Epidermolysis bullosa complete detail
Reading File
Finding Sources
Searching PubMed
"epidermolysis bullosa"[MeSH Terms]
Searching Images
epidermolysis bullosa skin blisters clinical
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have extensive content covering EBS (simplex), JEB, dystrophic EB, and EB acquisita. I have enough material to write a comprehensive answer. Let me now compile everything into a detailed, well-organized response.
Epidermolysis Bullosa — Complete Detail
Definition & Overview
Epidermolysis bullosa (EB) is a group of rare hereditary mechanobullous diseases characterized by extreme fragility of the skin and mucous membranes, resulting in blister formation in response to minor mechanical trauma. The name comes from the Greek epidermis + Latin bullosa (blistered). The unifying pathomechanism is a defect in the structural proteins responsible for dermal-epidermal adhesion — the cleavage plane determines the type.
Four main categories are recognized, each distinguished by the anatomical level of skin splitting:
| Type | Cleavage Plane | Key Protein Defect |
|---|---|---|
| EB Simplex (EBS) | Intraepidermal (within epidermis) | Keratins 5/14, plectin |
| Junctional EB (JEB) | Lamina lucida (within basement membrane) | Laminin-332, collagen XVII, integrins |
| Dystrophic EB (DEB) | Sublamina densa (below basement membrane) | Collagen VII |
| Kindler Syndrome | Mixed (multiple levels) | Kindlin-1 |
| EB Acquisita (EBA) | Sublamina densa (acquired/autoimmune) | Autoantibodies to type VII collagen |
Epidemiology
- Combined incidence: ~19.6 per million live births; prevalence ~11.1 per million population
- EBS is the most common subtype (~70% of cases)
- DEB accounts for ~25%, JEB ~5%
- EBA is very rare: ~0.25 per million/year in Western Europe; higher in Korean and African-American populations
Normal Skin Structure (Relevant to EB)
The dermal-epidermal basement membrane zone (BMZ) has three structural layers:
- Basal keratinocyte plasma membrane — hemidesmosomes anchor here
- Lamina lucida — contains laminin-332, integrin α6β4, collagen XVII (BP180)
- Lamina densa — contains collagen IV, perlecan
- Sub-lamina densa — anchoring fibrils made of collagen VII connect to anchoring plaques
Disruption of any of these layers creates the corresponding EB subtype.
1. Epidermolysis Bullosa Simplex (EBS)
Genetics & Pathomechanism
- Usually autosomal dominant; rare AR forms exist
- Most cases: mutations in KRT5 (keratin 5) or KRT14 (keratin 14) — the intermediate filament proteins of basal keratinocytes
- The mutant keratins form dysfunctional cytoskeletal networks → basal keratinocytes rupture under mechanical stress → intraepidermal blister
- Rarer mutations: PLEC (plectin) → EBS with muscular dystrophy; DST (dystonin/BPAG1); EXPH5 (exophilin 5)
Subtypes
A. Generalized Severe EBS (Dowling-Meara / Herpetiformis)
- Most severe EBS subtype
- Presents at birth with generalized blistering
- Characteristic grouped (herpetiform) blisters on trunk and proximal extremities, healing without scarring
- Oral mucosa frequently involved (extensive erosions)
- Milium formation in infancy (usually resolves in childhood)
- Nail shedding and dystrophic regrowth
- Palmoplantar hyperkeratosis progressing to confluent keratoderma → painful, can cause flexural contractures
- Heat does NOT significantly worsen this subtype (unlike others)
- Rarely: esophageal involvement (erosions to pyloric atresia), laryngeal mucosa affected
B. Generalized Intermediate EBS (Koebner)
- Generalized blistering from birth or early infancy
- Hands, feet, extremities most involved
- Heals with post-inflammatory hyper/hypopigmentation; milia and atrophy rare
- Palmar-plantar hyperkeratosis and erosions; sole thickening appears later in childhood
- Mild oral mucosal erosions, improving with age
- Growth is usually normal
C. Localized EBS (Weber-Cockayne)
- Mildest common subtype
- Blistering predominantly on hands and feet (friction/pressure sites)
- Usually appears in early childhood or adolescence
- No systemic involvement; heals without scarring
D. Rare EBS Variants
- EBS with muscular dystrophy (PLEC mutations): progressive limb-girdle muscular dystrophy + skin blistering
- EBS with mottled pigmentation: mottled dark/light spots on trunk; DSCAM-like gene or KRT5 mutation (R125C)
- EBS Ogna: Norwegian, PLEC mutation, seasonal blistering
- Suprabasal EBS subtypes: lesions just above basal layer; include Lethal acantholytic EBS (DSP mutation), EB superficialis

2. Junctional Epidermolysis Bullosa (JEB)
Genetics & Pathomechanism
- Autosomal recessive
- Cleavage within the lamina lucida (between lamina lucida and basal cell layer)
- Mutations in genes encoding:
- Laminin-332 (LAMA3, LAMB3, LAMC2 — encoding α3, β3, γ2 subunits): ~80% of laminin-332 mutations involve recurrent nonsense mutations in LAMB3
- Collagen XVII / BP180 (COL17A1): hemidesmosomal protein
- Integrins α6 or β4 (ITGA6, ITGB4)
- Null mutations → complete absence of laminin-332 → Herlitz JEB (lethal)
- Missense mutations → reduced/dysfunctional protein → milder phenotypes
Subtypes
A. Herlitz JEB (Generalized Severe / Lethal)
- Most severe JEB; formerly "junctional EB gravis"
- Born with extensive blistering, perioral and perinasal granulation tissue
- Laryngeal and tracheobronchial involvement → hoarseness, respiratory distress
- Severe growth retardation, anemia, sepsis
- Most infants die within first 2 years (respiratory failure, sepsis, failure to thrive)
- Complete absence of laminin-332 on immunofluorescence
B. Non-Herlitz JEB (Generalized Intermediate)
- Less severe; patients survive into adulthood
- Includes Generalized Atrophic Benign EB (GABEB): COL17A1 mutations most common
- Features: alopecia (scarring or non-scarring), nail dystrophy/absence, enamel hypoplasia, periungual granulation tissue, mucous membrane involvement
- Atrophic healing (no milia, no scarring in the classic sense)
C. JEB Localized
- Restricted to hands, feet; milder course
D. Laryngo-Onycho-Cutaneous (LOC) Syndrome
- LAMA3 mutations; nail dystrophy, cutaneous erosions, extensive granulation tissue particularly in conjunctiva and larynx; periorbital sites, elbows, knees
Immunofluorescence Pattern in JEB
- IF: blister forms BELOW the laminin-332 staining (laminin-332 stays on the roof)
- Anti-laminin 332 or anti-collagen XVII antibodies can be used to map the precise level
- Cleavage in lamina lucida → IgG/IgA deposited at BMZ in a linear pattern
3. Dystrophic Epidermolysis Bullosa (DEB)
Genetics & Pathomechanism
- Mutations in COL7A1 (collagen VII gene) — both dominant and recessive forms
- Collagen VII forms anchoring fibrils below the lamina densa, securing the epidermis to dermis
- Cleavage occurs just below the lamina densa in the uppermost dermis
- Blisters heal with scarring (unlike EBS/JEB) — hallmark of DEB
- Severe recessive DEB: null mutations → complete absence of collagen VII and anchoring fibrils
- Milder forms: missense mutations → anchoring fibril dysfunction
Subtypes
A. Recessive DEB (RDEB) — Severe Generalized (formerly Hallopeau-Siemens)
- Most severe form of DEB; presents at birth
- Widespread blistering, erosions, milia formation, scarring
- Progressive scarring leads to:
- Pseudosyndactyly (mitten deformities) of hands and feet — fusion of digits by scar tissue → "mitten hand"
- Esophageal stenosis → dysphagia, malnutrition
- Joint contractures
- Corneal erosions → scarring and visual impairment
- Dental enamel defects
- Squamous cell carcinoma (SCC): dramatically elevated risk — aggressive SCC is the leading cause of death in adults with severe RDEB (lifetime risk >90% by age 55); often multiple, metastatic
- Growth retardation, severe anemia, malnutrition
- Complete absence of anchoring fibrils on electron microscopy
B. Recessive DEB — Generalized Intermediate
- Less severe than Hallopeau-Siemens; some anchoring fibrils preserved
- Blistering, scarring, milia; pseudosyndactyly less severe
- SCC risk still markedly elevated
C. Dominant DEB (DDEB)
- Autosomal dominant; missense mutations in COL7A1 (often glycine substitutions in collagen triple helix)
- Generally milder; localized or generalized
- Pretibial blistering common; milia, scarring, nail dystrophy
- Albopapuloid variant: white papules (pretibial), blistering
- SCC risk elevated but lower than RDEB
Electron Microscopy in DEB
- Sub-lamina densa cleavage
- Absent or rudimentary anchoring fibrils (severe RDEB)
- Reduced / abnormal anchoring fibrils (DDEB, intermediate RDEB)
4. Kindler Syndrome
- Autosomal recessive; mutations in FERMT1 (Kindlin-1)
- Kindlin-1 is a focal adhesion protein linking actin cytoskeleton to extracellular matrix
- Unique: mixed cleavage plane (intraepidermal and junctional)
- Features: photosensitivity (poikiloderma), progressive skin atrophy, mucosal fragility, colitis, urethral stenosis, esophageal/anal strictures
- Blistering tends to improve with age; poikilodermatous changes dominate in adulthood
5. Epidermolysis Bullosa Acquisita (EBA)
Definition & Pathomechanism
EBA is an acquired (autoimmune) subepidermal bullous disease caused by IgG autoantibodies against type VII collagen (NC1 domain), the major component of anchoring fibrils. This distinguishes it fundamentally from hereditary EB.
- Antibody–collagen VII binding → complement activation + neutrophil recruitment → FcγRIV-mediated leukocyte infiltration → dermal-epidermal separation
- Antibody titers parallel disease activity; transplacental transfer → neonatal blistering in babies of affected mothers
- Annual incidence ~0.25/million (Western Europe); higher in Koreans and African-Americans
Clinical Presentations
Two main phenotypes:
1. Non-inflammatory (mechanobullous) variant
- Resembles dystrophic EB clinically
- Tense blisters at trauma-prone sites (knuckles, elbows, knees, sacrum)
- Heals with scarring, milia, nail dystrophy
- No significant inflammation
2. Inflammatory variant
- Resembles bullous pemphigoid (BP)
- Urticarial plaques and vesicles on erythematous base, widespread
- Can also resemble: MMP, Brunsting-Perry MMP, or LABD phenotypically
Diagnosis
- DIF: linear IgG (and/or IgA, C3) at the BMZ — below the lamina densa on immunoelectron microscopy
- IIF on salt-split skin: IgG deposits on the dermal (floor) side of the split (distinguishes from BP, which deposits on epidermal/roof side)
- ELISA / immunoblot: anti-type VII collagen IgG
- Immunoelectron microscopy: gold standard — confirms sublamina densa location of deposits
Treatment
- More refractory to treatment than BP
- Colchicine, dapsone — for non-inflammatory variant
- Systemic corticosteroids, ciclosporin, azathioprine, mycophenolate mofetil
- Rituximab (anti-CD20): emerging evidence (2025 systematic review, PMID 40196952) supports its use in refractory EBA
- IVIg, plasmapheresis for severe/resistant disease
- Infliximab (anti-TNF): some case series evidence
Diagnosis of Hereditary EB
Approach
Neonate/child with blistering
↓
Rule out infection (bullous impetigo, herpes, etc.)
↓
Skin biopsy — at edge of fresh blister (< 24h old)
[Circle marks biopsy site at blister margin — see image above]
↓
1. Light microscopy (H&E): level of split
2. Transmission Electron Microscopy (TEM): ultrastructure
3. Immunofluorescence antigen mapping (IF/IEM):
- Antibodies to laminin-332, collagen VII, collagen XVII, α6β4 integrin
- Reveals protein expression and precise cleavage level
↓
Genetic testing: confirms specific gene mutation
→ guides prognosis, genetic counseling, prenatal diagnosis
Immunofluorescence Antigen Mapping Summary
| Antibody | EBS | JEB | DEB |
|---|---|---|---|
| Anti-K5/K14 | Staining in blister floor | Normal | Normal |
| Anti-laminin-332 | Roof + floor | Floor only (roof absent in Herlitz) | Normal |
| Anti-collagen XVII | Normal | Reduced/absent in GABEB | Normal |
| Anti-collagen VII | Normal | Normal | Absent/reduced |
Prenatal Diagnosis
- Chorionic villus sampling (CVS) at 10–12 weeks: DNA mutation analysis
- Fetal skin biopsy at 16–20 weeks (now rarely needed given genetic testing advances)
- Preimplantation genetic diagnosis (PGD): available for known mutations

Extracutaneous / Systemic Manifestations
| System | Manifestation | Most Common in |
|---|---|---|
| GI | Esophageal strictures, pyloric atresia, dysphagia, malnutrition | RDEB, Herlitz JEB |
| Respiratory | Laryngeal involvement, tracheal stenosis, hoarseness | Herlitz JEB, DEB |
| Ophthalmic | Corneal erosions → scarring, ectropion, symblepharon | RDEB |
| Dental | Enamel hypoplasia → extensive caries | All types, esp. JEB |
| Renal | Amyloidosis (secondary, AA type) | RDEB |
| Hematologic | Chronic iron-deficiency anemia | RDEB |
| Musculoskeletal | Pseudosyndactyly, flexural contractures | RDEB |
| Oncologic | Aggressive SCC | RDEB (highest risk) |
| Cardiac | Dilated cardiomyopathy (rarely, in RDEB) | RDEB |
Management
General / Wound Care (All Types)
- Protective padding and dressings: non-adherent dressings (e.g., Mepitel® / silicone-based), soft foam, tubular bandages
- Blister aspiration with sterile needle to relieve tension (leave blister roof intact)
- Avoid friction, adhesive tapes directly on skin
- Temperature control: avoid heat (worsens EBS)
- Emollients for skin hydration
- Infection prevention: silver-containing dressings (e.g., Mepilex Ag) for colonized wounds
Nutritional Support
- High-calorie, high-protein diet; supplementation with iron, zinc, selenium, vitamins C and D
- Gastrostomy tube (PEG/button) for severe RDEB patients with esophageal strictures
Esophageal/GI Management
- Esophageal dilation (endoscopic) for strictures — careful technique to minimize trauma
- Soft/blended diet
Anemia
- Iron supplementation, erythropoietin; blood transfusion in severe cases
SCC Surveillance
- Annual full-body skin checks from adolescence in RDEB
- Any non-healing wound → biopsy to exclude SCC
- Early surgical excision; palliative approaches for metastatic disease
Pharmacological Approaches
- Tetracyclines (e.g., doxycycline): reduce blistering in some EBS patients
- Retinoids: used in DEB for SCC prophylaxis and wound healing (limited evidence)
- Antipruritic therapy (2024 systematic review, PMID 39069296): gabapentinoids, antihistamines, dupilumab for itch management
Emerging & Gene-Based Therapies
| Approach | Mechanism | Status |
|---|---|---|
| Beremagene geperpavec (B-VEC, Vyjuvek®) | HSV-1 vector delivering COL7A1 gene topically | FDA-approved 2023 for RDEB |
| Gene-corrected cell therapy | COL7A1-corrected iPSC / keratinocyte grafts | Phase I/II trials |
| Exon skipping | Antisense oligonucleotides to skip mutant exon | Phase II (RDEB) |
| Protein replacement | Recombinant collagen VII intradermal injections | Clinical trials |
| Bone marrow / stem cell transplant (BMT) | Allogenic HSC transplant provides collagen VII–producing cells | Phase II; risk of mortality |
| Gentamicin / aminoglycosides | Read-through of premature stop codons (in RDEB with PTC) | Phase II |
| Diacerein 1% cream | Inhibits IL-1β; reduces blister count in EBS-DM | Phase II/III (children) |
| Losartan | TGF-β inhibition → reduce fibrosis | Early clinical trials |
Prognosis Summary
| Type | Prognosis |
|---|---|
| EBS Localized | Excellent; normal life expectancy |
| EBS Generalized (Koebner) | Good; quality of life impaired |
| EBS Dowling-Meara | Good survival; significant morbidity |
| JEB Non-Herlitz | Variable; significant morbidity |
| JEB Herlitz | Very poor; death usually in infancy |
| DEB Dominant | Moderate morbidity; normal life expectancy |
| DEB Recessive (severe) | Poor; major morbidity; SCC main cause of death |
| Kindler Syndrome | Moderate; malignancy risk elevated |
| EBA | Chronic, remitting-relapsing; often refractory |
Key Differential Diagnoses (EB vs Other Blistering Diseases)
| Disease | Key Differentiator |
|---|---|
| Bullous pemphigoid | Anti-BP180/BP230 IgG; IIF roof-side on salt-split skin; older adults |
| Pemphigus vulgaris | Intraepidermal, acantholytic; anti-desmoglein 3/1 |
| Dermatitis herpetiformis | Granular IgA at dermal papillae; gluten-sensitive |
| Staphylococcal scalded skin syndrome | Infection; exfoliatin toxin; no basement membrane defect |
| Bullous impetigo | Localized; S. aureus; positive culture |
| Porphyria cutanea tarda | Photodistributed; elevated urine porphyrins |
| Incontinentia pigmenti | X-linked; Blaschkoid distribution; NEMO mutations |
Summary Classification Table (ISEB 2020 Consensus)
| Major Type | Subtype | Inheritance | Gene | Protein |
|---|---|---|---|---|
| EBS | Generalized Severe | AD | KRT5/KRT14 | K5/K14 |
| EBS | Generalized Intermediate | AD | KRT5/KRT14 | K5/K14 |
| EBS | Localized | AD | KRT5/KRT14 | K5/K14 |
| EBS | with MD | AR | PLEC | Plectin |
| JEB | Generalized Severe (Herlitz) | AR | LAMA3/LAMB3/LAMC2 | Laminin-332 |
| JEB | Generalized Intermediate | AR | COL17A1/LAMB3 | ColXVII/Lam332 |
| JEB | LOC Syndrome | AR | LAMA3 | Laminin α3 |
| DEB | Generalized Severe (RDEB) | AR | COL7A1 | Collagen VII |
| DEB | Dominant | AD | COL7A1 | Collagen VII |
| Kindler | — | AR | FERMT1 | Kindlin-1 |
| EBA | — | Acquired | — | Anti-Col VII IgG |
Sources:
- Fitzpatrick's Dermatology, 9th ed., Ch. 60 — Epidermolysis Bullosa, pp. 1044–1068
- Dermatology 2-Volume Set, 5th ed. (Bolognia), Ch. 32, 71, 95
- Rituximab in EBA: Xenopoulou D et al. J Drugs Dermatol 2025 Apr [PMID 40196952]
- Antipruritic therapies in EB: Welponer T et al. J Dermatol Treat 2024 Dec [PMID 39069296]
Details about pediatrics emergencies and their management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the complete, detailed response on pediatric emergencies.
Pediatric Emergencies — Complete Detail
1. General Approach to Pediatric Emergencies
Primary Survey: ABCDE
Every pediatric emergency begins with a structured primary survey:
| Step | Assessment | Key Actions |
|---|---|---|
| A — Airway | Patency, obstruction | Head-tilt chin-lift / jaw thrust; OPA/NPA; suction |
| B — Breathing | Rate, effort, aeration | Supplemental O₂, BVM ventilation, intubation |
| C — Circulation | HR, BP, perfusion, capillary refill | IV/IO access, fluids, vasopressors |
| D — Disability | GCS, pupils, glucose | Dextrose for hypoglycemia |
| E — Exposure | Temperature, rash, trauma | Remove clothing, prevent hypothermia |
Pediatric Assessment Triangle (PAT)
A rapid <30-second across-the-room assessment:
- Appearance: Tone, interactivity, consolability, cry, gaze
- Work of Breathing: Retractions, nasal flaring, grunting, stridor, head bobbing
- Circulation to Skin: Pallor, mottling, cyanosis
Age-Based Normal Vital Signs
| Age | HR (bpm) | RR (breaths/min) | Systolic BP (mmHg) |
|---|---|---|---|
| Neonate (0–28 days) | 100–160 | 40–60 | 60–90 |
| Infant (1–12 mo) | 100–160 | 30–60 | 70–100 |
| Toddler (1–3 yr) | 90–150 | 24–40 | 80–110 |
| Preschool (3–5 yr) | 80–140 | 22–34 | 80–110 |
| School age (6–12 yr) | 70–120 | 18–30 | 85–120 |
| Adolescent (>12 yr) | 60–100 | 12–16 | 95–140 |
Minimum acceptable systolic BP (hypotension threshold):
- Infants: <70 mmHg
- Children 1–10 years: <70 + (2 × age in years) mmHg
- Children >10 years: <90 mmHg
Weight Estimation
- Broselow tape: Most accurate for children up to ~35 kg
- Formula: Weight (kg) ≈ 2 × (age in years + 4) — for children 1–10 years
2. Pediatric Cardiac Arrest
Epidemiology & Causes
- Pediatric cardiac arrest is mostly asphyxial (respiratory failure → hypoxia) rather than primary cardiac in origin (unlike adults)
- Most common causes: respiratory failure, drowning, sepsis, trauma, SIDS
- Primary arrhythmic arrest (VF/pVT) is rare but seen in congenital heart disease, myocarditis, prolonged QT, Wolff-Parkinson-White, electrolyte disturbances, and drug toxicity
CPR Technique
Compression depth:
- Infants (<1 year): 1.5 inches (≈4 cm) — one-third AP diameter
- Children (>1 year): 2 inches (≈5 cm)
- Rate: 100–120 compressions/minute
- Allow full chest recoil; minimize pauses
Compression technique:
- Infants: 2-finger technique (single rescuer) or 2-thumb encircling technique (preferred, 2 rescuers)
- Children: 1-hand or 2-hand technique over lower half of sternum
Compression-to-ventilation ratio:
- Single rescuer: 30:2
- Two rescuers: 15:2 (for infants and children <8 years)
- Advanced airway in place: continuous compressions at 100–120/min + 1 breath every 2–3 seconds (20–30/min); ventilation should NOT interrupt compressions
Key principle: Minimize pauses; high-quality compressions with full recoil; compress "hard and fast"
AHA 2020 Pediatric Cardiac Arrest Algorithm
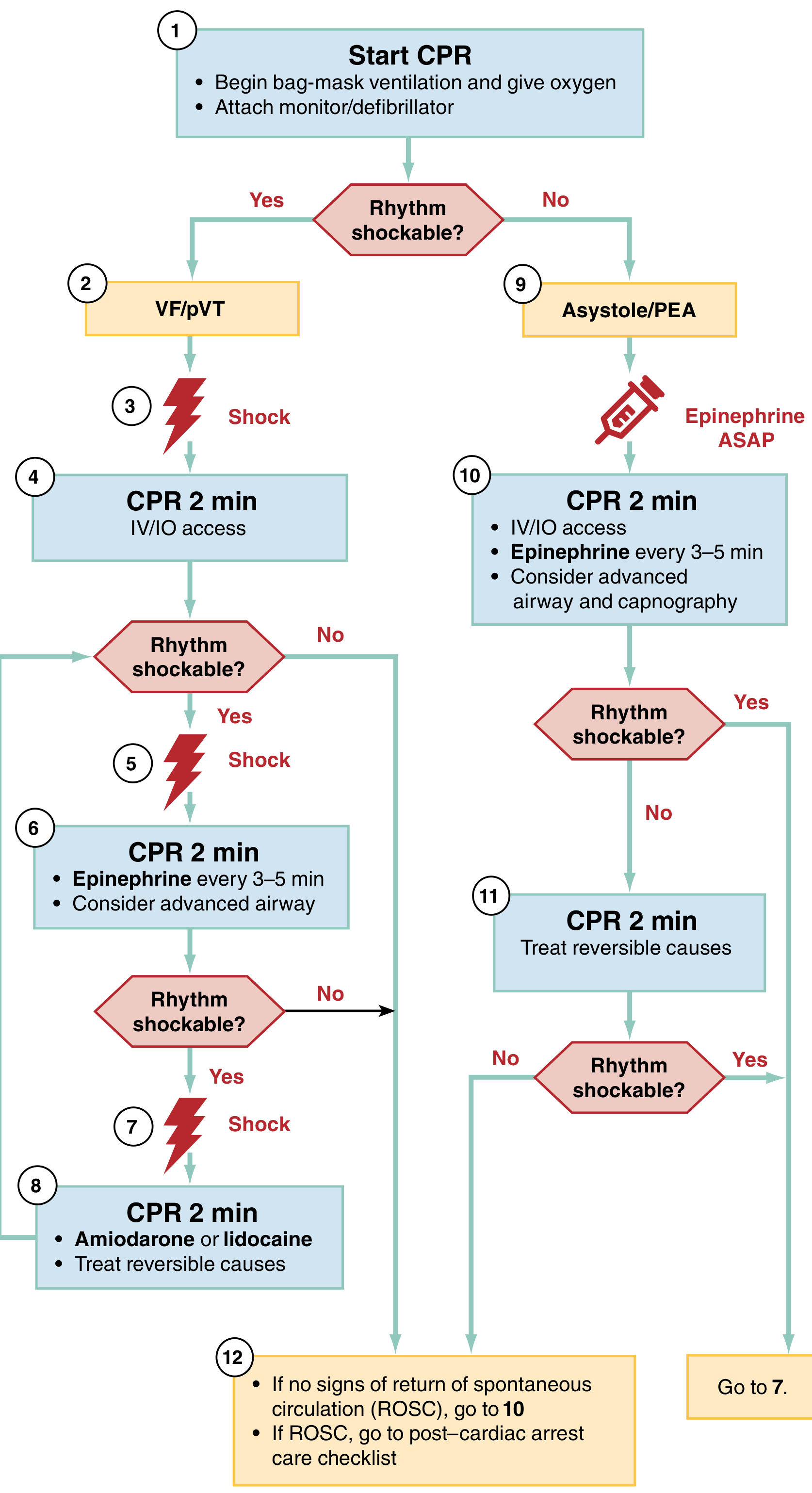
Shockable rhythms (VF/pVT):
- Start CPR → shock ASAP → CPR 2 min + IV/IO access
- After second shock → Epinephrine every 3–5 min
- After third shock → Amiodarone or lidocaine + treat reversible causes
Non-shockable rhythms (Asystole/PEA):
- Start CPR → Epinephrine ASAP → CPR 2 min + IV/IO access
- Epinephrine every 3–5 min; consider advanced airway + capnography
- Treat reversible causes (5H's and 5T's)
Reversible Causes — 5H's and 5T's
| 5H's | 5T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo/Hyperkalemia | Thrombosis (pulmonary) |
| Hypothermia | Thrombosis (coronary) |
Defibrillation
- Initial shock: 2 J/kg
- Subsequent shocks: 4 J/kg (max 10 J/kg or adult dose)
- Use pediatric pads for children <10 kg or <1 year
- Minimize time from rhythm check to shock delivery
Resuscitation Medications
| Drug | Indication | Dose |
|---|---|---|
| Epinephrine | Asystole, PEA, VF, pVT, bradycardia | 0.01 mg/kg IV/IO (0.1 mL/kg of 1:10,000); 0.1 mg/kg ET (1:1000); max 1 mg; repeat every 3–5 min. Infusion: 0.05–2 mcg/kg/min |
| Amiodarone | Shock-refractory VF/pVT | 5 mg/kg IV/IO (max 300 mg); push undiluted if pulseless; repeat up to 15 mg/kg total |
| Lidocaine | VF/pVT (2nd-line after amiodarone) | 1 mg/kg IV/IO bolus |
| Adenosine | SVT (AV nodal reentry) | 0.1 mg/kg IV (max 6 mg); 2nd dose 0.2 mg/kg (max 12 mg); rapid push + flush |
| Atropine | Bradycardia (vagal, organophosphate) | 0.02 mg/kg IV/IO (min 0.1 mg; max 0.5 mg); repeat once; max total 1 mg |
| Calcium chloride | Hypocalcemia, hyperkalemia, Ca-blocker OD | 20 mg/kg IV (max 1 g) over 5 min |
| Dextrose | Hypoglycemia | Neonates: 5–10 mL/kg D₁₀W; Infants/children: 2–4 mL/kg D₂₅W; Adolescents: 1–2 mL/kg D₅₀W |
| Magnesium sulfate | Torsades de pointes, hypomagnesemia | 25–50 mg/kg IV/IO (max 2 g) over 10–20 min |
| Sodium bicarbonate | Severe metabolic acidosis, TCA toxicity, hyperkalemia | 1 mEq/kg IV/IO slow push |
Source: Harriet Lane Handbook, 23rd ed., p. 25–26
Post-Cardiac Arrest Care
- Maintain O₂ saturation 94–99%; PaCO₂ 35–45 mmHg
- Maintain SBP >5th percentile for age
- Target glucose 80–180 mg/dL (avoid hypoglycemia and severe hyperglycemia)
- Continuous EEG monitoring — >10% develop seizures post-arrest, >2/3 evolve to status epilepticus
- Chest X-ray to verify ET tube placement
- Consider therapeutic hypothermia or normothermia for comatose patients after out-of-hospital cardiac arrest
- Evaluate for rehabilitation services
3. Pediatric Airway Emergencies
Airway Assessment
- Signs of obstruction: stridor, grunting, retractions (subcostal, intercostal, supraclavicular), nasal flaring, head bobbing, cyanosis
- Infants depend on nasal breathing — nasal obstruction can cause significant distress
Airway Adjuncts
- OPA (Oropharyngeal airway): use in unconscious patients without gag reflex; correct size = corner of mouth to mandibular angle
- NPA (Nasopharyngeal airway): use in conscious/semiconscious patients; correct size = tip of nose to tragus of ear; contraindicated with significant facial trauma
- BVM ventilation: Can be used indefinitely if effective; bring face into mask (do not push mask down)
Bag-Valve-Mask (BVM) Technique
- E-C clamp grip
- Cricoid pressure (Sellick maneuver) to minimize aspiration
- Adequate seal; watch for symmetric chest rise
- Avoid hyperventilation (compresses cardiac output in arrest)
Endotracheal Intubation
ETT size formulas:
- Uncuffed: (Age/4) + 4 (for children >2 years)
- Cuffed: (Age/4) + 3.5
- Cuffed tubes are preferred in most pediatric settings (reduces need for re-intubation)
Depth of insertion (lip to midtrachea):
- Formula: 3 × ETT internal diameter
- Alternatively: (Age/2) + 12 cm at the lip
Laryngoscope blade selection:
- Neonates/infants: straight blade (Miller) preferred
- Older children: curved blade (Macintosh) acceptable
Upper Airway Emergencies
Croup (Laryngotracheobronchitis)
- Most common in children 6 months–3 years; caused by parainfluenza virus
- Steeple sign on AP neck X-ray (subglottic narrowing)
- Clinical: barky ("seal-like") cough, inspiratory stridor, hoarse voice, low-grade fever
- Management:
- Mild: Dexamethasone 0.15–0.6 mg/kg PO/IM (single dose; max 16 mg); cool mist
- Moderate/Severe: Dexamethasone + nebulized racemic epinephrine 0.05 mL/kg (max 0.5 mL) of 2.25% solution in 3 mL NS; observe ≥2–4 hours after epinephrine (rebound risk)
- Heliox (70:30 helium:oxygen) for severe cases pending other therapy
Epiglottitis
- Bacterial (H. influenzae type b — now rare with vaccination; also S. aureus, Group A Strep)
- Sudden high fever, toxic appearance, drooling, dysphagia, muffled voice, "tripod" position
- "Thumbprint sign" on lateral neck X-ray
- NEVER examine oropharynx without airway backup
- Management: Call anesthesia/ENT immediately; intubation in OR setting; IV ceftriaxone/ampicillin-sulbactam
Foreign Body Aspiration
- Peak age: 1–3 years
- Sudden choking/coughing episode; unilateral wheeze; may have inspiratory stridor if laryngeal
- Conscious child with mild obstruction: Encourage coughing
- Conscious child with severe obstruction (cannot cry/cough/breathe):
- Infant: 5 back blows + 5 chest thrusts (do NOT do abdominal thrusts in infants)
- Child >1 year: 5 back blows + 5 abdominal thrusts (Heimlich)
- Unconscious child: CPR; look in mouth before each ventilation; rigid bronchoscopy for definitive removal
4. Respiratory Emergencies
Bronchiolitis
- Most common lower respiratory tract infection in infants; RSV most common cause
- Age: typically <2 years; peak 2–6 months
- Features: coryza → tachypnea, wheeze, crackles, subcostal retractions, feeding difficulty
- Management (largely supportive):
- Supplemental O₂ to maintain SpO₂ ≥90–92%
- Nasogastric feeds or IV fluids if poor oral intake
- High-flow nasal cannula (HFNC) for moderate-severe cases
- NOT recommended: bronchodilators (albuterol), corticosteroids, antibiotics (unless secondary bacterial infection)
- CPAP/intubation for severe respiratory failure
Acute Asthma / Bronchospasm
Severity Assessment:
| Feature | Mild | Moderate | Severe | Impending Arrest |
|---|---|---|---|---|
| SpO₂ | >95% | 90–95% | <90% | Cyanosis |
| Retractions | None/mild | Moderate | Severe | Paradoxical |
| Speech | Sentences | Phrases | Words | Cannot speak |
| PEFR | >70% | 40–70% | <40% | Unable |
Management:
- Supplemental O₂ → target SpO₂ >92%
- Albuterol (salbutamol): Nebulized 2.5–5 mg (0.15 mg/kg, min 2.5 mg, max 5 mg) q20 min × 3, then q1–4h PRN; MDI with spacer equally effective
- Ipratropium bromide: 250–500 mcg nebulized with albuterol (reduces hospitalizations)
- Systemic corticosteroids: Prednisolone 1–2 mg/kg/day (max 60 mg) × 3–5 days; IV methylprednisolone 1–2 mg/kg if unable to take orally
- Magnesium sulfate IV: 25–75 mg/kg (max 2 g) over 20 min for moderate-severe; reduces hospitalization
- Heliox (70:30): Reduces work of breathing in severe obstruction
- IV/subcutaneous epinephrine or terbutaline for life-threatening bronchospasm
- Intubation + mechanical ventilation: Last resort; use permissive hypercapnia strategy
5. Shock in Children
Classification
| Type | Mechanism | Examples | Hallmarks |
|---|---|---|---|
| Hypovolemic | ↓ Intravascular volume | Dehydration, hemorrhage, burns | ↓ CVP, tachycardia, oliguria |
| Distributive | Maldistribution of flow | Sepsis, anaphylaxis, neurogenic | Warm/bounding pulses (early sepsis) or cold/clammy (late) |
| Cardiogenic | ↓ Cardiac output | Myocarditis, arrhythmia, CHD | ↑ CVP, hepatomegaly, gallop rhythm |
| Obstructive | Impeded cardiac outflow | Tension pneumothorax, tamponade, massive PE | JVD, muffled sounds, absent breath sounds |
Recognition of Shock
Hypotension is late in children — early compensated shock may present with:
- Tachycardia
- Prolonged capillary refill >2 seconds
- Weak peripheral pulses
- Altered mental status, irritability
- Mottling, cool extremities
- Decreased urine output <1 mL/kg/hr
Combination of hypotension + delayed capillary refill → highest mortality predictor in pediatric sepsis.
Initial Management of Shock (All Types)
- Supplemental O₂; airway management
- Vascular access: IV × 2 large-bore or intraosseous (IO) if IV fails after 2 attempts or >60–90 seconds
- Isotonic crystalloid bolus: Normal saline or Lactated Ringer's 10–20 mL/kg over 5–20 minutes; reassess and repeat as needed
- Treat underlying cause
6. Septic Shock
Background
- Leading cause of death in children worldwide
- Mortality approaches 25% in severe pediatric sepsis in ICU
- Risk factors: age <1 month, immunosuppression, chronic disease, invasive devices, genitourinary anomalies
Pathophysiology
Immune dysregulation → pro- and anti-inflammatory cascades → vasodilation, myocardial depression, complement activation, DIC, excess nitric oxide → end-organ hypoperfusion → multi-organ failure.
Diagnosis
- SIRS criteria: Abnormal temperature (>38.5°C or <36°C) OR abnormal WBC + tachycardia or tachypnea + suspected infection
- Septic shock: Hypotension refractory to ≥40 mL/kg IV fluids in 1 hour, OR any hypotension (BP <5th percentile for age)
- Children may have warm shock (early — warm skin, bounding pulses, wide pulse pressure) or cold shock (late — cold extremities, mottling, weak pulses, narrow pulse pressure)
- Lactate >4 mmol/L in ED associated with OR 3.3 for 30-day mortality
- qSOFA (altered mental status + hypotension + tachypnea) helps identify organ dysfunction
Management (Surviving Sepsis Campaign 2020 Pediatric Guidelines)
Hour 1 Bundle:
| Step | Action |
|---|---|
| 1. Recognize | Screen systematically; do not delay treatment for labs |
| 2. Access | IV or IO within 5 minutes |
| 3. Cultures | Blood cultures × 2 (aerobic/anaerobic) before antibiotics if possible; do NOT delay antibiotics >1 hour |
| 4. Antibiotics | Broad-spectrum IV within 1 hour of recognition (delays increase mortality) |
| 5. Fluid resuscitation | 10–20 mL/kg isotonic fluid bolus over 5–20 min; reassess after each bolus; titrate to clinical endpoints |
| 6. Vasopressors | Start if fluid-refractory (≥40–60 mL/kg administered) or signs of fluid overload |
Fluid Resuscitation Notes:
- Maximum: 40–60 mL/kg total in first hour; stop if signs of fluid overload (hepatomegaly, crackles)
- FEAST trial (Africa, 2011): Fluid boluses ↑ mortality in resource-limited settings; careful titration essential
- After 40 mL/kg without improvement → vasopressors
Vasopressors (fluid-refractory septic shock):
- Epinephrine or norepinephrine as first-line (both acceptable)
- Dopamine: second-line if epinephrine/norepinephrine unavailable
- Vasopressin: adjunctive for catecholamine-refractory shock
- Central venous access not required to start vasopressors in ED; can be given peripherally or via IO temporarily
Antibiotics (empirical):
- Community-acquired (no focus): Ceftriaxone or ampicillin-sulbactam; add vancomycin if MRSA risk
- Healthcare-associated/immunocompromised: Anti-pseudomonal coverage (pip-tazo or meropenem) + vancomycin
- Neonates (<28 days): Ampicillin + gentamicin ± cefotaxime (for meningitis coverage)
- Meningococcemia: Ceftriaxone; add steroids (dexamethasone) if meningitis
Corticosteroids:
- Hydrocortisone: 1–2 mg/kg/day (max 200 mg/day) IV if catecholamine-refractory shock; not routine
- Avoid high-dose steroids
7. Anaphylaxis
Diagnosis Criteria (NIAID/FAAN 2006)
Anaphylaxis is likely when any one of three criteria is fulfilled:
- Acute illness involving skin/mucosa + either respiratory compromise or hypotension
- Two or more of the following after exposure to a likely allergen: skin/mucosal involvement, respiratory compromise, hypotension, persistent GI symptoms
- Hypotension after exposure to a known allergen
Most common precipitants in children: foods (peanuts, tree nuts, milk, eggs, shellfish — highest mortality in peanut allergy + asthma + atopy)
Management
First-line (DO NOT DELAY):
- Epinephrine IM (anterolateral thigh): 0.01 mg/kg of 1 mg/mL solution (max 0.5 mg); autoinjector: EpiPen Jr 0.15 mg (<30 kg), EpiPen 0.3 mg (≥30 kg)
- Repeat every 5–15 minutes if no improvement
- Place patient supine (Trendelenburg if hypotensive)
- Call for help; prepare for airway management
Subsequent management:
- Supplemental O₂
- IV fluid bolus (10–20 mL/kg NS) for hypotension/anaphylactic shock
- H₁ antihistamine (diphenhydramine 1 mg/kg IV/IM, max 50 mg) — adjunctive, NOT first-line
- H₂ antihistamine (ranitidine 1 mg/kg IV) — adjunctive
- Systemic corticosteroids (methylprednisolone 1–2 mg/kg IV, max 60 mg) — prevent biphasic reaction
- Salbutamol/albuterol nebulized for bronchospasm
- IV epinephrine infusion (0.05–2 mcg/kg/min) for refractory anaphylaxis/anaphylactic shock
Observation:
- Minimum 4–6 hours after epinephrine (biphasic reaction risk: 1–20%)
- Admit overnight for severe reactions or if biphasic concern
Discharge:
- Prescribe epinephrine autoinjector (2 prescribed)
- Written anaphylaxis action plan
- Allergen avoidance counseling
- Referral to allergist
8. Status Epilepticus
Definition
- Seizure lasting >5 minutes, OR two or more seizures without return to baseline consciousness
Classification
- Convulsive SE: Generalized tonic-clonic, most recognizable
- Non-convulsive SE (NCSE): Subtle motor findings or none; only detectable on EEG; common after cardiac arrest
Febrile Seizure
- Simple febrile seizure: Primary generalized, age 6–60 months, <15 minutes, non-focal, does NOT recur within 24 hours
- Management: Identify fever source; no neuroimaging, EEG, or antiseizure medications needed in well-appearing, fully immunized child with normal neuro exam and no meningeal signs
- Complex febrile seizure: Focal, >15 minutes, or recurs within 24 hours → further evaluation indicated
Status Epilepticus Management (Rosen's Emergency Medicine)
TIME 0–5 min: STABILIZE
• Position: maximize ventilation; protect airway
• O₂ via mask/NC; suction oropharynx
• If trauma suspected: C-spine precautions
• NPA if airway obstructed (avoid OPA — causes vomiting on awakening)
• Monitor: HR, BP, RR, SpO₂, temperature
• Bedside glucose → correct hypoglycemia
• IV/IO access → send: electrolytes, glucose, Ca, Mg, LFT, RFT, AED levels, CBC, urine tox
TIME 5 min: FIRST-LINE — BENZODIAZEPINES
• Lorazepam 0.1 mg/kg IV/IO (max 4 mg) — PREFERRED
• Diazepam 0.2 mg/kg IV/IO (max 10 mg); 0.5 mg/kg rectal (max 20 mg)
• If NO IV access: Midazolam 0.2 mg/kg IM (max 10 mg); or intranasal/buccal
[Delays >10 min in giving BZD → higher death, longer seizure, more complications]
TIME 10 min (if seizure continues): SECOND BENZODIAZEPINE DOSE
• Repeat benzodiazepine (same dose) after 5 minutes of continued seizure
TIME 15–20 min: SECOND-LINE AGENTS (choose one)
• Levetiracetam 60 mg/kg IV (max 4,500 mg) over 10 min
• Fosphenytoin 20 mg PE/kg IV/IM (max 1,500 mg PE) at 3 mg PE/kg/min
• Valproic acid 40 mg/kg IV (max 3,000 mg) over 10 min
⚠️ Valproate CONTRAINDICATED: liver disease, thrombocytopenia, possible metabolic disease
• Levetiracetam and fosphenytoin have comparable efficacy; levetiracetam may have fewer adverse effects
TIME 30–45 min: REFRACTORY STATUS EPILEPTICUS
• Third benzodiazepine or repeat second-line agent
• Consider RSI and intubation (use propofol or ketamine — both have antiepileptic activity)
• EEG monitoring if possible (NCSE common)
• Third-line: Phenobarbital 15–20 mg/kg IV (max 1 g)
SUPER-REFRACTORY SE (>24h despite anesthesia):
• Midazolam infusion (0.05–2 mg/kg/hr)
• Propofol infusion (⚠️ avoid >48h in children — propofol infusion syndrome)
• Ketamine infusion
• Topiramate via NG tube
• Consider: pyridoxine (neonates/infants), immunotherapy (NMDAR encephalitis)
Intubation choice: Short-acting NMB (succinylcholine) preferred to allow monitoring of continued seizure activity; RSI drug with antiepileptic property (propofol, ketamine).
Correct metabolic causes:
- Hypoglycemia: Dextrose (see dosing above)
- Hyponatremia: 3% NaCl 2–4 mL/kg IV over 20 min
- Hypocalcemia: Calcium gluconate 50–100 mg/kg IV
- Pyridoxine deficiency: 100 mg IV (neonates)
9. Diabetic Ketoacidosis (DKA) in Children
Diagnosis
- Glucose >200 mg/dL + pH <7.3 or HCO₃ <15 mEq/L + ketonemia/ketonuria
- Severe: pH <7.1 or HCO₃ <5 mEq/L
- DKA at diagnosis more common in children <5 years
Dreaded complication: Cerebral edema (rare ~1%, but mortality 20–25%)
- Risk factors: young age, high BUN, severe acidosis, rapid fluid administration, early insulin
- Symptoms: headache, altered mental status, bradycardia with hypertension, unequal pupils
Management
1. Fluid Resuscitation:
- Shock: 10–20 mL/kg NS bolus (reassess; repeat if needed)
- Rehydration: Replace estimated deficit over 48 hours (deficit calculated from % dehydration)
- Typical rate: maintenance + deficit spread over 48 hours using 0.9% or 0.45% NaCl
2. Insulin:
- Begin insulin ONLY after at least 1 hour of IV fluids and K⁺ >3.5 mEq/L
- Regular insulin IV infusion: 0.05–0.1 units/kg/hour (start at lower end in DKA with cerebral edema risk)
- Do NOT give insulin bolus (increases cerebral edema risk)
- Target glucose fall: 50–100 mg/dL/hour; add dextrose to IV fluids when glucose <250–300 mg/dL
3. Potassium:
- Initially elevated (despite total body depletion due to acidosis)
- Replace K⁺ when K⁺ <5.5 mEq/L and good urine output: add 20–40 mEq/L KCl (or KPO₄) to IV fluids
- Insulin must NOT be started if K⁺ <3.5 mEq/L without concurrent K⁺ replacement
4. Bicarbonate:
- NOT routinely recommended (may worsen paradoxical CSF acidosis and cerebral edema)
- Consider only for life-threatening hyperkalemia or pH <6.9 with cardiovascular compromise
5. Cerebral Edema Treatment (if suspected):
- Mannitol: 0.5–1 g/kg IV over 20 min
- Hypertonic saline (3%): 2.5–5 mL/kg IV over 15 min (alternative to mannitol)
- Restrict fluids; elevate head of bed
- Urgent CT head to confirm; neurosurgical consultation
10. Meningitis / Encephalitis
Bacterial Meningitis
Classic triad: Fever + Headache + Neck stiffness (meningismus)
- In neonates/infants: bulging fontanelle, high-pitched cry, hypothermia, poor feeding, seizures
- Kernig's sign: Hip flexed 90°; inability to extend knee >135°
- Brudzinski's sign: Passive neck flexion → involuntary hip/knee flexion
Common organisms by age:
| Age | Organisms |
|---|---|
| Neonates (<28 days) | Group B Strep, E. coli, Listeria |
| 1–3 months | Above + S. pneumoniae, N. meningitidis |
| 3 months–18 years | S. pneumoniae, N. meningitidis |
| >18 years | S. pneumoniae, N. meningitidis, Listeria (>50 yr) |
Management:
- Blood cultures (before LP if possible — do NOT delay antibiotics for LP)
- Empiric antibiotics IMMEDIATELY:
- Neonates: Ampicillin + cefotaxime ± gentamicin
- Children >3 months: Ceftriaxone 100 mg/kg/day IV (max 4 g) + Vancomycin (if resistant pneumococcus concern)
- Dexamethasone 0.15 mg/kg IV q6h × 4 days: start 15–30 min before or with first antibiotic dose; reduces hearing loss and neurologic sequelae in H. influenzae and pneumococcal meningitis
- LP (cerebrospinal fluid analysis) after stabilization:
| CSF Finding | Bacterial | Viral | TB/Fungal |
|---|---|---|---|
| Appearance | Turbid/purulent | Clear | Cloudy/xanthochromic |
| WBC | >1000 (PMN) | 10–500 (lymphocytes) | 100–500 (lymphocytes) |
| Protein | ↑↑ >100 mg/dL | Normal/mildly ↑ | ↑↑ |
| Glucose | ↓ (<40 mg/dL) | Normal | ↓ |
- Chemoprophylaxis: Rifampin or ciprofloxacin for close contacts of N. meningitidis
11. Trauma in Children
Pediatric Trauma Differences
- Higher surface area:body weight ratio → greater heat loss and fluid shifts per kg
- Chest wall more compliant → internal injury without rib fractures; pulmonary contusion common
- Larger head:body ratio → head injury more common and severe
- Abdominal organs relatively larger → liver/spleen more exposed
- Growth plates open → Salter-Harris fractures; ligaments stronger than growth plates
AMPLE History
- Allergies, Medications, Past medical history, Last meal, Events/Environment
Non-Accidental Trauma (Child Abuse) — Red Flags
- Bruising in non-mobile infant (<6 months)
- Bruising in unusual locations (torso, ears, neck, buttocks)
- Fractures inconsistent with developmental stage
- Retinal hemorrhages → Shaken Baby Syndrome
- Posterior rib fractures (virtually pathognomonic for abuse)
- Multiple fractures of different ages
- Delay in seeking care; inconsistent history
Skeletal survey: Mandatory for children <2 years with suspected abuse
12. Neonatal Emergencies
Neonatal Resuscitation (NRP Algorithm)
- Golden minute: Complete initial steps and reassess within 60 seconds
- Initial steps: Warmth, dry/stimulate, position airway, suction (only if secretions obstruct airway)
- Assess: Respiratory effort, HR (most important), color/tone
| HR | Action |
|---|---|
| >100 bpm, breathing | Routine care; supplemental O₂ if cyanosis |
| 60–100 bpm, not breathing | PPV (21% O₂ in term; up to 30–100% if meconium/depressed) |
| <60 bpm | PPV + chest compressions (3:1 ratio); IV epinephrine |
- Meconium-stained amniotic fluid + vigorous infant: Routine care (suctioning no longer recommended routinely)
- Meconium + depressed infant: Intubate and suction before PPV
Neonatal Hypoglycemia
- Glucose <40 mg/dL (some guidelines <45 mg/dL) in first 24 hours
- Risk factors: LGA/SGA infant, diabetic mother, prematurity, hypothermia, sepsis
- Treatment: Early feeding; D₁₀W 2 mL/kg IV if symptomatic or not responding to feeding
Neonatal Jaundice / Hyperbilirubinemia
- Physiologic jaundice: Appears day 2–3, peaks day 4–5; total bilirubin <15 mg/dL
- Pathologic: Jaundice <24 hours, total bilirubin >17 mg/dL in term infant, direct bili >2 mg/dL
- Management: Phototherapy (blue light 430–490 nm); exchange transfusion for severe/rapidly rising levels
13. Hypertensive Emergency in Children
Definition
Hypertensive emergency = severe hypertension + end-organ damage (encephalopathy, seizures, retinopathy, heart failure, AKI)
Management
- Target: Reduce BP by no more than 25% in first 8 hours, then gradual reduction over 24–48 hours (rapid reduction → ischemia)
- IV agents: Labetalol, nicardipine, sodium nitroprusside
- Oral agents (non-emergency): Amlodipine, enalapril, propranolol
14. Common Pediatric Toxicological Emergencies
| Toxin | Key Features | Treatment |
|---|---|---|
| Acetaminophen | NAC within 8–10h of ingestion; hepatotoxicity >24h | NAC (oral/IV) per Rumack-Matthew nomogram |
| Iron | GI symptoms → shock → hepatotoxicity | Deferoxamine IV |
| Opioids | Respiratory depression, miosis, coma | Naloxone 0.01 mg/kg IV; repeat q2–3 min |
| Benzodiazepines | Sedation; rarely life-threatening alone | Flumazenil (use with caution; seizure risk) |
| TCA | Arrhythmias, seizures, QRS >100 ms | Sodium bicarbonate 1–2 mEq/kg IV |
| Organophosphates | Cholinergic crisis (SLUDGE/DUMBELS) | Atropine (large doses); pralidoxime |
| Beta-blockers | Bradycardia, hypotension | Glucagon, calcium, high-dose insulin-euglycemia |
| Clonidine | Opioid-like: bradycardia, sedation, miosis | Naloxone (may work); atropine for bradycardia |
Quick Reference: Pediatric Emergency Doses
| Drug | Dose | Route | Max |
|---|---|---|---|
| Epinephrine (cardiac arrest) | 0.01 mg/kg | IV/IO | 1 mg |
| Adenosine (SVT) | 0.1 mg/kg (1st), 0.2 mg/kg (2nd) | IV rapid push | 6 mg / 12 mg |
| Atropine | 0.02 mg/kg | IV/IO | 0.5 mg |
| Lorazepam (seizure) | 0.1 mg/kg | IV/IO | 4 mg |
| Diazepam rectal | 0.5 mg/kg | PR | 20 mg |
| Midazolam | 0.2 mg/kg | IM/IN | 10 mg |
| Dexamethasone (croup) | 0.6 mg/kg | PO/IM/IV | 10 mg |
| Albuterol (asthma) | 0.15 mg/kg | Nebulized | 5 mg |
| Magnesium (asthma) | 25–75 mg/kg | IV over 20 min | 2 g |
| Naloxone (opioid) | 0.01 mg/kg | IV/IO/IM/IN | 2 mg |
| Mannitol (↑ICP) | 0.5–1 g/kg | IV over 20 min | — |
| 3% NaCl (SIADH/cerebral edema) | 2–4 mL/kg | IV over 15–20 min | — |
| Normal saline bolus | 10–20 mL/kg | IV/IO | 60 mL/kg cumulative |
| Dextrose (hypoglycemia — infant) | 2–4 mL/kg D₂₅W | IV/IO | — |
Summary: Pediatric Emergency Priorities
Any Child → PAT Assessment (30 seconds)
↓
Primary Survey: ABCDE
↓
Airway patency → ventilate if needed (BVM first)
Circulation → IV/IO access → fluid bolus 10–20 mL/kg NS
↓
Cardiac arrest → High-quality CPR + algorithm (VF/pVT vs. asystole/PEA)
Septic shock → Fluids + cultures + antibiotics within 1 hour + vasopressors if needed
Status epilepticus → Benzodiazepines → second-line AEDs → RSI if refractory
Anaphylaxis → Epinephrine IM 0.01 mg/kg IMMEDIATELY
DKA → Slow rehydration + insulin (after 1h fluids) + K⁺ monitoring
Meningitis → Antibiotics + dexamethasone IMMEDIATELY
Sources:
- Rosen's Emergency Medicine, 9th ed., Chapters 158, 169 — Pediatric Resuscitation & Status Epilepticus
- Harriet Lane Handbook, 23rd ed. (Johns Hopkins) — Resuscitation Medications & Airway
- Miller's Anesthesia, 10th ed. — Pediatric Cardiac Arrest and Resuscitation
- AHA 2020 Pediatric Advanced Life Support (PALS) Guidelines
- Surviving Sepsis Campaign 2020 Pediatric Guidelines
Nursing management in Pediatrics emergencies and nursing procedures in details
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.