Cryptochordism
Reading File
Finding Sources
Searching PubMed
cryptorchidism management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to provide a thorough answer on cryptorchidism.
Cryptorchidism (Undescended Testis)
Definition
Cryptorchidism (from Greek kryptos = hidden, orchis = testis) refers to failure of one or both testes to descend into their normal scrotal position. The testis may reside in the retroperitoneum, at the internal inguinal ring, within the inguinal canal, or at the external ring.
Embryology & Pathogenesis
Testicular descent is a complex, hormonally orchestrated process:
- In the 5th–6th week of embryological life, gonads arise from the urogenital ridge on the posterior abdominal wall.
- In the 7th–8th months, the testis descends along the inguinal canal into the scrotum, dragging the processus vaginalis with it.
- Key regulatory molecules include INSL3 (insulin-like factor 3), RXFP2/LGRF8, AMH (anti-Müllerian hormone), and HOX gene family receptors (HOX10).
- Androgens are required in the 4th month to induce regression of the cranial suspensory ligament.
- Failure of any of these steps results in cryptorchidism.
By birth, ~95% of infants have both testes in the scrotum. — Campbell-Walsh-Wein Urology
Epidemiology
| Group | Prevalence |
|---|---|
| Preterm infants | ~30% |
| Full-term newborns | 1–4% |
| By 1 year of age | <1.5% (due to spontaneous descent) |
- Unilateral cryptorchidism is ~twice as common as bilateral.
- A pattern of maternal inheritance is noted, but the intrauterine environment also plays a role. — Campbell-Walsh-Wein Urology
Classification
| Type | Description |
|---|---|
| True undescended testis | Arrested along normal descent path (retroperitoneal, canalicular, prescrotal) |
| Ectopic testis | Has exited the external ring but come to rest in an abnormal location (over rectus abdominis, medial thigh, perineum) |
| Retractile testis | Has a normal cord length; reaches and stays in scrotum when warm/relaxed — NOT an undescended testis |
| Vanishing testis | Absent gonad due to intrauterine accident or failure of development |
Clinical Presentation & Examination
- Inspection: hypoplastic or poorly rugated scrotum on the affected side.
- Palpation technique (child should be warm and relaxed):
- Ask caregivers if the testis is ever visible in the scrotum during a warm bath or sleep (supports retractile testis).
- Examine supine; have the child cross their legs or sit cross-legged to dampen the cremasteric reflex.
- Apply soap to the inguinal canal and use one hand above the canal to "milk" the testis downward.
- If the testis reaches the scrotum and stays there, it is retractile — not undescended.
- If the testis is impalpable, consider abdominal location or congenital absence.
Distinguishing retractile from true undescended testes is clinically critical, as management differs. — Smith and Tanagho's General Urology, 19th Ed.
Complications
| Complication | Notes |
|---|---|
| Infertility | Thermal injury to spermatogonia from higher abdominal temperature; reduced spermatogonia evident histologically after age 2. Bilateral cryptorchidism carries ~70% paternity rates vs. 96% for unilateral with orchidopexy |
| Testicular malignancy | Cryptorchidism is a factor in ~10% of testicular malignancies (most commonly germ cell tumors). Risk persists post-orchidopexy but scrotal location facilitates earlier detection. Intra-abdominal testes carry the highest risk |
| Testicular torsion | Abnormal gubernacular attachment increases susceptibility |
| Inguinal hernia | Patent processus vaginalis is commonly associated |
| Psychological impact | Empty scrotum in developing males |
The evidence points to an inherent testicular abnormality predisposing to both incomplete descent and malignancy — not malignancy secondary to the abnormal environment. — Schwartz's Principles of Surgery, 11th Ed.
Investigations
- Ultrasound: Generally not recommended for routine cryptorchidism — poor sensitivity for localizing an undescended testis and does not alter surgical management. Exception: obese child where identifying an inguinal testis on US simplifies surgical approach.
- MRI/Laparoscopy: Preferred for non-palpable testes; laparoscopy is the procedure of choice for locating and treating abdominal testes.
- Hormonal evaluation: Indicated when bilateral undescended testes are combined with micropenis (to rule out hypogonadism and disorders of sex development).
Management
Timing
- Observe for the first 6 postnatal months — spontaneous descent may occur.
- If no descent by 6 months, surgery should be performed before 12 months (corrected gestational age).
- Rationale: spontaneous descent is unlikely after 2–6 months in full-term males; early orchidopexy restores testicular growth and preserves spermatogonia. — Campbell-Walsh-Wein Urology
Hormonal Therapy
- hCG (chorionic gonadotropin): May occasionally stimulate descent in bilateral cases where hormonal insufficiency is suspected. If no descent after ~1 month, proceed to surgery.
- GnRH: Has been used for germ cell maturation as an adjunct.
- Current AUA and most modern guidelines do not recommend hormonal therapy as primary treatment — surgery is the treatment of choice. — Campbell-Walsh-Wein Urology; Schwartz's
Surgical: Orchidopexy
Palpable testes (inguinal/canalicular):
- Standard inguinal orchidopexy through a groin + scrotal incision — mobilize the spermatic cord and secure the testis in a subdartos pouch.
Non-palpable / abdominal testes:
- Diagnostic laparoscopy first to confirm location.
- Single-stage laparoscopic orchidopexy if cord length is adequate.
- Two-stage Fowler-Stephens orchidopexy if the testis is too high:
- Stage 1: Clip the testicular vessels laparoscopically to allow collateral development via the vas deferens (months of waiting).
- Stage 2: Mobilize the testis with a swath of peritoneum carrying the vas collaterals; success rate >90%.
- Orchiectomy: For postpubertal patients with a small, dysgenetic, or poorly viable testis.
Post-pubertal undescended testis
A 2024 systematic review (PMID 39399296) confirms that management in this group must weigh malignancy risk heavily — orchiectomy vs. orchidopexy is individualized based on testis viability and contralateral testis status.
Prognosis
- Unilateral cryptorchidism treated with childhood orchidopexy: paternity rate ~96% (comparable to controls); inhibin B ~2/3 of normal.
- Bilateral cryptorchidism: paternity rate ~70%; inhibin B ~1/3 of normal; sperm density consistently lower.
- Fertility impairment primarily reflects seminiferous epithelium dysfunction, not Leydig cell (testosterone) failure.
- Malignancy risk persists post-orchidopexy but is reduced; scrotal location allows self-examination for early detection. — Campbell-Walsh-Wein Urology
Sources: Campbell-Walsh-Wein Urology (3-Vol Set) | Schwartz's Principles of Surgery 11e | Smith and Tanagho's General Urology 19e | Grainger & Allison's Diagnostic Radiology | Harriet Lane Handbook 23e
Growth plate
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
epiphyseal growth plate zones histology
Reading File
Reading File
Excellent — I now have rich material from histology, pathology, surgery, and emergency medicine textbooks. Let me compose the comprehensive answer.
The Growth Plate (Physis / Epiphyseal Plate)
Definition & Location
The growth plate (also called the physis or epiphyseal plate) is a transverse disc of hyaline cartilage located between the epiphysis and metaphysis of growing long bones. It is the engine of longitudinal bone growth via endochondral ossification. It persists from birth until skeletal maturity, when it closes and leaves behind a dense epiphyseal line.
Embryology & Formation
Long bones develop via endochondral ossification:
- A mesenchymal cartilage anlage (mold) forms at ~8 weeks gestation.
- A primary ossification center appears in the diaphysis — osteoblasts deposit cortex under the periosteum.
- Secondary ossification centers form in the epiphyses after birth.
- Plates of cartilage become entrapped between the two expanding ossification centers → forming the growth plate (physis).
Flat bones (skull, clavicle) form by intramembranous ossification — direct osteoblast deposition without a cartilage mold; they do not have growth plates. — Robbins Cotran & Kumar Pathologic Basis of Disease
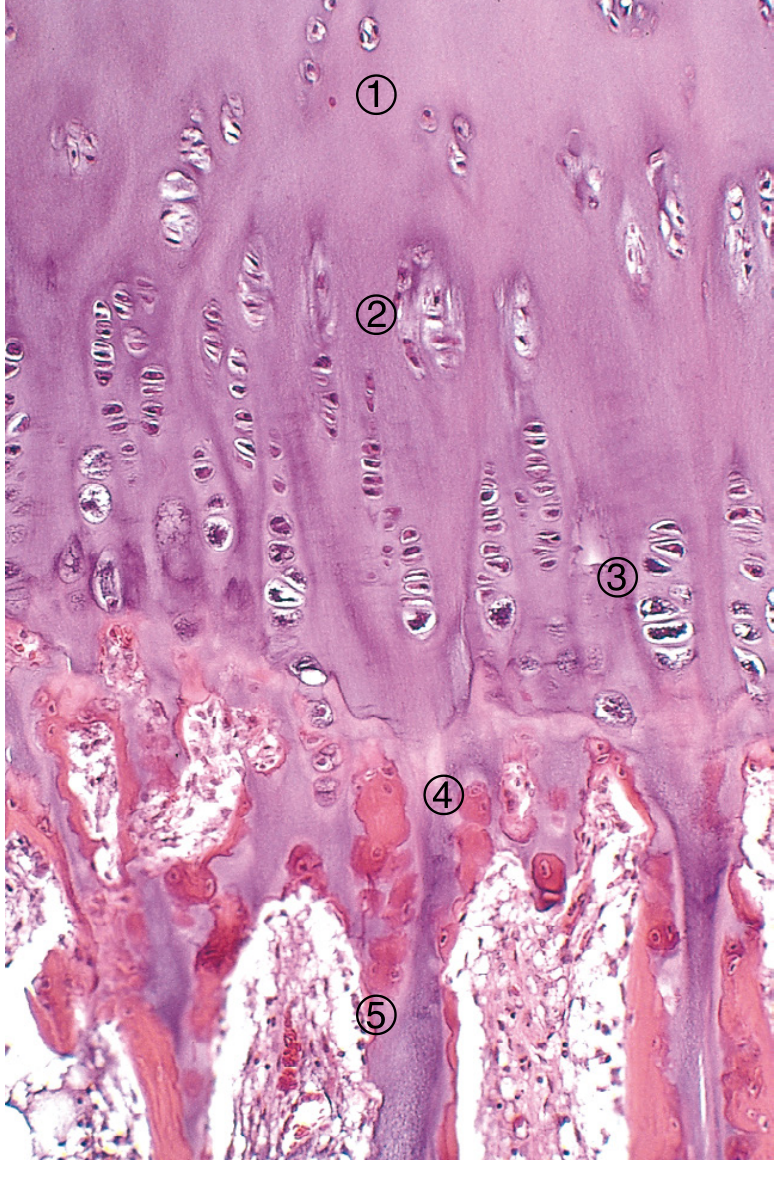
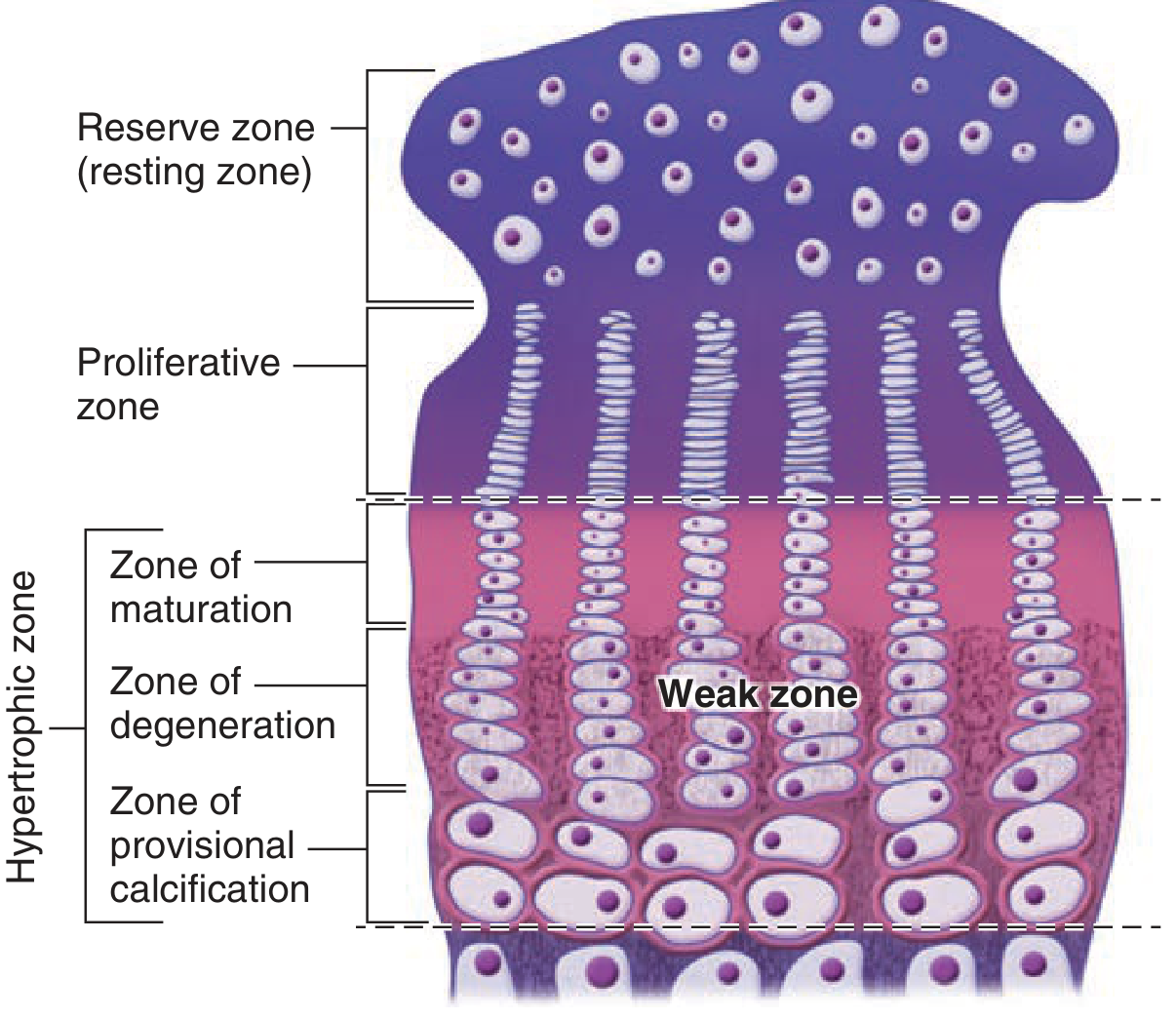
Zones of the Growth Plate
From epiphysis → diaphysis (5 zones):
| Zone | Histology | Function | Key Molecules |
|---|---|---|---|
| 1. Reserve (Resting) zone | Small, scattered chondrocytes in hyaline cartilage matrix | Stem cell reservoir; anchors plate to epiphysis | PTHrP, SOX9 |
| 2. Zone of proliferation | Chondrocytes dividing rapidly; organized into columns (like stacked coins) | Produces new cartilage matrix → pushes epiphysis away → lengthens bone | GH/IGF-1, Indian hedgehog (Ihh), Wnt/β-catenin, SOX9; type II & XI collagen |
| 3. Zone of hypertrophy | Chondrocytes enlarge 10–20×; clear cytoplasm (glycogen) | Increases column height; secretes type X collagen; triggers vascular invasion | VEGF, RANKL, FGF-3 (inhibits further proliferation), RUNX2 |
| 4. Zone of calcification (mineralization) | Hypertrophic chondrocytes degenerate/undergo apoptosis; matrix calcifies | Calcified matrix serves as scaffold for bone deposition | Alkaline phosphatase (TNAP), RANKL |
| 5. Zone of resorption (primary spongiosa) | Blood vessels + osteoprogenitor cells invade; calcified cartilage spicules remain | Osteoblasts deposit osteoid on spicules → primary spongiosa (earliest trabeculae) | Osteoblasts, osteoclasts |
Key principle: The thickness of the epiphyseal plate remains constant during growth — the rate of new cartilage production (proliferation zone) equals the rate of resorption. Actual bone lengthening occurs because new matrix production pushes the epiphysis away from the diaphysis. — Histology: A Text and Atlas, Wheater's
Hormonal & Molecular Regulators
| Factor | Source | Effect on Growth Plate |
|---|---|---|
| Growth hormone (GH) | Anterior pituitary | Induces & maintains chondrocyte proliferation (via IGF-1) |
| IGF-1 | Liver / local | Stimulates proliferating zone chondrocytes |
| Thyroid hormone | Thyroid | Acts on proliferating chondrocytes → induces hypertrophy |
| Indian hedgehog (Ihh) | Prehypertrophic chondrocytes | Coordinates proliferation & differentiation; stimulates PTHrP |
| PTHrP | Perichondrial stromal cells | Maintains chondrocyte proliferation; delays hypertrophy |
| FGFs (FGF-3) | Mesenchymal cells | Inhibit proliferation; promote differentiation |
| BMPs (TGF-β family) | Various | Diverse effects on proliferation and hypertrophy |
| Wnt/β-catenin | Proliferating zone | Promotes chondrocyte proliferation & maturation |
| Sex steroids (estrogen) | Gonads | Accelerate epiphyseal closure at puberty |
— Robbins, Cotran & Kumar Pathologic Basis of Disease
Blood Supply
The growth plate has a dual blood supply:
- Epiphyseal vessels (from the secondary ossification center) supply the reserve and proliferative zones.
- Metaphyseal vessels supply the zone of resorption/primary spongiosa.
- The hypertrophic zone is relatively avascular and relies on diffusion — making it the weakest zone and the most common site of physeal fracture.
Epiphyseal Closure
- When maximal growth is achieved, chondrocyte proliferation ceases.
- Remaining cartilage completes its cycle (hypertrophy → calcification → ossification).
- Epiphyseal and diaphyseal marrow cavities become confluent.
- A dense epiphyseal line (seen on X-ray) marks the former growth plate site.
- Timing is governed by estrogen (hence women close earlier than men) and thyroid/GH.
- "Bone age" is assessed radiographically by the appearance and fusion of ossification centers. — Schwartz's Principles of Surgery, 11th Ed.
Growth Plate Injuries — Salter-Harris Classification
Because the physis is unossified and biomechanically weak, it fractures more readily than attached ligaments in children. The Salter-Harris (SH) classification guides prognosis and treatment:
| Type | Fracture Pattern | Prognosis | Notes |
|---|---|---|---|
| I | Through physis only (transverse); epiphysis separates from metaphysis | Excellent — low growth disturbance risk | May be radiographically occult; diagnose clinically by physeal tenderness |
| II | Through physis + triangular metaphyseal fragment (Thurston-Holland sign) | Good — reproductive layer preserved with epiphysis | Most common SH type |
| III | Intra-articular; from joint surface through epiphysis → exits through physis | Usually favorable if vascularity preserved | Intra-articular fracture — requires anatomic reduction |
| IV | From articular surface → through epiphysis → entire physis → metaphysis | Significant growth disturbance risk | Precise reduction essential; often requires ORIF |
| V | Crush/compression injury to physis — often missed acutely | Poor — high risk of premature growth arrest | May look like a normal X-ray; diagnosed retrospectively after growth arrest |
In children, a physeal fracture should be assumed until proven otherwise — children rarely get sprains. — Miller's Review of Orthopaedics, 9th Ed.
Complications of Growth Plate Injury
| Complication | Mechanism | Management |
|---|---|---|
| Leg length discrepancy (LLD) | Complete physeal arrest → affected bone stops growing | Contralateral epiphysiodesis to equalize |
| Angular deformity | Partial physeal arrest (bony bar/bridge) → asymmetric growth | If <50% of physis involved and ≥2 years of growth remain: physeal bar resection + fat interposition; if >50%: complete the arrest + contralateral epiphysiodesis |
| Avascular necrosis | Disruption of epiphyseal blood supply (especially SH III/IV) | Depends on location; femoral head most vulnerable |
Fixation principle: If hardware must cross the physis, use only smooth K-wires — never threaded screws across an open plate. — Schwartz's Principles of Surgery, 11th Ed.
Sources: Histology: A Text and Atlas (Eroschenko) | Robbins, Cotran & Kumar Pathologic Basis of Disease | Schwartz's Principles of Surgery 11e | Tintinalli's Emergency Medicine | Miller's Review of Orthopaedics 9e | THIEME Atlas of Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.