
- Excessive vasoconstriction and volume retention
- Electrolyte/renal abnormalities
- Baroreceptor dysfunction
- Direct myocardial toxicity (norepinephrine, angiotensin II)
- Cardiac arrhythmias
- Ventricular remodeling (heart + blood vessels)
Key neurohormonal mediators:
| System | Effects |
|---|
| SNS (NE elevation) | Vasoconstriction, tachycardia, direct myocardial toxicity, arrhythmias |
| Angiotensin II | Vasoconstriction, aldosterone release, myocardial fibrosis, hypertrophy |
| Aldosterone | Na/water retention, K/Mg wasting, myocardial fibrosis |
| Vasopressin (ADH) | Water retention, hyponatremia |
| Endothelin-1 | Potent vasoconstriction, myocyte hypertrophy, pulmonary vasoconstriction |
Vasodilatory/Counter-Regulatory Hormones
Counter-regulatory mechanisms that are overwhelmed in HF:
- Natriuretic peptides (ANP, BNP): Vasodilation, natriuresis, anti-fibrotic, anti-hypertrophic; levels rise with wall stress - used as biomarkers
- Nitric oxide (NO): Vasodilation, anti-remodeling; impaired in HF (reduced NOS activity, increased ROS consumption)
- Prostaglandins: Vasodilatory, renoprotective
Endothelin
- ET-1 is a potent vasoconstrictor (>10x more potent than NE)
- Stimulates myocyte hypertrophy, fibrosis, and pulmonary vasoconstriction
- Elevated in proportion to HF severity
- Endothelin antagonists tested but NOT effective in HF (actually worsened outcomes in some trials)
Inflammatory Cytokines and Oxidative Stress
- TNF-α, IL-1β, IL-6: Directly depress myocardial function; induce myocyte apoptosis; contribute to cardiac cachexia
- Reactive oxygen species (ROS): Generated by xanthine oxidase, mitochondria, NADPH oxidase; cause protein oxidation, lipid peroxidation, DNA damage; impair myocyte function
- MMP (matrix metalloproteinases): Degrade ECM; contribute to LV dilatation
- Anti-cytokine therapy (e.g., etanercept, infliximab): NOT effective in HF trials
Novel Biological Targets
- ST2 (IL-1 receptor family): Decoy receptor for IL-33; elevated ST2 predicts adverse outcomes
- Galectin-3: Macrophage-derived; promotes fibrosis; elevated = poor prognosis
- GDF-15: Stress-responsive cytokine; marker of metabolic stress
- MicroRNAs: Gene regulatory molecules; potential therapeutic targets
- SGLT-2 pathway: Beyond glycemic control - reduces preload/afterload, improves cardiac metabolism, reduces oxidative stress, has direct cardiac effects
Dyssynchrony and Electrical Instability
-
Dyssynchrony: Abnormal activation sequence (esp. with LBBB, QRS >150ms) leads to:
- Paradoxical septal motion
- Reduced mechanical efficiency
- Secondary MR worsening
- Further adverse remodeling
- CRT reverses dyssynchrony and improves outcomes
-
Electrical Instability:
- Remodeled heart has heterogeneous refractoriness → substrate for re-entry
- HFrEF: 40-50% of deaths are sudden (VF/VT); risk highest in early disease
- ICD therapy reduces SCD
Secondary Mitral Regurgitation
- In dilated CMP: LV dilatation displaces papillary muscles laterally + tethers leaflets → incomplete coaptation
- Annular dilatation from LV dilatation further worsens MR
- Creates a vicious cycle: MR → more volume overload → more dilatation → worse MR
- Functional/secondary MR carries poor prognosis
- Guideline-directed therapy (GDMT) can reduce secondary MR; surgical repair in selected cases (MITRA-FR vs. COAPT trial controversy)
Cardiorenal and Abdominal Interactions
- Cardiorenal syndrome (CRS):
- Low forward CO → reduced renal perfusion → prerenal azotemia
- High venous pressure → elevated renal venous pressure → reduced filtration gradient → worsening renal function
- Neurohormonal activation (RAAS, SNS) → renal vasoconstriction
- Type 1 CRS: Acute worsening of HF causes acute kidney injury
- Type 2 CRS: Chronic HF causes progressive CKD
- Abdominal congestion: Elevated venous pressure → gut wall edema → impaired absorption → malnutrition
Gut Congestion, Microbiome, and Inflammation
- Gut congestion → increased intestinal permeability → translocation of bacterial products (lipopolysaccharide = LPS/endotoxin)
- Endotoxemia → systemic inflammation → worsening HF (cytokine storm)
- Gut microbiome alterations in HF:
- Reduced microbial diversity
- Overgrowth of pathogenic species
- Altered bile acid metabolism
- Trimethylamine N-oxide (TMAO): gut microbiome-derived metabolite; elevated in HF → platelet aggregation, atherosclerosis, worsening cardiorenal function
- Active area of investigation for microbiome-targeted therapies
High-Output States
- Characterized by elevated CO (>8 L/min) with reduced SVR despite normal or increased contractility
- The heart fails to keep up with elevated metabolic demand
- Causes:
- Severe anemia (Hgb <5 g/dL)
- AV fistulae (acquired or dialysis access)
- Thyrotoxicosis
- Paget's disease of bone (extensive)
- Wet beriberi (thiamine deficiency)
- Pregnancy/cirrhosis/obesity
- Characteristics: Wide pulse pressure, bounding pulses, warm extremities, normal or elevated EF
- Treatment: directed at underlying cause
III. EVALUATION
HISTORY
Symptoms of Congestion: Pulmonary vs. Systemic
| Pulmonary Congestion | Systemic Congestion |
|---|
| Dyspnea on exertion (most common/sensitive) | Peripheral edema (ankle, leg, sacral) |
| Orthopnea (dyspnea lying flat - elevated LVEDP) | Abdominal bloating/discomfort |
| Paroxysmal nocturnal dyspnea (PND) | RUQ pain (hepatic congestion) |
| Cough (nocturnal, dry or productive) | Nausea/early satiety (gut edema) |
| Acute pulmonary edema | Ascites |
| Cardiac asthma (wheeze from bronchial edema) | Weight gain (>2 kg/24-48h = alert) |
TABLE 264-4: NYHA FUNCTIONAL CLASSIFICATION (NYHAFC)
| Class | Description | Symptoms |
|---|
| I | No limitation of physical activity | Ordinary physical activity does NOT cause dyspnea, fatigue, or palpitations |
| II | Slight limitation | Comfortable at rest; ordinary activity causes symptoms |
| III | Marked limitation | Comfortable at rest; less-than-ordinary activity causes symptoms |
| IV | Symptoms at rest | Unable to carry on any physical activity without discomfort; symptoms at rest |
Note: NYHA class is dynamic and changes with treatment. Used to guide therapy decisions.
Symptoms of Reduced Perfusion (Low Output)
- Fatigue and exercise intolerance (most common)
- Mental confusion, difficulty concentrating
- Cold, clammy extremities
- Oliguria or nocturia (as renal perfusion shifts nocturnally when supine)
- Anorexia and early satiety
- Pre-syncope or syncope (advanced HF)
- Hemodynamic profile: "Cold and wet" (elevated filling pressures + low output) = worst prognosis
Other Symptoms
- Palpitations (arrhythmias: AF, PVCs, VT)
- Chest pain (may represent underlying CAD, or from RV stretch in acute decompensation)
- Depression and anxiety (common, underdiagnosed)
- Sleep disturbances: Cheyne-Stokes breathing, central sleep apnea, OSA
- Weight loss/cardiac cachexia (advanced HF - TNF-α-mediated)
Precipitating Factors
TABLE 264-5: PRECIPITATING FACTORS IN HEART FAILURE
| Category | Specific Factors |
|---|
| Non-compliance | Dietary sodium/fluid excess, medication non-adherence |
| Ischemic | ACS, MI, new ischemia/angina |
| Arrhythmia | New-onset AF/flutter, VT/VF, complete heart block, rapid ventricular rate |
| Hypertensive | Uncontrolled hypertension, hypertensive urgency/emergency |
| Infection | Pneumonia, sepsis, endocarditis, viral myocarditis, COVID-19 |
| Valvular | Worsening valvular disease, acute valve rupture (papillary muscle), endocarditis |
| Drug-related | NSAIDs, steroids, CCBs, negative inotropes; new cardiotoxic agents; drug/alcohol excess |
| Thyroid/Metabolic | Thyrotoxicosis/hypothyroidism, anemia, renal failure |
| Pulmonary | Pulmonary embolism, pneumonia, exacerbation of COPD |
| Other | Pregnancy, surgery/perioperative stress, anemia |
PHYSICAL EXAMINATION
General Appearance
- May appear comfortable at rest (compensated HF) or in obvious respiratory distress
- Cardiac cachexia: temporal wasting, temporal muscle loss (advanced HF, poor prognosis)
- Pallor, jaundice (hepatic congestion)
- Cyanosis: peripheral (reduced perfusion) or central (intracardiac shunt, severe pulmonary disease)
Vital Signs
- Heart Rate: On GDMT, resting HR ideally <70-75 bpm; tachycardia (>90 bpm) = poor prognosis
- Blood Pressure: May have hypotension with narrow pulse pressure in severe HF; hypertension suggests HFpEF or acute HF trigger
- Pulsus alternans: Alternating strong-weak pulse; incomplete LV recovery every alternate beat; indicates severe LV dysfunction
- Respiratory Rate: May increase with exertion or lying down; Cheyne-Stokes breathing in advanced HF
- O₂ saturation: Usually normal at rest; reduced with acute pulmonary edema, intracardiac shunting, pulmonary HTN, or concomitant lung disease
- Low-grade fever: May occur with severe HF (cytokine activation)
Jugular Venous Pulse (JVP)
- Method: 45° angle; JVP = height above sternal angle in cm + 5 cm H₂O
- Normal: ≤8 cm H₂O
- Hepatojugular reflux (HJR): Firm pressure over liver 15-30s + normal breathing → sustained JVP rise = elevated right-sided pressures
- Abdominojugular test: Rise in RA pressure during mid-abdominal compression + abrupt drop on release → elevated left-sided filling pressure
- Prominent V waves + Y descents = significant tricuspid regurgitation
- Kussmaul's sign: JVP rises with inspiration (instead of falling) - seen in severe biventricular HF, constrictive pericarditis, restrictive CMP; marker of poor outcome
Lung Examination
- Rales (crackles): Transudation into alveoli; bilateral basal; diffuse in severe HF/acute pulmonary edema
- Wheeze/Rhonchi: Bronchial mucosal congestion ("cardiac asthma") - may mimic COPD/asthma
- Absent rales: Despite elevated PCWP in chronic HF due to increased lymphatic drainage
- Pleural effusions: Dullness to percussion + decreased breath sounds at bases; usually bilateral (right > left when unilateral)
Cardiac Examination
- Apical impulse: Displaced laterally and inferiorly (dilated CMP); sustained/heaving (pressure overload)
- RV heave/parasternal lift: Biventricular or right HF
- S3 gallop: Volume overload + tachycardia; most commonly in HFrEF; hemodynamic compromise; negative prognostic significance
- S4 gallop: Reduced LV compliance (HFpEF, HTN); not specific to HF
- Murmurs: Holosystolic murmur of MR or TR (secondary to annular dilatation in HF); soft murmurs may indicate low-output state
- P2 loud: Pulmonary hypertension
Abdomen and Extremities
- Hepatomegaly: Tender, pulsatile (TR); painful with acute congestion
- Ascites: Advanced right/biventricular HF
- Splenomegaly: Chronic passive congestion
- Peripheral edema: Bilateral pitting; distribution follows gravity (ankles in ambulatory, sacrum in bedridden)
- Jaundice: Chronic hepatic congestion → cardiac cirrhosis (late)
IV. DIAGNOSIS
Routine Laboratories
- CBC: Anemia (high-output HF trigger; predicts poor prognosis); leukocytosis (infection trigger)
- Metabolic panel: Hyponatremia (poor prognosis - dilutional; RAAS/vasopressin activation); hyperkalemia or hypokalemia (RAAS therapy effects); BUN/creatinine (cardiorenal syndrome)
- LFTs: Transaminase/bilirubin elevation (passive hepatic congestion)
- TSH: Thyroid disease as cause or comorbidity
- Iron studies (Fe, TIBC, ferritin): Iron deficiency = major contributor to exercise intolerance; treatable comorbidity
- Uric acid: Elevated in HF; marker of poor prognosis
- Lipid panel: CAD evaluation
Chest X-Ray (CXR)
- Cardiomegaly: Cardiothoracic ratio >50% on PA film (not reliable in portable AP)
- Pulmonary venous hypertension: Upper zone vascular redistribution ("cephalization")
- Interstitial edema: Kerley B lines (horizontal lines in costophrenic angles = engorged lymphatics); peribronchial cuffing
- Alveolar edema: "Bat-wing" or "butterfly" pattern; perihilar haziness
- Pleural effusions: Blunting of costophrenic angles (right > left)
- Normal CXR does NOT exclude HF (especially HFpEF or early HF)
ECG
- LVH (pressure overload HTN/AS)
- LBBB (dyssynchrony, suggests dilated CMP, guides CRT)
- Q waves (ischemic CMP)
- AF/atrial arrhythmias
- Low voltage (amyloid, pericardial effusion)
- Prolonged QRS (CRT candidate)
- Low voltage with pseudoinfarct pattern = amyloidosis
Noninvasive Imaging
Echocardiography (FIRST LINE):
- Measures LVEF (classifies HFrEF/HFmrEF/HFpEF)
- LV dimensions, volumes, wall thickness, wall motion
- Diastolic function (tissue Doppler E/e' ratio, E/A, deceleration time)
- Valvular disease, pericardial effusion
- Estimated RVSP (pulmonary HTN)
- Strain imaging (GLS - global longitudinal strain) - detects subclinical dysfunction
CMR (Cardiac MRI):
- Gold standard for volumes/EF when echo is inadequate
- Tissue characterization: LGE identifies fibrosis/scar (ischemic vs. non-ischemic pattern)
- Edema detection (myocarditis)
- Amyloid, sarcoidosis, ARVC diagnosis
Nuclear Imaging:
- Radionuclide ventriculography (MUGA): accurate EF measurement
- Myocardial perfusion imaging (MPI): ischemia/viability assessment
CT Coronary Angiography:
- Rule out CAD as etiology (when echo/clinical data inconclusive)
Cardiopulmonary Exercise Testing (CPET)
- Peak VO₂ (<14 mL/kg/min = poor prognosis; threshold for transplant listing)
- VE/VCO₂ slope (>35 = poor prognosis)
- Used for transplant/LVAD evaluation
- Distinguishes cardiac from pulmonary etiology of dyspnea
Biomarkers
- BNP/NTproBNP: Released with wall stress; elevated in HF; useful for diagnosis, monitoring, prognosis
- BNP >100 pg/mL or NTproBNP >300 pg/mL supports HF diagnosis in dyspneic patients
- Used to guide decongestion therapy
- "BNP-guided therapy" trials (SIGNAL-HF, PRIMA, GUIDE-IT): inconclusive benefits in outpatient setting
- Troponin (cTnI/cTnT): Chronic low-level elevation in HF = ongoing myocyte injury; predicts poor prognosis
- ST2 (sST2): Elevated = cardiac fibrosis and remodeling; additive to BNP for risk stratification
- Galectin-3: Fibrosis marker; predicts adverse events
Invasive Studies
- Right heart catheterization (RHC):
- Measures RA, RV, PA pressures; PCWP (estimates LVEDP); CO by thermodilution/Fick
- Indicated when: diagnosis uncertain, pre-transplant/LVAD evaluation, pulmonary HTN workup, hemodynamic-guided management of refractory HF
- Hemodynamic profiles:
- "Warm and wet" (high PCWP, normal CO) = most common; diuresis
- "Cold and wet" (high PCWP, low CO) = advanced HF; inotropes + diuresis
- "Cold and dry" (normal PCWP, low CO) = volume depletion or advanced HF
- Left heart catheterization: Coronary angiography for ischemic workup; LV end-diastolic pressure
- Endomyocardial biopsy: Giant cell myocarditis, cardiac amyloidosis, drug toxicity - when specific diagnosis impacts management
V. COMORBIDITIES
Diabetes Mellitus
- Present in ~40% of HF patients
- Both HFrEF and HFpEF are more common in diabetics
- SGLT-2 inhibitors: cornerstone of both DM management and HF management (proven benefit in HFrEF and HFpEF regardless of DM status)
- GLP-1 agonists: reduce obesity, improve QOL; semaglutide shown to improve symptoms in HFpEF-obesity
- Avoid TZDs (pioglitazone) - cause fluid retention and worsen HF
Sleep Apnea
- Obstructive sleep apnea (OSA): ~40% of HF; contributes to HTN, pulmonary HTN, right heart dysfunction; CPAP effective
- Central sleep apnea/Cheyne-Stokes respiration: Driven by high loop gain and chronic hyperventilation; present in ~40% of advanced HFrEF
- Adaptive servo-ventilation (ASV) - CONTRAINDICATED in HFrEF with EF ≤45% and central sleep apnea - increased mortality (SERVE-HF trial)
Obesity
- Major risk factor for HFpEF; "obese HFpEF" is a distinct phenotype
- Pericardial constraint, increased ventricular interaction, elevated filling pressures
- GLP-1 agonists (semaglutide): reduced symptoms and improved QOL in STEP-HFpEF trial
- Paradox of obesity in HFrEF: higher BMI associated with better short-term outcomes ("obesity paradox") - may reflect cardiac reserve
Depression
- Prevalence ~30-40% in HF; independently predicts worse outcomes
- SSRIs: Do NOT improve survival (SADHART-CHF); neutral on mortality but may improve QOL
- Escitalopram shown to be neutral to negative in one trial
- Psychosocial support and collaborative care important
TABLE 264-8: DIFFERENTIAL DIAGNOSIS OF HEART FAILURE
| Condition | Distinguishing Features |
|---|
| Pulmonary disease (COPD, asthma) | Spirometry, DLCO; PFTs; response to bronchodilators; no elevated BNP |
| Pulmonary embolism | Acute onset; D-dimer; CT-PA; normal BNP possible |
| Pericardial effusion/tamponade | Echo; pulsus paradoxus; JVP elevated; no pulmonary rales |
| Constrictive pericarditis | Kussmaul's sign; pericardial knock; CT/CMR calcification; hemodynamic equalization |
| Restrictive cardiomyopathy | Amyloid/infiltrative pattern; low voltage; biatrial enlargement; CMR LGE |
| Nephrotic syndrome | Proteinuria; hypoalbuminemia; no elevated BNP/NTproBNP |
| Cirrhosis/Hepatic ascites | Liver disease history; normal BNP; hepatic stigmata; portal HTN |
| Hypoalbuminemia | Low albumin; causes dependent edema without elevated filling pressures |
| Venous insufficiency | Chronic stasis; no JVP elevation; normal BNP; unilateral or bilateral leg edema |
| Obesity hypoventilation | Elevated BMI; CO₂ retention; normal BNP; no cardiac structural abnormality |
| Bilateral pleural effusions (malignant) | No elevated JVP; cytology; CT |
| Thyroid disease | TSH; cardiac features reversible with treatment |
Differential Diagnosis - Clinical Approach
Key features favoring HF over mimics:
- Elevated BNP/NTproBNP + structural cardiac abnormality on echo
- Elevated JVP + pulmonary rales + S3 gallop
- Response to diuresis
- Symptoms in concordance with echocardiographic findings
CHAPTER 265: HEART FAILURE MANAGEMENT
I. HFpEF AND HFmrEF MANAGEMENT
General Principles
- Treat underlying causes and precipitants
- Aggressive control of comorbidities (HTN, AF, DM, obesity, sleep apnea, ischemia)
- Decongestion with diuretics (symptom relief)
- Avoid excessive preload reduction (risk of underfilling → azotemia, hypotension, syncope)
Clinical Trials in HFpEF
| Trial | Intervention | Result |
|---|
| TOPCAT | Spironolactone vs. placebo | Primary endpoint negative; post-hoc: benefit in Americas subgroup |
| CHARM-Preserved | Candesartan vs. placebo | Non-significant trend; some reduction in HF hospitalizations |
| I-PRESERVE | Irbesartan vs. placebo | Negative |
| PEP-CHF | Perindopril vs. placebo | Negative primary endpoint |
| PARAGON-HF | Sacubitril-valsartan vs. valsartan | Primary endpoint p=0.06 (marginally missed); benefit in women and those with lower EF; FDA approved across full EF spectrum |
| PARAGLIDE-HF | Sacubitril-valsartan vs. valsartan | Reduced NTproBNP at 8 weeks; benefit confined to EF ≤60% |
| EMPEROR-Preserved | Empagliflozin vs. placebo | POSITIVE - significant reduction in CV death/HF hospitalizations |
| DELIVER | Dapagliflozin vs. placebo | POSITIVE - significant reduction in worsening HF/CV death |
| STEP-HFpEF | Semaglutide vs. placebo | Improved symptoms, QOL, and 6MWT in obese HFpEF |
SGLT-2 inhibitors (dapagliflozin, empagliflozin): First class of drugs with proven benefit in HFpEF - now Class I recommendation.
Other Therapeutic Agents in HFpEF
- Diuretics: Symptom relief; no mortality benefit demonstrated
- ACEIs/ARBs: Not proven effective (except prevention); guideline-directed for HTN management
- Spironolactone/MRA: May be beneficial; used especially when EF 45-55%
- Sacubitril-valsartan: Approved across full EF spectrum; greatest benefit EF below normal
- Beta-blockers: Useful for rate control in AF; not proven beneficial in pure HFpEF sinus rhythm
- GLP-1 agonists (semaglutide): Improve QOL irrespective of DM status in obese HFpEF
- Avoid: ASV (increased mortality), TZDs (fluid retention), calcium channel blockers (limited role)
FIGURE 265-1: HFpEF - Pathophysiology, Therapeutic Principles and Directed Therapy
Key elements (from Harrison's Figure 265-1):
PATHOLOGY: Hypertrophy, Fibrosis/altered collagen, Infarction/ischemia
RISK MARKERS: Hypertension, Aging, Atherosclerosis, Diabetes, Obesity
General Therapeutic Principles:
- Reduce the congestive state - Caution: don't reduce preload excessively; implantable hemodynamic monitors useful
- Control blood pressure - Central aortic BP control may be more relevant
- Maintain atrial contraction and prevent tachycardia - AF ablation may reduce morbidity/mortality
- Treat and prevent myocardial ischemia - May mimic HF as angina equivalent
- Detect and treat sleep apnea - Common comorbidity; ASV INEFFECTIVE/harmful
- Lifestyle modification - Diet + exercise for weight reduction and functional capacity
Specific Therapy Targets:
- RAAS: ACEIs/ARBs ineffective (except prevention); aldosterone antagonists may be beneficial
- Digoxin: Ineffective (may reduce hospitalizations)
- Beta blockers/CCBs: Ineffective (useful for tachycardia prevention in AF)
- PDE-5 inhibitors: Sildenafil ineffective
- Novel: ARNi (may be effective); SGLT-2i (reduce HF hospitalization) - PROVEN
- Chronotropic insufficiency: Targeted pacing - likely ineffective
- Obesity: GLP-1 agonists (improve QOL irrespective of DM)
Clinical Guiding Principles (HFpEF)
- Precise diagnosis essential - HFpEF is a heterogeneous group; infiltrative, storage, pericardial, valvular disease may require entirely different management
- Aggressive BP control to guideline targets
- Diuretics for volume overload
- Evaluate for ischemia if coronary risk present
- AF: aggressive rate control, anticoagulation, early rhythm restoration
- Comorbidities (obesity, OSA, CKD, anemia/iron deficiency) = important treatment targets
- Avoid excessive preload reduction
II. ACUTE DECOMPENSATED HEART FAILURE (ADHF)
General Principles
- ADHF is a heterogeneous clinical syndrome resulting from decreased cardiac performance + renal dysfunction + vascular compliance alterations
- Admission with ADHF = excessive morbidity/mortality; ~50% readmission within 6 months
- Primary goal: Rapid decongestion while maintaining organ perfusion
- Hemodynamic profiling essential:
- "Warm and wet" = most common; diuresis
- "Cold and wet" = inotropes + diuresis
- "Cold and dry" = volume challenge or advanced HF/cardiogenic shock
Volume Management - IV Diuretics
First-line therapy for ADHF with congestion:
| Drug | Class | Starting Dose | Notes |
|---|
| Furosemide | Loop diuretic | 40-200 mg IV | Standard first-line; double outpatient oral dose IV at minimum |
| Bumetanide | Loop diuretic | 0.5-2 mg IV | More bioavailable than furosemide |
| Torsemide | Loop diuretic | 10-100 mg IV/PO | Better oral bioavailability; may be preferred in outpatient transition |
| Ethacrynic acid | Loop diuretic | 25-100 mg IV | Use if sulfonamide allergy |
DOSE Trial findings: High-dose diuretic strategy (2.5x oral dose) → greater diuresis and more rapid symptom relief, at cost of transient worsening of renal function; no difference in 60-day outcomes. Bolus vs. continuous infusion: No significant difference; bolus may be preferred operationally.
Goal of diuresis: Net negative fluid balance 1-2 L/day; urine Na >70 mEq/L suggests adequate response; daily weights; avoid excessive diuresis (watch BUN/creatinine)
Diuretic resistance:
- Mechanisms: Poor gut absorption (IV route needed), aldosterone breakthrough, neurohormonal activation, renal hypoperfusion
- Management: IV loop diuretics + metolazone (thiazide) combination (synergistic); ultrafiltration
Cardiorenal Syndrome in ADHF
- Worsening renal function (WRF) during ADHF hospitalization = common and complex
- May NOT worsen outcomes if decongestion is achieved (CARRESS-HF data)
- Permissive approach to creatinine rise (if decongestion is ongoing) is often appropriate
- Persistent WRF with inadequate decongestion = poor prognosis
Ultrafiltration
- Mechanical removal of isotonic plasma water using semipermeable membrane
- CARRESS-HF trial: Ultrafiltration was NOT superior to pharmacologic diuresis; associated with more adverse events including worsening renal function
- Reserved for: true diuretic resistance, intractable volume overload, hypervolemic hyponatremia
Vasoactive Therapy
Vasodilators (for "warm and wet" or hypertensive ADHF):
TABLE 265-1: VASOACTIVE THERAPY IN ADHF
| Drug | Class | Mechanism | Dose | Hemodynamic Effects | Notes |
|---|
| Nitroglycerin (NTG) | Organic nitrate | NO donor; venodilation (low dose) + arteriodilation (high dose) | 10-200 mcg/min IV | ↓ preload >> afterload; ↓ PCWP, ↓ RA | First-line vasodilator; tachyphylaxis within 24h; avoid in RV infarction |
| Sodium Nitroprusside | Inorganic nitrate | NO donor; balanced arteriolar + venous dilation | 0.1-5 mcg/kg/min IV | ↓↓ SVR, ↓ PCWP | Hypertensive urgency + HF; cyanide toxicity (renal insufficiency); requires ICU monitoring |
| Nesiritide (BNP) | Natriuretic peptide | Stimulates cGMP; vasodilation, natriuresis | 2 mcg/kg bolus → 0.01 mcg/kg/min | ↓ PCWP, ↓ SVR; mild ↑ CO | ASCEND-HF: No mortality benefit; renal concerns; limited current use |
| Hydralazine | Direct vasodilator | Arteriolar dilation via unclear mechanism | 10-75 mg q6-8h PO | ↓ SVR, ↓ afterload | Used in combo with isosorbide dinitrate (BiDil for African Americans) |
| Isosorbide dinitrate | Organic nitrate | Venodilation | 20-160 mg/day PO | ↓ Preload | Combination with hydralazine |
| Clevidipine | Short-acting CCB | L-type Ca channel blockade | 1-16 mg/h IV | Rapid BP lowering; minimal HR effect | Hypertensive ADHF |
| Fenoldopam | DA-1 agonist | Renal + systemic vasodilation | 0.1-0.3 mcg/kg/min | ↓ BP; ↑ renal blood flow | Hypertensive ADHF + renal dysfunction |
Inotropic Therapy:
| Drug | Class | Mechanism | Dose | Notes |
|---|
| Dobutamine | Beta-1 agonist | ↑ cAMP; ↑ contractility, ↑ HR | 2-20 mcg/kg/min IV | First-line inotrope; tachycardia; arrhythmogenic; tolerance develops |
| Milrinone | PDE-3 inhibitor | ↑ cAMP; inodilatation (inotrope + vasodilator) | 0.125-0.75 mcg/kg/min IV | Preferred in beta-blocked patients; hypotension; arrhythmias; OPTIME-CHF: worse in ischemic HF |
| Dopamine | Dopaminergic/adrenergic | Dose-dependent: D1 (renal) → β1 (inotrope) → α1 (vasoconstriction) | 2-20 mcg/kg/min | Low-dose ("renal dose") dopamine unproven for renal protection; not first-line inotrope |
| Levosimendan | Ca sensitizer + K-ATP channel opener | ↑ myofilament Ca sensitivity; vasodilation | 12 mcg/kg bolus → 0.1 mcg/kg/min | Approved in EU; NOT approved in US; neutral/positive results in some trials |
| Norepinephrine | Alpha + beta agonist | Vasoconstriction + inotropy | 0.1-1 mcg/kg/min | For cardiogenic shock with hypotension; combination with inotrope |
Other ADHF Therapies:
- Oxygen: Maintain SpO₂ >94%; high-flow nasal cannula for moderate hypoxia
- Non-invasive ventilation (NIV) - CPAP/BiPAP: Beneficial for cardiogenic pulmonary edema (reduces intubation rate, improves dyspnea)
- Mechanical ventilation: For refractory respiratory failure
- Morphine: Historical use; recent ADHF data (OPIATES trial) showed increased ICU transfer, mechanical ventilation, mortality - CAUTION/avoid
- Mechanical circulatory support (IABP, Impella, ECMO): For cardiogenic shock
ADHF Clinical Guiding Principles:
- Rapidly identify and treat precipitating cause
- Hemodynamic profiling to guide therapy
- Decongestion is the primary goal
- Transition to oral GDMT before discharge
- Intensive early postdischarge follow-up (STRONG-HF: 2-week intensive titration → reduced 180-day readmissions)
- Avoid morphine
- Correct electrolyte abnormalities
III. HFrEF MANAGEMENT
TABLE 265-2: GUIDELINE-DIRECTED PHARMACOLOGIC THERAPY (GDMT) AND TARGET DOSES IN HFrEF
| Drug | Starting Dose | Target/Maximum Dose | Key Trial | Outcome |
|---|
| ACE INHIBITORS | | | | |
| Captopril | 6.25 mg TID | 50 mg TID | SAVE, SOLVD | ↓ Mortality 17-23% |
| Enalapril | 2.5 mg BID | 10-20 mg BID | CONSENSUS, SOLVD | ↓ Mortality 16-40% |
| Lisinopril | 2.5-5 mg OD | 20-40 mg OD | ATLAS | ↓ Mortality/hospitalizations |
| Ramipril | 1.25-2.5 mg OD | 10 mg OD | AIRE, HOPE | Post-MI benefit |
| ARBs (if ACEI-intolerant) | | | | |
| Candesartan | 4-8 mg OD | 32 mg OD | CHARM | Non-inferior to ACEI |
| Valsartan | 40 mg BID | 160 mg BID | Val-HeFT | ↓ Hospitalization |
| ARNi (REPLACE ACEI/ARB) | | | | |
| Sacubitril-Valsartan | 24/26 mg BID | 97/103 mg BID | PARADIGM-HF | ↓ CV death/HF hosp 20% vs. enalapril |
| BETA-BLOCKERS | | | | |
| Carvedilol | 3.125 mg BID | 25 mg BID (50 mg if >85 kg) | COPERNICUS, CAPRICORN | ↓ Mortality 35% |
| Metoprolol succinate (XL) | 12.5-25 mg OD | 200 mg OD | MERIT-HF | ↓ Mortality 34% |
| Bisoprolol | 1.25 mg OD | 10 mg OD | CIBIS-II | ↓ Mortality 34% |
| MRA | | | | |
| Spironolactone | 12.5-25 mg OD | 25-50 mg OD | RALES | ↓ Mortality 30% (Class III-IV) |
| Eplerenone | 25 mg OD | 50 mg OD | EPHESUS, EMPHASIS-HF | ↓ Mortality post-MI and Class II |
| SGLT-2 INHIBITORS | | | | |
| Dapagliflozin | 10 mg OD | 10 mg OD | DAPA-HF | ↓ CV death/worsening HF 26% |
| Empagliflozin | 10 mg OD | 10 mg OD | EMPEROR-Reduced | ↓ CV death/HF hosp 25% |
| SPECIAL POPULATIONS | | | | |
| Hydralazine + Isosorbide (BiDil) | H 25 mg + I 20 mg TID | H 75 mg + I 40 mg TID | V-HeFT I/II, A-HeFT | ↓ Mortality in African Americans; alternative if ACEI/ARNi intolerant |
| HEART RATE MODIFICATION | | | | |
| Ivabradine | 5 mg BID | 7.5 mg BID | SHIFT | ↓ HF hospitalization (EF ≤35%, HR ≥70, on max BB, sinus rhythm) |
NEUROHORMONAL ANTAGONISM (HFrEF)
Class Effect and Sequence of Administration:
- ACEIs/ARBs: Class effect; any can be used; titrate to evidence-based doses
- Beta-blockers: NOT a class effect - only carvedilol, bisoprolol, and metoprolol succinate proven to improve survival; agents with ISA (xamoterol, bucindolol) ineffective or harmful
- CIBIS III trial: Order of initiation (ACEI vs. BB first) does not affect outcome; what matters is achieving optimal doses of both
- Dose and outcome are correlated: Aggressive titration to target doses improves outcomes
RAAS Therapy and Neurohormonal Escape:
- Aldosterone levels may "escape" ACE inhibitor therapy over time (via non-ACE pathways: chymase, kallikrein)
- Rationale for adding MRA (spironolactone/eplerenone) on top of ACEI/ARB
- RAAS triple therapy (ACEI + ARB + MRA): AVOID - increased adverse events (hyperkalemia, renal impairment) without additional benefit (ONTARGET)
- ARNi (Sacubitril-Valsartan) has REPLACED ACEI/ARB as preferred neurohormonal agent:
- PARADIGM-HF: Sacubitril-valsartan reduced CV death/HF hospitalization by 20% vs. enalapril
- Requires wash-out period of 36 hours when switching from ACEI (angioedema risk)
- Neprilysin inhibition → ↑ BNP (can no longer use BNP for monitoring; use NTproBNP instead)
Mineralocorticoid Receptor Antagonists (MRA)
- Spironolactone (RALES trial): NYHA III-IV on ACEI + furosemide; 30% reduction in mortality
- Eplerenone (EMPHASIS-HF): NYHA II, EF ≤35%; significant mortality reduction
- Key safety: Monitor K+ and renal function (risk of hyperkalemia); avoid if K+ >5.0 mEq/L or eGFR <30
Alternative Vasodilators
- Hydralazine + Isosorbide dinitrate (H-ISDN):
- Alternative for patients who cannot tolerate ACEI/ARB (renal insufficiency, bilateral RAS, angioedema)
- A-HeFT trial: Significant mortality benefit specifically in African Americans - BiDil (fixed-dose combination) approved for this indication
- Mechanism: Hydralazine (arteriodilation) + ISDN (venodilation) + hydralazine antioxidant effect (prevents nitrate tolerance)
Novel Neurohormonal Antagonists
Sacubitril-Valsartan (ARNi): (see above)
Vericiguat (sGC stimulator):
- Stimulates soluble guanylyl cyclase (sGC) → ↑ cGMP → vasodilation; independent of NO availability
- VICTORIA trial: Significant reduction in HF hospitalization and CV death in high-risk HFrEF (after worsening HF event); absolute benefit modest
- Dose: 2.5 mg → 10 mg once daily
- Added to GDMT for high-risk patients
HEART RATE MODIFICATION
Ivabradine:
- Selective If channel blocker (funny current in SA node) → ↓ HR without negative inotropy
- SHIFT trial: EF ≤35%, sinus rhythm, HR ≥70 bpm, on maximally tolerated beta-blocker
- Significant reduction in HF hospitalization (not mortality)
- Indication: LVEF ≤35%, sinus rhythm, HR ≥70 bpm despite maximally tolerated beta-blocker
SGLT-2 INHIBITION
- Originally developed for diabetes; demonstrated striking CV benefits independent of glycemic effects
- Mechanisms in HF:
- Osmotic diuresis/natriuresis (reduce preload)
- Reduced sympathetic tone
- Improved cardiac metabolism (ketone utilization)
- Reduced oxidative stress and inflammation
- Direct cardiac effects (anti-hypertrophic, anti-fibrotic)
- Erythropoietic effects (increase EPO)
- DAPA-HF (dapagliflozin): 26% reduction in CV death/worsening HF in HFrEF (with AND without DM)
- EMPEROR-Reduced (empagliflozin): 25% reduction in CV death/HF hospitalization in HFrEF
- EMPEROR-Preserved + DELIVER: Proven benefit in HFpEF/HFmrEF
- Dose: Fixed: Dapagliflozin 10 mg OD, Empagliflozin 10 mg OD
SOLUBLE GUANYLYL CYCLASE (sGC) STIMULATION
Vericiguat: (see above)
- Mechanism: sGC stimulator → ↑ cGMP → vasodilation + cardiac effects
- Works independently of NO availability (advantage in HF where NO signaling is impaired)
- VICTORIA trial: modest but significant benefit in very high-risk HFrEF
MYOSIN ACTIVATION (Novel Agent)
Omecamtiv Mecarbil:
- Selective cardiac myosin activator → prolongs systolic ejection time → ↑ stroke volume without ↑ intracellular calcium
- GALACTIC-HF trial: Modest reduction in HF events (significant primary endpoint); no significant mortality reduction; largest benefit in those with lowest LVEF (≤28%)
- Not yet approved; represents a new class targeting contractile apparatus rather than neurohormonal system
DIGOXIN
- Oldest cardiac drug; inhibits Na+/K+ ATPase → increases intracellular Ca → modest positive inotropy; also reduces sympathetic tone and slows AV conduction
- DIG trial: No mortality benefit; significant reduction in HF hospitalizations
- Current role:
- Rate control in HFrEF + AF (adjunct to beta-blockers)
- Selected symptomatic patients with HFrEF despite GDMT
- NARROW THERAPEUTIC WINDOW: Target digoxin level 0.5-0.9 ng/mL (higher levels = increased mortality)
- Caution: renal failure, hypokalemia, hypomagnesemia, drug interactions (amiodarone, clarithromycin, verapamil)
- NOTE: Ineffective in HFpEF
ORAL DIURETICS
- Furosemide: 20-160 mg OD-BID PO; variable bioavailability (10-100%); consider switching to torsemide
- Torsemide: Superior oral bioavailability; may reduce HF hospitalizations vs. furosemide (TRANSFORM-HF: similar overall, but torsemide better tolerated)
- Metolazone: Added for diuretic resistance; 2.5-5 mg before loop diuretic; monitor electrolytes carefully
- Spironolactone/Eplerenone: Dual function (MRA + diuretic); especially useful with electrolyte-sparing effect
- Goal: Euvolemia; daily weight monitoring; adjust dose based on renal function and electrolytes
CALCIUM CHANNEL ANTAGONISTS
- Non-dihydropyridines (verapamil, diltiazem): CONTRAINDICATED in HFrEF - negative inotropy worsens outcomes
- Amlodipine/Felodipine: Safe in HFrEF; no mortality benefit but no harm (PRAISE-1/2); used for hypertension or angina in HFrEF
- In HFpEF: CCBs may be used for rate control in AF or HTN management
ANTI-INFLAMMATORY THERAPY
- IL-1 blockade (Anakinra): Small RCTs show improvement in functional capacity and inflammatory markers; larger trials needed
- Colchicine: COPE trial (post-pericardiotomy); data in HF limited
- TNF-α antagonists: Infliximab, etanercept - TESTED AND FAILED in HF trials (ATTACH, RENEWAL); harm in higher doses - AVOID/CONTRAINDICATED in HFrEF
- Pentraxin: No proven benefit
- SGLT-2i indirectly anti-inflammatory: Partly explains benefits
HMG-CoA REDUCTASE INHIBITORS (STATINS)
- Theoretically beneficial (anti-inflammatory, anti-fibrotic, pleiotropic effects)
- CORONA and GISSI-HF trials: Rosuvastatin vs. placebo in HFrEF → NO mortality benefit
- Current recommendation:
- Initiate statins if underlying CAD or other CV indications (primary indication remains lipid lowering/cardiovascular event prevention)
- Do NOT start statins solely for HF treatment
- If already on statins, continue (do not discontinue)
ANTICOAGULATION AND ANTIPLATELET THERAPY
- AF + HF: Oral anticoagulation (OAC) is indicated - NOACs preferred over warfarin (ARISTOTLE, ROCKET-AF data)
- HFrEF in sinus rhythm: NO routine anticoagulation; WARCEF trial: warfarin vs. aspirin - net effect neutral; ↑ bleeding, modest stroke reduction
- Low-dose rivaroxaban (COMMANDER-HF): No benefit in HFrEF sinus rhythm with CAD
- Aspirin: If concurrent CAD/prior MI; not routinely for HF alone
- Heparin (DVT prophylaxis): LMWH during hospitalization for immobile patients
FISH OIL (N-3 PUFA)
- GISSI-HF trial: Omega-3 (1 g/day) in HFrEF → modest but significant reduction in mortality and HF hospitalizations (NNT ~56 over 4 years)
- Mechanism: Anti-arrhythmic, anti-inflammatory, membrane stabilizing
- Considered "potentially effective" (see Fig 265-3)
- Recommended: 1 g OD omega-3 PUFA in symptomatic HFrEF (Class IIb recommendation)
MICRONUTRIENTS
- Iron deficiency (without anemia): Common in HF; impairs exercise tolerance and quality of life
- IV iron (ferric carboxymaltose - AFFIRM-AHF, CONFIRM-HF): Reduces HF hospitalizations; improves symptoms and functional capacity; AFFIRM-AHF: IV FCM reduced HF hospitalization by 26% after ADHF
- Oral iron: Poorly absorbed in HF; generally less effective
- Thiamine: Deficiency possible in elderly HF patients on furosemide; supplementation reasonable
- Magnesium: Deplete with diuresis; supplement to prevent arrhythmias
- Zinc: Deficiency in cardiac cachexia; supplementation not proven
ENHANCED EXTERNAL COUNTERPULSATION (EECP)
- Pneumatic compression of lower limbs during diastole → augments diastolic pressure and coronary perfusion
- MUST study: limited benefit in HFrEF
- Current role: Adjunct for refractory angina in patients not candidates for revascularization; limited HF use
EXERCISE
- HF-ACTION trial: Aerobic exercise training (supervised + home-based) → modest but significant improvement in all-cause mortality/hospitalization; improved QOL and functional capacity
- Recommendation: Moderate-intensity aerobic exercise (e.g., walking 30 min, 5 days/week) in stable HFrEF is safe and beneficial
- Cardiac rehabilitation programs recommended
- Resistance training: Safe in stable HFrEF; improves muscle strength and functional capacity
MANAGEMENT OF SELECTED COMORBIDITIES
| Comorbidity | Management Strategy |
|---|
| AF | Rate control (beta-blocker + digoxin); rhythm control (amiodarone, catheter ablation); OAC mandatory |
| Hypertension | ARNi/ACEI/ARB + MRA + beta-blocker (GDMT serves dual purpose) |
| Diabetes | SGLT-2i first-line (HF benefit); GLP-1 agonists (weight/QOL in HFpEF); avoid TZDs |
| CKD | GDMT with dose adjustment; SGLT-2i safe to eGFR 20-25; RHC before renal transplant |
| Iron deficiency | IV iron (ferric carboxymaltose); recheck ferritin/TSAT every 3-6 months |
| OSA | CPAP |
| Central sleep apnea | Oxygen; ASV CONTRAINDICATED in HFrEF EF ≤45% |
| Depression | SSRIs (neutral outcome; may improve QOL); psychotherapy; collaborative care |
| Anemia | Treat iron deficiency; ESAs NOT beneficial in HF |
| Gout | Allopurinol safe; colchicine for acute gout; avoid NSAIDs |
| COPD | Continue beta-blockers (cardioselective preferred); address modifiable risk |
IV. DEVICE THERAPY (NEUROMODULATION)
Cardiac Contractility Modulation (CCM)
- Delivers non-excitatory electrical signals during absolute refractory period → ↑ contractility without initiating AP
- FIX-HF-5 trial: Improved VO₂ and QOL in NYHA III, EF 25-45%, QRS <130 ms (i.e., NOT CRT candidate)
- Approved in US as adjunct to GDMT for HFrEF in non-CRT candidates
Cardiac Resynchronization Therapy (CRT)
Mechanism: Simultaneous biventricular pacing corrects electrical dyssynchrony → improved mechanical efficiency → reverse remodeling
Indications (Class I):
- LVEF ≤35%
- LBBB with QRS ≥150 ms
- NYHA Class II-III-IV (ambulatory) on GDMT
- Sinus rhythm
MADIT-CRT, RAFT, REVERSE trials: CRT reduces HF hospitalizations, mortality, and achieves reverse remodeling (↑ EF, ↓ LV dimensions)
CRT-D (with defibrillator) vs. CRT-P (pacemaker only):
- CRT-D preferred in most patients with reasonable survival expectancy and no significant comorbidities
- CRT-P in older patients, significant comorbidity, shorter expected benefit
Response rates: ~70% show clinical improvement; ~15-20% are "non-responders"
Predictors of CRT response: LBBB morphology, female sex, non-ischemic etiology, QRS >150ms, less RV dysfunction
Sudden Cardiac Death Prevention in HF
Risk factors for SCD in HF:
- LVEF ≤35% (strongest predictor)
- Prior VT/VF
- NYHA Class II-III (paradoxically higher risk than NYHA IV)
- NSVT on Holter
ICD Therapy:
| Setting | Trial | Indication | Benefit |
|---|
| Secondary prevention | All SCD trials | Prior VT/VF arrest | ↓ Mortality vs. amiodarone |
| Primary prevention - Non-ischemic | SCD-HeFT, MADIT-CRT | LVEF ≤35%, NYHA II-III on GDMT ≥3 months | ↓ Mortality 23-31% |
| Primary prevention - Ischemic | MADIT-II, MUSTT | LVEF ≤30-35%, prior MI ≥40 days | ↓ Mortality 31% |
Key caveats:
- Wait ≥3 months of GDMT before reassessing EF for ICD/CRT eligibility (EF may recover)
- Wait ≥40 days post-MI before ICD implant
- Wearable ICD (LifeVest): Bridge to ICD in newly diagnosed HFrEF awaiting GDMT response assessment
V. SURGICAL THERAPY IN HF
| Intervention | Indication | Evidence |
|---|
| CABG | Ischemic HFrEF with viable myocardium | STICH trial: CABG + GDMT → ↓ long-term mortality vs. GDMT alone |
| Surgical ventricular restoration (SVR) | LV aneurysm post-MI | STICH: SVR added to CABG → no additional benefit |
| Mitral valve repair/replacement | Severe functional MR, NYHA III-IV, EF >30% | COAPT: MitraClip → ↓ mortality and HF hospitalizations in severe functional MR |
| TAVI/SAVR | Severe AS-related HF | Standard of care; TAVI for high/intermediate-risk |
| Heart transplantation | End-stage HF, peak VO₂ <12-14 mL/kg/min, refractory to GDMT | 1-year survival >90%; median survival >12 years; gold standard for end-stage HF |
| LVAD (Destination therapy) | Ineligible for transplant; bridge to transplant | REMATCH: DT-LVAD → ↓ mortality vs. medical therapy in end-stage HF |
| Total artificial heart | Biventricular failure; bridge to transplant only | CardioWest TAH; highly specialized centers |
VI. CELLULAR AND GENE-BASED THERAPY
- Bone marrow/cardiac-derived stem cells: Multiple trials; inconsistent results; not currently clinically established
- c-kit+ cells: Small pilot trials showed LV function improvement; not confirmed in larger studies
- Mesenchymal stem cells (DREAM-HF): Randomized trial - NEGATIVE primary and secondary endpoints
- SERCA2a gene therapy (CUPID trial): Initially promising; confirmatory trial failed primary endpoint
- Current status: Investigational; no approved cellular or gene therapy for HF as of 2025
- LVAD recovery strategy: Efforts to use MSCs for weaning from LVAD have been disappointing
VII. DISEASE MANAGEMENT AND SUPPORTIVE CARE
- Despite excellent pharmacotherapy, ~50% readmitted within 6 months of discharge
- Recurrent HF = only half of readmissions; non-cardiac comorbidities drive the rest
- STRONG-HF trial: Intensive titration of GDMT within 2 weeks + frequent ambulatory follow-up through 2 months → significant reduction in all-cause mortality and HF readmission at 180 days
- Telemonitoring of weight/vital signs: NOT shown to decrease hospitalizations in RCTs
- Intrathoracic impedance monitoring (OptiVol): Not proven; high false-positive rate → may paradoxically increase hospitalizations
- CardioMEMS (implantable PA pressure sensor - CHAMPION trial): PA pressure-guided management → significant reduction in HF hospitalization; approved in US for NYHA III HF with prior HF hospitalization
Key discharge elements:
- Comprehensive discharge planning + patient/caregiver education
- Appropriate visiting nurse involvement
- Optimized oral GDMT before discharge
- Follow-up within 7-14 days of discharge (STRONG-HF protocol)
- Daily weight monitoring; action plan for weight gain >2 kg
Supportive/Palliative Care:
- Advance directives and goals-of-care discussions in advanced HF
- Symptom management: opioids for dyspnea (low-dose), diuretics
- Multidisciplinary HF team (cardiologist, HF nurse, pharmacist, social work, palliative care)
- Hospice referral for NYHA IV refractory to all therapy
QUICK-REFERENCE FLOWCHARTS
FLOWCHART 1: HF DIAGNOSIS
Symptoms (dyspnea, edema, fatigue) + Signs (elevated JVP, rales, S3)
↓
Measure BNP/NTproBNP
┌────────────────────────────────────┐
BNP <100 pg/mL BNP ≥100 pg/mL
(HF unlikely) (HF possible)
↓
Echocardiography
┌──────────────────────────────────┐
Structural cardiac abnormality?
YES NO
↓ ↓
Classify EF: Consider alternative dx
EF ≤40% → HFrEF (pulmonary, renal, etc.)
EF 41-49% → HFmrEF
EF ≥50% → HFpEF
↓
Search for cause (Table 264-2)
Identify precipitants (Table 264-5)
Assess severity (NYHA class - Table 264-4)
FLOWCHART 2: ADHF MANAGEMENT
ADHF Presentation
↓
Hemodynamic Profiling
┌──────────────────────────────────────┐
"Warm & Wet" "Cold & Wet" "Cold & Dry"
(Most Common) (Low output + HF) (Advanced/Volume depleted)
↓ ↓ ↓
IV Diuretics Inotropes + Careful volume
(loop diuretic) IV Diuretics challenge or
+ Vasodilators (Dobutamine/ MCS/evaluation
(if BP ≥90) Milrinone) for advanced HF
↓
Assess response at 6-12 hours:
- Urine output >100 mL/h? ✓
- Dyspnea improving? ✓
- Weight decreasing? ✓
↓
If inadequate: Add metolazone or consider ultrafiltration
↓
Euvolemia achieved → Transition to oral GDMT
↓
Before Discharge:
- Start/optimize ARNi/ACEI + BB + MRA + SGLT-2i
- Patient education
- Follow-up within 7-14 days
FLOWCHART 3: HFrEF GDMT INITIATION (THE "FANTASTIC FOUR")
New HFrEF Diagnosis (EF ≤40%)
↓
Start ALL FOUR simultaneously or sequentially:
┌─────────────────────────────────────────────────────┐
│ 1. ARNi (sacubitril-valsartan) - preferred over │
│ ACEI/ARB; if intolerant → ACEI or ARB or H-ISDN │
│ 2. Beta-blocker (carvedilol/metoprolol/bisoprolol) │
│ 3. MRA (spironolactone/eplerenone) │
│ 4. SGLT-2i (dapagliflozin/empagliflozin) │
└─────────────────────────────────────────────────────┘
↓
Reassess in 3 months:
EF still ≤35% AND NYHA II-III AND HR ≥70?
↓ Yes
Consider ivabradine (SHIFT trial)
↓
EF still ≤35% on GDMT ≥3 months, LBBB QRS ≥150ms?
↓ Yes
CRT-D implant
↓
EF ≤35%, NYHA II-III, not CRT candidate?
↓ Yes
ICD (primary prevention) or
CCM (if QRS <130ms, EF 25-45%)
↓
Refractory/NYHA IV despite GDMT + device therapy?
↓ Yes
LVAD (bridge to transplant or destination therapy)
→ Cardiac transplantation if eligible
FLOWCHART 4: SCD PREVENTION IN HFrEF
HFrEF (EF ≤35%)
↓
Optimize GDMT ≥3 months
↓
Reassess LVEF
EF ≤35%?
↓ YES
NYHA II-III (ambulatory)?
↓ YES
Prior VT/VF? → ICD (Secondary prevention - Class I)
No prior VT/VF → ICD Primary prevention (SCD-HeFT/MADIT-II)
↓
LBBB + QRS ≥150ms? → CRT-D (preferred over ICD alone)
↓
Expected meaningful survival >1 year?
↓ YES
ICD or CRT-D implant
KEY SUMMARY TABLE: 4 PILLARS OF HFrEF THERAPY
| Drug Class | Drug | Mortality Reduction | Key Safety |
|---|
| ARNi/ACEI | Sacubitril-valsartan | ~20% vs. enalapril | Watch K+, renal function, BP; 36h washout from ACEI |
| Beta-blocker | Carvedilol/Metoprolol/Bisoprolol | ~34-35% | Start low, go slow; not for acute decompensation |
| MRA | Spironolactone/Eplerenone | ~15-30% | Monitor K+, eGFR; avoid if K+ >5 or eGFR <30 |
| SGLT-2i | Dapagliflozin/Empagliflozin | ~25% composite | UTI/genital infections; do not use if eGFR <20 |
Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Chapters 264 & 265
Authors: Michael M. Givertz, Mandeep R. Mehra