Antihypertensive drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full overview of antihypertensive drugs.
Antihypertensive Drugs
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition; Goodman & Gilman's Pharmacological Basis of Therapeutics
Sites of Action
All antihypertensive agents act at one or more of four anatomic control sites, interfering with normal blood pressure regulation mechanisms:
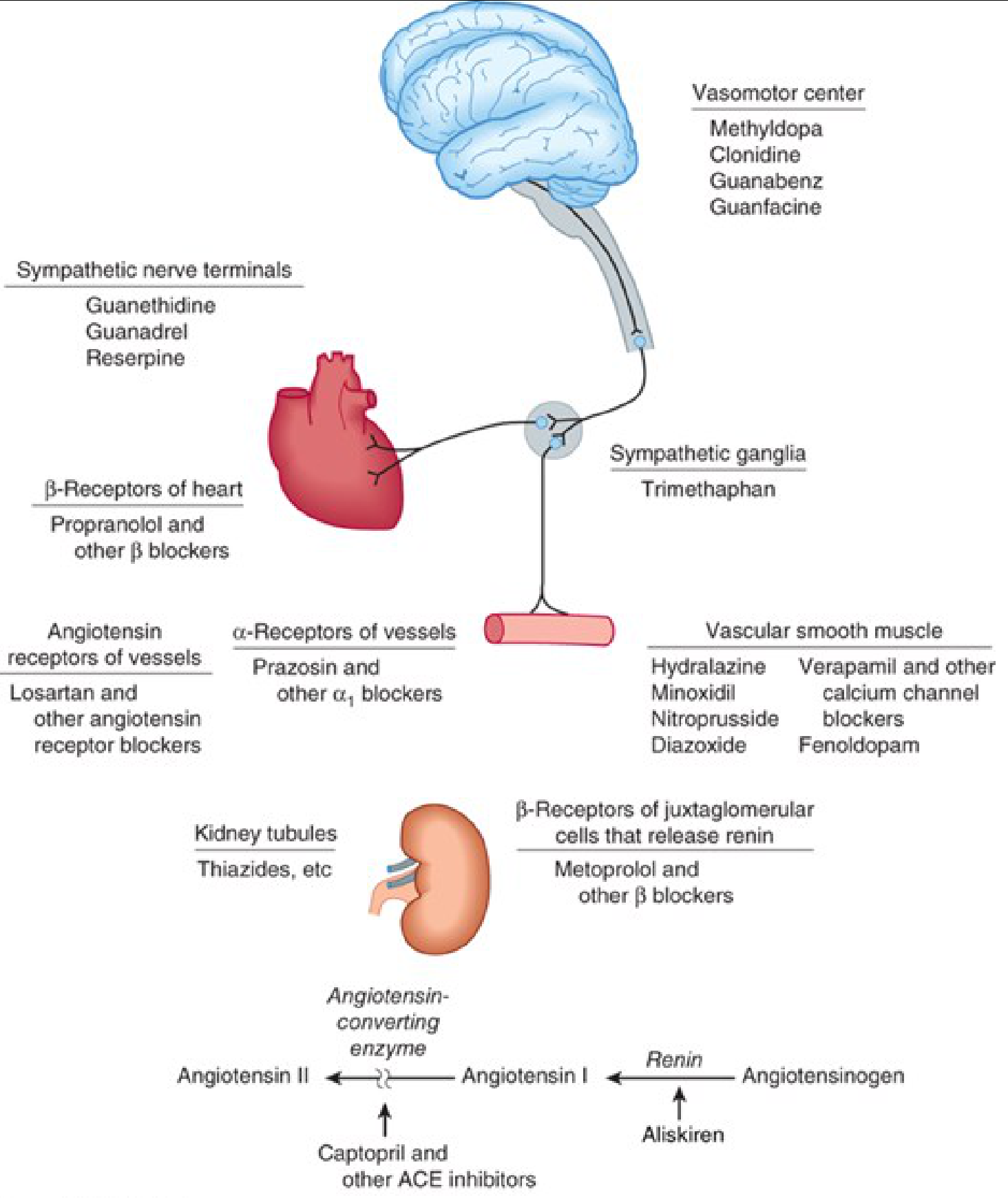
Classification by Mechanism
1. Diuretics
Mechanism: Deplete body sodium stores → initially ↓ blood volume and cardiac output → after 6–8 weeks, cardiac output normalizes and peripheral vascular resistance ↓.
| Subclass | Examples | Notes |
|---|---|---|
| Thiazides | Hydrochlorothiazide, Chlorthalidone | First-line for mild–moderate hypertension; chlorthalidone has longer action |
| Loop diuretics | Furosemide, Bumetanide, Torsemide | For severe hypertension, renal insufficiency (GFR <30–40 mL/min), heart failure, cirrhosis |
| Potassium-sparing | Spironolactone, Eplerenone, Amiloride | Prevent K⁺ depletion; MR antagonists especially useful in resistant hypertension |
Dosing note: Thiazides are antihypertensive at low doses (25–50 mg HCTZ); loop diuretics continue to ↑ effect with dose escalation.
2. Renin-Angiotensin System (RAS) Agents
ACE Inhibitors
Examples: Captopril, Enalapril, Lisinopril, Ramipril, Fosinopril
Mechanism: Block conversion of Angiotensin I → Angiotensin II; also prevent bradykinin degradation.
Key benefits:
- Reduce proteinuria and slow CKD progression (especially in diabetes — indicated even without hypertension)
- Reduce mortality in heart failure and post-MI
- Reduce incidence of new-onset diabetes in high-CV-risk patients
- Improve intraglomerular hemodynamics (↓ efferent arteriolar resistance → ↓ glomerular capillary pressure)
Adverse effects:
| Effect | Mechanism |
|---|---|
| Dry cough ± wheeze | ↑ Bradykinin / Substance P |
| Angioedema | ↑ Bradykinin |
| Hyperkalemia | ↓ Aldosterone |
| Acute renal failure | In bilateral renal artery stenosis |
| Hypotension (first dose) | Volume depletion states |
| Neutropenia/proteinuria | Especially captopril at high doses |
Contraindications: Pregnancy (2nd & 3rd trimester — risk of fetal hypotension, anuria, renal failure, death; 1st trimester teratogenicity also implicated).
Drug interactions: K⁺ supplements/K⁺-sparing diuretics (→ hyperkalemia); NSAIDs (↓ hypotensive effect).
Angiotensin Receptor Blockers (ARBs)
Examples: Losartan, Valsartan, Candesartan, Irbesartan, Olmesartan, Telmisartan, Azilsartan, Eprosartan
Mechanism: Selectively block AT₁ receptors. No effect on bradykinin → more selective angiotensin blockade than ACEi. Also have potential for more complete angiotensin blockade (non-ACE enzymes can still generate Ang II with ACEi).
Similarities to ACEi: Similar benefits in heart failure and CKD. Cough and angioedema occur but are uncommon (no bradykinin accumulation). Contraindicated in pregnancy.
Current use: Once primarily used as ACEi alternatives; now used interchangeably as first-line agents.
Direct Renin Inhibitor
Aliskiren — inhibits renin, preventing conversion of angiotensinogen → Angiotensin I (shown in the diagram above). Less commonly used; not combined with ACEi or ARBs (excess RAS blockade).
3. Sympathoplegic Agents
Subdivided by site of action in the sympathetic reflex arc:
a) CNS-Acting Agents (Vasomotor Center)
| Drug | Mechanism |
|---|---|
| Methyldopa | α₂ agonist (via active metabolite α-methylnorepinephrine); reduces sympathetic outflow |
| Clonidine | α₂ agonist; also imidazoline receptor agonist |
| Guanabenz, Guanfacine | α₂ agonists similar to clonidine |
Note: Abrupt discontinuation of clonidine causes rebound hypertension.
b) Sympathetic Ganglia Blockers
- Trimethaphan — nicotinic receptor blocker at ganglia; rarely used (mainly historical)
c) Adrenergic Nerve Terminal Blockers
| Drug | Mechanism |
|---|---|
| Reserpine | Depletes catecholamines from storage vesicles |
| Guanethidine, Guanadrel | Block norepinephrine release from terminals |
d) β-Adrenoceptor Blockers
Examples: Propranolol, Metoprolol, Atenolol, Carvedilol, Labetalol, Bisoprolol, Nebivolol
Mechanisms:
- ↓ Heart rate and contractility → ↓ cardiac output
- ↓ Renin release from juxtaglomerular cells (β₁ blockade)
- Central ↓ sympathetic outflow
Cautions: Avoid in asthma/COPD (non-selective β blockers); considered less useful than CCBs in the elderly unless heart failure is present.
e) α₁-Adrenoceptor Blockers
Examples: Prazosin, Doxazosin, Terazosin
Mechanism: Block α₁ receptors on blood vessels → vasodilation. Do not impair reflex tachycardia.
4. Direct Vasodilators
Act directly on vascular smooth muscle.
Arterial Vasodilators
| Drug | Mechanism | Route | Notes |
|---|---|---|---|
| Hydralazine | Opens K⁺ channels / NO-mediated | Oral/IV | Causes reflex tachycardia + Na⁺ retention → requires combination with β-blocker + diuretic; lupus-like syndrome at high doses |
| Minoxidil | K⁺ channel opener (ATP-sensitive) | Oral | Reserved for severe resistant hypertension; causes hypertrichosis and fluid retention |
| Nitroprusside | Releases NO → cGMP-mediated relaxation | IV infusion | Hypertensive emergencies; cyanide toxicity with prolonged use → give thiosulfate or hydroxocobalamin |
| Diazoxide | K⁺ channel opener | IV (formerly); Oral (for hypoglycemia) | No longer used for HTN in USA; also inhibits insulin release |
| Fenoldopam | D₁ receptor agonist → renal and peripheral vasodilation | IV | Preferred in HTN emergencies with renal impairment |
Key pharmacology of hydralazine/vasodilator combination rationale:
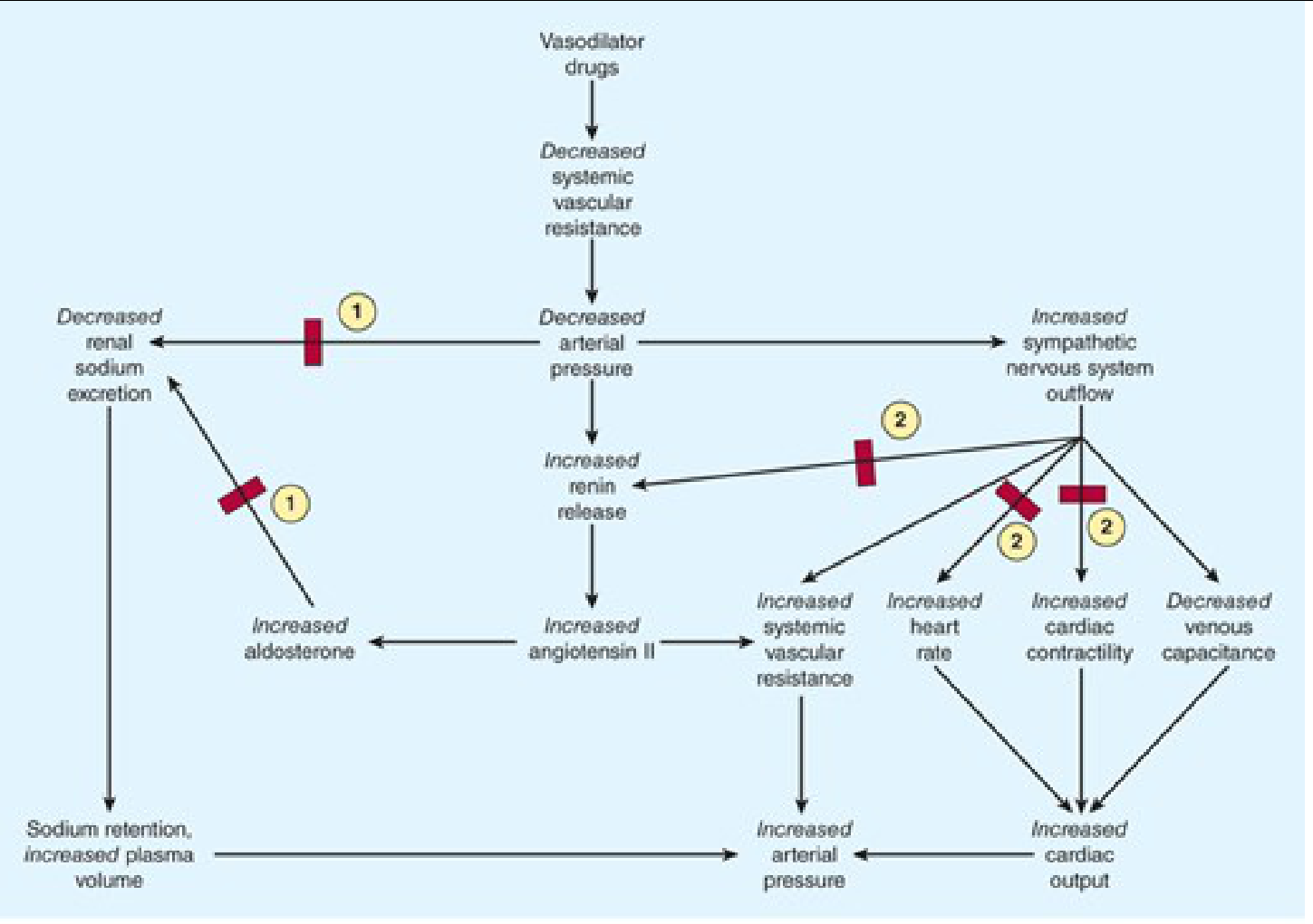
Vasodilators → ↓ SVR → compensatory ↑ heart rate + Na⁺/water retention → β-blocker (blocks tachycardia) + diuretic (blocks fluid retention) are added to maintain effect.
5. Calcium Channel Blockers (CCBs)
Examples: Amlodipine, Nifedipine, Felodipine (dihydropyridines — vascular selective); Verapamil, Diltiazem (non-dihydropyridines — also cardiac effects)
Mechanism: Block L-type Ca²⁺ channels in vascular smooth muscle → vasodilation; non-DHP agents also ↓ HR and contractility.
Key uses: Effective and safe across most patient groups; particularly useful in elderly and patients with angina (atherosclerotic). Preferred over β-blockers in elderly without heart failure.
Polypharmacy Principles
- Up to 40% of hypertensives require 3+ drugs ("resistant hypertension").
- First exclude: excess dietary Na⁺, NSAIDs/stimulant drugs, secondary HTN.
- Standard approach: start monotherapy → add second agent from different class with different toxicity profile → add third (usually includes a diuretic).
- Mineralocorticoid antagonists (spironolactone) are particularly effective as add-on for resistant hypertension.
- Renal denervation: investigational for advanced CKD/resistant cases.
Drug Selection by Patient Profile
| Patient Condition | Preferred Agent(s) |
|---|---|
| Diabetes + proteinuria | ACE inhibitor or ARB (even without HTN) |
| Heart failure | ACE inhibitor/ARB + β-blocker + aldosterone antagonist |
| Post-MI | ACE inhibitor + β-blocker |
| CKD (GFR <30) | Loop diuretic (thiazides less effective) + ACEi/ARB |
| Elderly | CCB, thiazide; avoid high-dose thiazides (arrhythmias, gout, DM risk) |
| Angina | CCB or β-blocker |
| Asthma/COPD | Avoid non-selective β-blockers |
| Pregnancy | Methyldopa, Labetalol, Nifedipine; avoid ACEi/ARBs |
| Resistant HTN (3+ drugs) | Add spironolactone |
| Hypertensive emergency | IV nitroprusside, IV labetalol, IV nicardipine, IV fenoldopam |
Pharmacokinetics Summary (Selected Agents)
| Drug | Half-life | Bioavailability | Usual Dose | Renal Dose Reduction? |
|---|---|---|---|---|
| Amlodipine | 35 h | 65% | 5–10 mg/d | No |
| Atenolol | 6 h | 60% | 50–100 mg/d | Yes |
| Enalapril (→ enalaprilat) | 11 h | ~40% | 10–20 mg once/twice daily | Yes (most ACEi except fosinopril/moexipril) |
| Lisinopril | 12 h | ~25% | 10–80 mg/d | Yes |
| Losartan | ~2 h (active metabolite 6–9 h) | ~33% | 50–100 mg/d | No |
| Captopril | ~2 h | 60–70% | 25–50 mg 2–3×/d | Yes |
Key Adverse Effects at a Glance
| Drug Class | Major Adverse Effects |
|---|---|
| Thiazides | Hypokalemia, hyperglycemia, hyperuricemia, hyponatremia |
| Loop diuretics | Hypokalemia, ototoxicity, hypomagnesemia |
| ACE inhibitors | Dry cough, angioedema, hyperkalemia, teratogenicity, acute renal failure (bilateral RAS) |
| ARBs | Similar to ACEi but no cough; teratogenic |
| β-blockers | Bronchoconstriction, bradycardia, masking of hypoglycemia, fatigue |
| CCBs (DHP) | Peripheral edema, reflex tachycardia, flushing |
| CCBs (non-DHP) | Bradycardia, heart block, constipation (verapamil) |
| α₁-blockers | First-dose orthostatic hypotension, dizziness |
| Clonidine | Rebound HTN on withdrawal, sedation, dry mouth |
| Hydralazine | Reflex tachycardia, lupus-like syndrome (high doses) |
| Minoxidil | Hypertrichosis, fluid retention, pericardial effusion |
| Nitroprusside | Cyanide toxicity (prolonged infusion), methemoglobinemia |
Katzung's Basic and Clinical Pharmacology, 16th Ed. — Chapter 11; Goodman & Gilman's Pharmacological Basis of Therapeutics — Chapter 9
This is a shared conversation. Sign in to Orris to start your own chat.