Necrosis pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
I now have comprehensive, authoritative content from both Robbins textbooks with pathological images. Let me compile the full answer.
Necrosis - Pathology
Definition
Necrosis is a pathologic form of cell death resulting from severe, irreparable injury. It is distinct from apoptosis (programmed cell death) in that it is always pathological, triggers inflammation, and involves uncontrolled breakdown of cellular membranes.
Main causes include: ischemia, microbial toxins, burns and chemical/physical injury, and situations where active proteases leak out of cells (e.g., pancreatitis).
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 54-56
- Robbins & Kumar Basic Pathology, p. 21-23
Pathogenesis
Necrosis follows a sequence:
- Severe injury damages membranes and mitochondria irreparably
- Lysosomal enzymes enter the cytoplasm and digest the cell from within
- Cellular contents leak through the damaged plasma membrane into extracellular space
- DAMPs (Damage-Associated Molecular Patterns) are released - including ATP (from damaged mitochondria) and uric acid (DNA breakdown product)
- DAMPs are recognized by receptors on macrophages, triggering phagocytosis and cytokine-driven inflammation
- Inflammatory cells produce more proteolytic enzymes, leading to clearance of necrotic debris
This necrosis-associated leakage of intracellular proteins forms the basis of blood biomarkers - cardiac troponins (detectable as early as 2 hours after myocardial necrosis), transaminases in hepatocyte necrosis, and alkaline phosphatase in bile duct damage.
Microscopic (Morphologic) Changes
Cytoplasmic Changes
- Increased eosinophilia (pink on H&E) - due to denatured cytoplasmic proteins binding eosin dye, plus loss of basophilic RNA
- Glassy, homogeneous appearance - from loss of glycogen particles
- Vacuolated, "moth-eaten" cytoplasm - after enzymatic digestion of organelles
- Myelin figures - phospholipid whorls from disrupted membranes; may calcify (dystrophic calcification)
- EM: discontinuities in plasma and organelle membranes; marked mitochondrial dilation with amorphous intramitochondrial densities; disrupted lysosomes
Nuclear Changes (3 Patterns)
| Pattern | Description |
|---|---|
| Pyknosis | Nuclear shrinkage + increased basophilia (DNA condenses into dark, shrunken mass) |
| Karyorrhexis | Fragmentation of the pyknotic nucleus |
| Karyolysis | Fading of basophilia due to DNase-mediated digestion of DNA; nucleus dissolves within 1-2 days |
Morphologic Patterns of Tissue Necrosis
There are 6 recognized patterns, each with distinct causes and appearances:
1. Coagulative Necrosis
- Most common type
- Tissue architecture is preserved for days because the injurious stimulus denatures structural proteins AND enzymes, blocking proteolysis
- Affected tissue becomes firm in texture
- Histology: intensely eosinophilic, anucleate "ghost cells" with preserved cell outlines
- Caused by: ischemia (infarction) in all solid organs except the brain
- A localized area is called an infarct
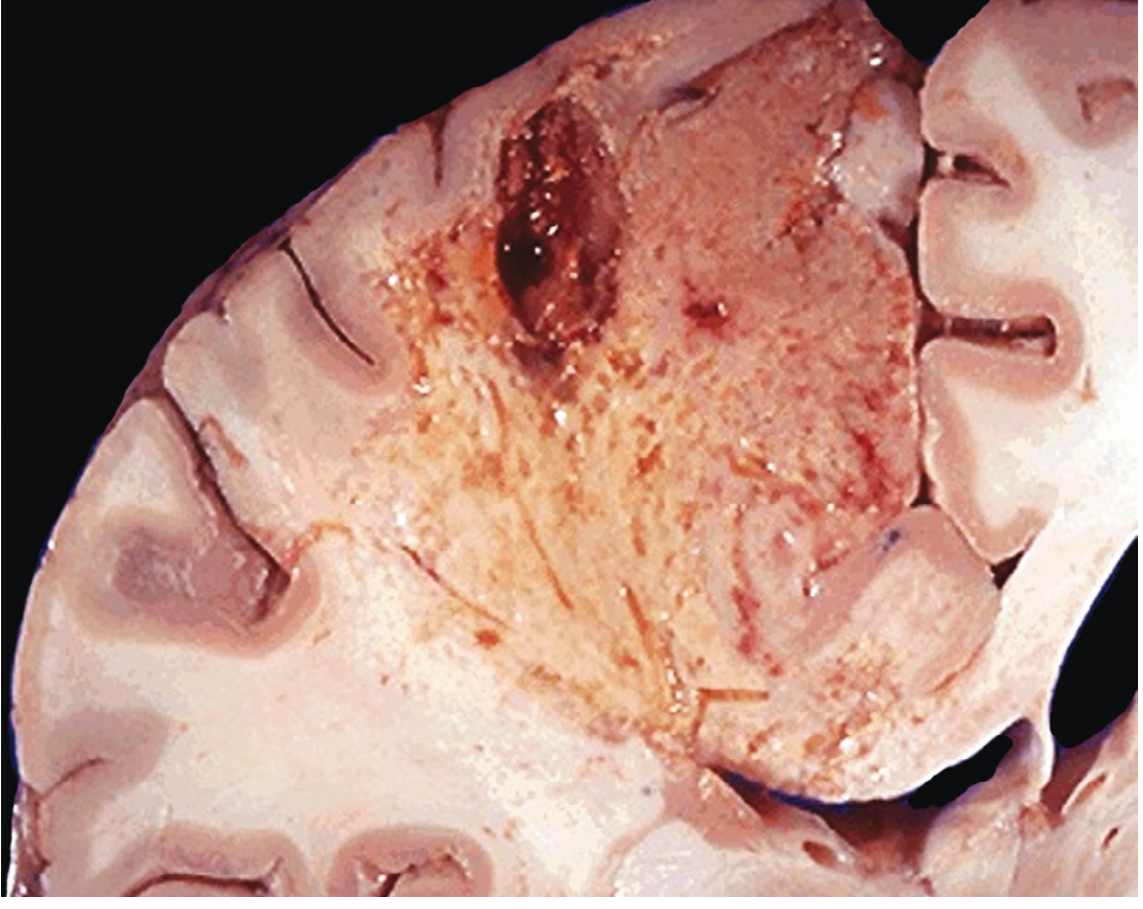
2. Liquefactive Necrosis
- Dead cells are completely digested, transforming tissue into a viscous liquid
- Caused by: bacterial or fungal infections (leukocytes accumulate and release enzymes); also seen in CNS ischemia (brain infarcts) for unknown reasons
- When due to acute bacterial infection: material is creamy yellow = pus; localized pus collection = abscess
3. Gangrenous Necrosis
- Not a distinct pattern - essentially coagulative necrosis of a limb (usually lower leg) that has lost blood supply, involving multiple tissue planes
- Dry gangrene: ischemic coagulative necrosis
- Wet gangrene: superimposed bacterial infection converts it to liquefactive necrosis
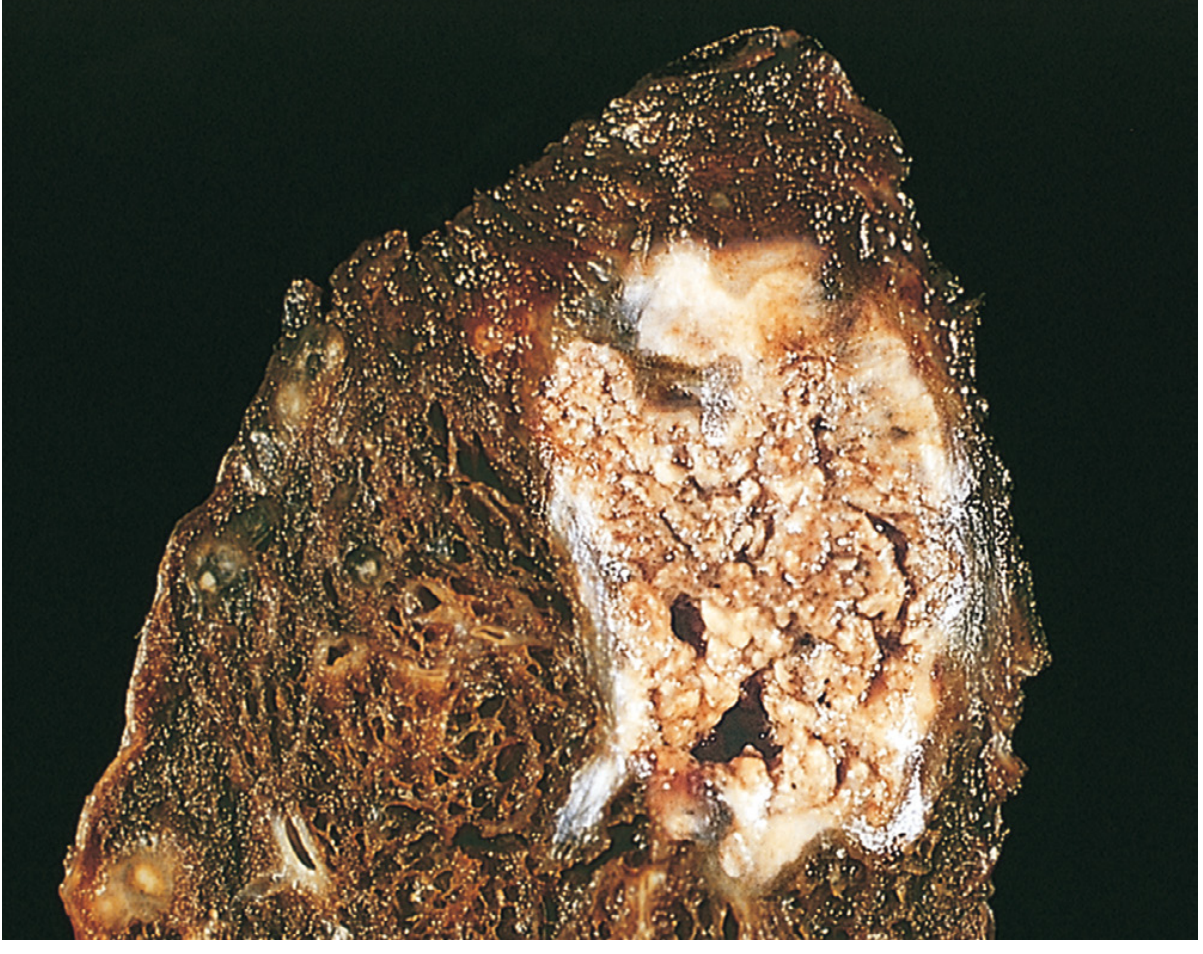
4. Caseous Necrosis
- Classic feature of tuberculous infection (and other mycobacterial/fungal granulomatous diseases)
- Gross: friable, yellow-white, "cheese-like" appearance ("caseous" = cheeselike)
- Histology: structureless collection of fragmented/lysed cells with amorphous granular pink debris; tissue architecture is completely obliterated (unlike coagulative necrosis)
- Surrounded by a collection of macrophages (epithelioid cells) = granuloma
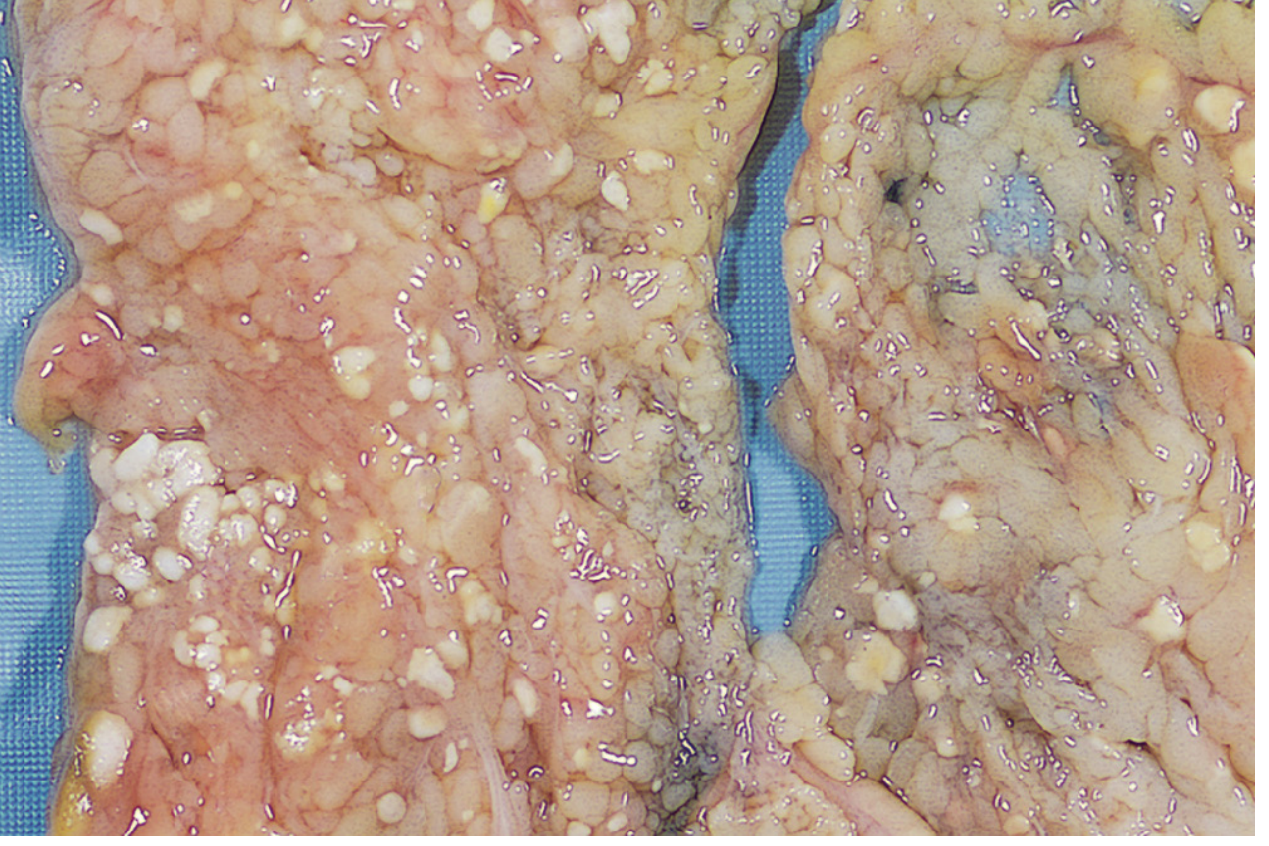
5. Fat Necrosis
- Focal areas of fat destruction
- Acute pancreatitis is the prototypical cause - pancreatic lipases leak from damaged acinar cells and digest peritoneal fat cells, releasing triglycerides
- Fatty acids combine with calcium -> chalky white deposits (saponification = calcium soap formation)
- Histology: shadowy outlines of necrotic fat cells + basophilic calcium deposits + inflammatory reaction
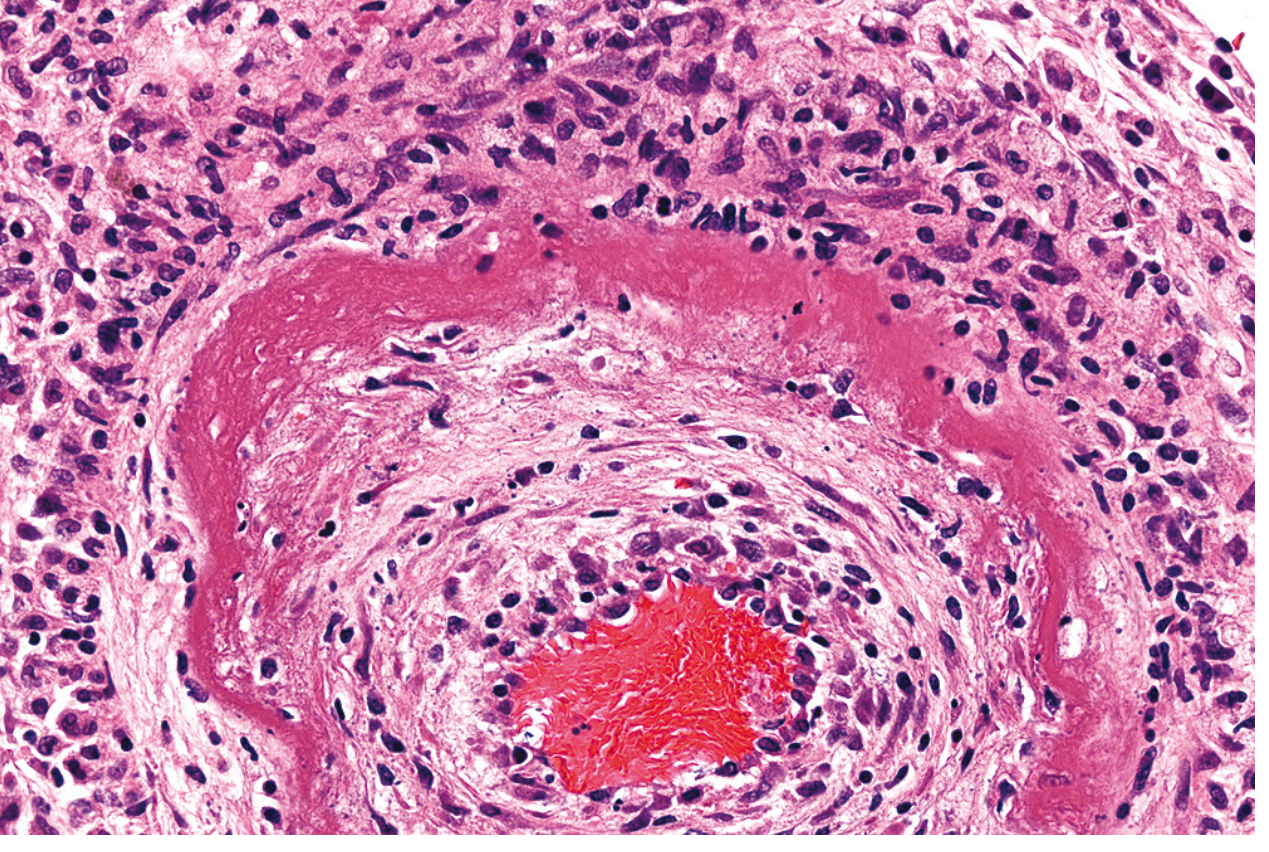
6. Fibrinoid Necrosis
- Detected only microscopically (no distinctive gross appearance)
- Seen in immune complex vasculitis (antigen-antibody complexes deposited in vessel walls) and malignant hypertension
- Histology: bright pink (eosinophilic), amorphous "fibrin-like" material in vessel walls = "fibrinoid" appearance
- Associated with: certain forms of vasculitis, glomerulonephritis
Summary Table
| Type | Cause | Key Feature | Example |
|---|---|---|---|
| Coagulative | Ischemia (all organs except brain) | Preserved architecture; ghost cells | Myocardial infarct |
| Liquefactive | Bacterial infection; CNS ischemia | Complete dissolution; pus | Brain abscess, brain infarct |
| Gangrenous | Vascular occlusion of limb | Coagulative ± liquefactive | Diabetic foot gangrene |
| Caseous | Tuberculosis, fungi | Cheesy; granuloma; architecture lost | Pulmonary TB |
| Fat | Acute pancreatitis; trauma | Chalky white saponification | Peritoneal fat in pancreatitis |
| Fibrinoid | Immune vasculitis; malignant HTN | Bright pink vessel wall deposits | Polyarteritis nodosa |
Necrosis vs. Apoptosis (Key Distinction)
| Feature | Necrosis | Apoptosis |
|---|---|---|
| Nature | Always pathologic | Physiologic or pathologic |
| Membrane integrity | Lost early | Maintained until late |
| Cell size | Swelling | Shrinkage |
| Nuclear change | Pyknosis/karyorrhexis/karyolysis | Chromatin condensation, fragmentation |
| Inflammation | Yes (DAMPs released) | No |
| Mechanism | Uncontrolled; enzymatic digestion | Regulated; caspase-mediated |
Other Regulated Forms of Necrosis (Modern Concepts)
- Necroptosis - programmed necrosis with features of both necrosis and apoptosis; regulated by specific signaling pathways (RIP kinases)
- Pyroptosis - cell death associated with release of pro-inflammatory cytokines (IL-1β, IL-18); important in innate immunity and infection
Sources: Robbins & Kumar Basic Pathology, 10th ed., pp. 21-24 | Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 54-57
This is a shared conversation. Sign in to Orris to start your own chat.