Scoliosis Anaesthesia considerations Preoperative evaluation Intraoperative management Post op management Full long answer Also explain me in detail about the pathophysiological changesin scoliosis, specially respiratory changes,for understanding purpose Al
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
scoliosis anaesthesia management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching the Web
scoliosis anaesthesia preoperative intraoperative postoperative management respiratory pathophysiology
I now have comprehensive information from Miller's Anesthesia, Bailey and Love's Surgery, Campbell's Operative Orthopaedics, and web sources. I have everything needed to write a thorough, well-structured answer. Let me now compose the full detailed response.
Scoliosis: Anaesthesia Considerations - Complete Guide
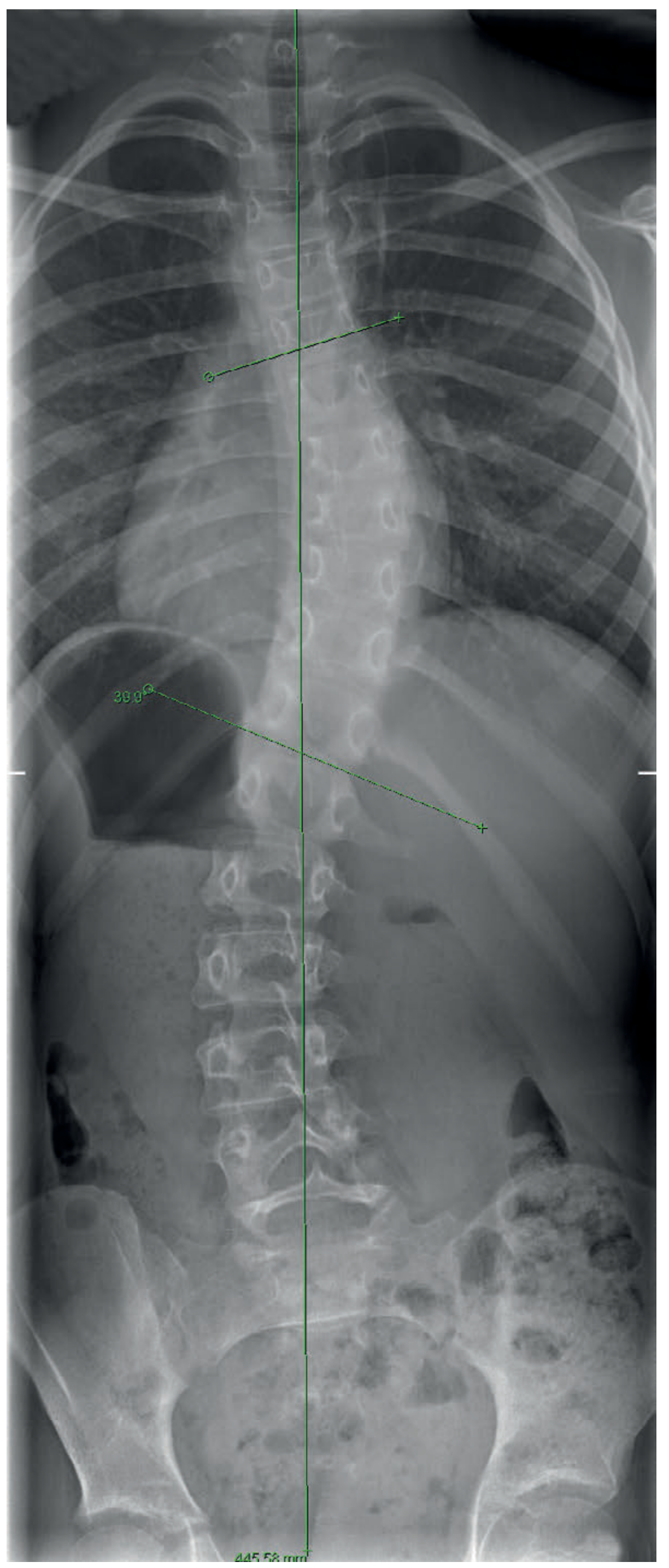
The Cobb Angle X-ray (Scoliosis Severity Measurement)
PART 1: PATHOPHYSIOLOGY OF SCOLIOSIS
Definition and Anatomy
Scoliosis is a three-dimensional spinal deformity - not just a simple lateral curve. It involves:
- Lateral curvature in the coronal plane (the obvious deformity)
- Vertebral rotation (creates the characteristic "rib hump" on forward flexion)
- Sagittal profile changes (loss of normal kyphosis/lordosis)
The Cobb angle is the radiological measurement on standing PA spine X-ray that defines severity and guides treatment:
- < 20° → observation only
- 25-40° → consider bracing
-
40-50° → surgical correction indicated
Aetiology: Idiopathic (70-80%), neuromuscular, congenital, syndromic.
Pathophysiological Changes
1. RESPIRATORY CHANGES (Detailed)
This is the most clinically important system affected. Understanding the mechanism is essential for anaesthetic planning.
A. Mechanical Distortion of the Thoracic Cage
The rotational component of scoliosis physically distorts the rib cage. As the vertebrae rotate around the axis of the curve:
- Ribs on the convex side are pushed posteriorly → create the rib hump → limited excursion
- Ribs on the concave side are crowded anteriorly → reduced intercostal space → limited expansion
- The result is a deformed, rigid thoracic cage that cannot expand normally
This creates mechanical restriction of chest wall movement - the fundamental driver of all pulmonary dysfunction.
B. Restrictive Lung Disease (Primary Mechanism)
The chest wall distortion leads to classic restrictive lung disease:
| Parameter | Effect in Scoliosis |
|---|---|
| Total Lung Capacity (TLC) | Reduced |
| Vital Capacity (VC) | Reduced (proportional to Cobb angle) |
| Functional Residual Capacity (FRC) | Reduced |
| Residual Volume (RV) | Relatively preserved or mildly reduced |
| FEV1/FVC ratio | Normal or slightly elevated (unlike obstructive) |
Key point: VC falls by approximately 20% for every 10° increase in Cobb angle above 65°. A Cobb angle > 100° is associated with severe respiratory failure.
Forced vital capacity (FVC) > 50% of normal = reduces risk of pulmonary complications. FVC < 35% indicates severe compromise (associated with cardiomyopathy in neuromuscular scoliosis - relative contraindication to surgery).
C. Ventilation-Perfusion (V/Q) Mismatch
This is the next step in the cascade:
- The compressed concave lung is small and poorly ventilated but may receive disproportionate blood flow → increased shunt (perfusion without ventilation)
- The convex lung is over-distended → increased dead space (ventilation without perfusion)
- Net result: V/Q mismatch → increased alveolar-arterial (A-a) oxygen gradient → hypoxaemia
This explains why even patients who appear mildly symptomatic may have significant hypoxaemia, especially during exercise or when supine (important for anaesthetic planning).
D. Alveolar Hypoventilation
In severe curves:
- The work of breathing increases substantially because of chest wall rigidity
- Respiratory muscles work at mechanically disadvantaged positions
- In neuromuscular scoliosis, the underlying muscle weakness adds to this
- Result: chronic alveolar hypoventilation → CO₂ retention → hypercapnia
- Hypercapnia → respiratory acidosis → compensatory metabolic alkalosis
This explains why some patients with severe scoliosis have a rightward shift of their CO₂ dissociation curve and blunted hypercapnic response - they have adapted to chronically elevated PaCO₂.
E. Pulmonary Hypertension (Cascade to Right Heart Failure)
This is the critical downstream consequence:
Mechanism:
- Chronic hypoxia → hypoxic pulmonary vasoconstriction (HPV) (Euler-Liljestrand reflex) → widespread vasoconstriction in poorly ventilated lung regions
- V/Q mismatch perpetuates hypoxia → sustained HPV
- Sustained HPV → structural changes in pulmonary vasculature → fixed pulmonary hypertension
- Pulmonary hypertension → increased right ventricular afterload → right ventricular hypertrophy (RVH)
- RVH → eventual right ventricular failure (Cor Pulmonale)
Additionally, the physical compression of pulmonary vasculature by the distorted thoracic cage directly elevates pulmonary vascular resistance.
Clinical cascade in severe scoliosis:
Chest wall deformity → Restriction → Hypoventilation → Hypoxia + Hypercapnia → HPV → Pulmonary HTN → Cor Pulmonale → Right Heart Failure
F. Reduced Lung Development (Early-Onset Scoliosis)
Most lung alveolar development occurs in the first 8 years of life. Early-onset scoliosis (< 10 years) physically restricts lung growth during this critical period, resulting in:
- Fewer alveoli (reduced alveolar count - "hypoplastic lung")
- Permanently reduced lung volumes even after surgical correction
- This is why early management (casting, growing rods) aims to preserve growth before fusion
2. CARDIOVASCULAR CHANGES
- Right ventricular hypertrophy secondary to pulmonary hypertension
- Right ventricular dysfunction/failure (cor pulmonale) in severe/chronic cases
- The mechanical rotation of the spine also displaces the heart and great vessels (mediastinal shift)
- In neuromuscular scoliosis (Duchenne MD, Friedreich's ataxia): cardiomyopathy is a co-existing finding
- Autonomic dysfunction (in some neuromuscular disorders) → haemodynamic instability under anaesthesia
3. NEUROLOGICAL CHANGES
- Risk of spinal cord injury from the deformity itself or from corrective surgery (stretch/ischemia)
- Syringomyelia may be present (especially in congenital scoliosis - mandates MRI pre-operatively)
- Neuropathic pain in some adults with degenerative scoliosis
- In neuromuscular scoliosis: underlying neurological disease (Cerebral palsy, DMD, SMA, etc.)
PART 2: PREOPERATIVE EVALUATION
Goals of Preoperative Assessment
The fundamental aim is to quantify end-organ dysfunction (respiratory, cardiac, neurological) and optimise the patient before a major, blood-loss-prone, prone-position surgery.
Detailed History
- Type and aetiology of scoliosis (idiopathic vs neuromuscular vs congenital vs syndromic)
- Age of onset - earlier onset = more likely severe pulmonary restriction
- Cobb angle - severity of curve
- Functional status: exercise tolerance, dyspnoea on exertion, oxygen requirement, nocturnal symptoms (nocturnal hypoventilation is common)
- Cough effectiveness - particularly in neuromuscular scoliosis (risk of postoperative secretion retention)
- Swallowing and aspiration risk (in cerebral palsy, SMA)
- Cardiac symptoms: palpitations (cardiomyopathy), syncope, ankle oedema (cor pulmonale)
- Previous anaesthetics: complications, difficult airway, malignant hyperthermia history
- Current medications: anticonvulsants (alter anaesthetic drug requirements and IONM signals), steroids, cardiac medications
Physical Examination
- Airway assessment - cervical spine mobility may be limited; some syndromic scoliosis (Marfan's, Down syndrome) may be at risk for atlantoaxial instability
- Chest wall inspection - rib hump, asymmetry, respiratory rate, use of accessory muscles
- Auscultation - areas of reduced air entry, added sounds
- Cardiovascular - JVP, peripheral oedema, murmurs (RV heave in pulmonary HTN)
- Neurological baseline - document ALL pre-existing neurological deficits (medicolegally critical, as any deficit found postoperatively must be distinguished from a pre-existing one)
- Nutritional status - in neuromuscular patients; poor nutrition = increased surgical risk and poor wound healing
Investigations
Respiratory Investigations
| Investigation | Significance |
|---|---|
| Pulmonary Function Tests (PFTs/Spirometry) | Most important. FVC, FEV1, FEV1/FVC. FVC > 50% predicted = acceptable risk. FVC < 35% = high risk / relative contraindication |
| Arterial Blood Gas (ABG) | Baseline PaO₂, PaCO₂, pH. Hypercapnia at rest = severe disease, indicates need for postoperative ventilation |
| Chest X-ray | Lung fields, cardiac size, mediastinal position |
| CT Chest | When needed for surgical planning or to assess pulmonary parenchyma |
| Sleep study (polysomnography) | If nocturnal desaturation suspected - guides need for preoperative nocturnal NIV/BiPAP |
| 6-minute walk test | Functional exercise tolerance |
Cardiac Investigations
| Investigation | Purpose |
|---|---|
| ECG | RVH pattern (R in V1, right axis deviation), arrhythmias (especially in DMD/Friedreich's) |
| Transthoracic Echocardiography (TTE) | Assess severity of pulmonary hypertension (TR jet velocity), RV function, LV function, LVEF, pericardial effusion |
| Cardiac MRI | If cardiomyopathy suspected (DMD) |
Haematological and Biochemical Investigations
- Full blood count - baseline haemoglobin (blood loss can be massive)
- Coagulation profile (PT, aPTT, INR, fibrinogen) - needed for blood conservation planning
- Group & Screen / Cross-match - for anticipated major blood loss (typically 2-4 units for posterior spinal fusion)
- Electrolytes, renal function - baseline; relevant if antifibrinolytics (TXA) to be used
- Liver function tests - if on hepatic metabolised medications
- HbA1c - if diabetic (relevant for wound healing)
Imaging
- Standing PA and lateral whole-spine X-ray - Cobb angle measurement
- MRI spine - rule out syringomyelia, tethered cord, spinal cord compression (especially in congenital/neuromuscular cases)
Preoperative Optimisation
- Chest physiotherapy and incentive spirometry (especially in neuromuscular scoliosis)
- Nocturnal NIV/BiPAP if nocturnal hypoventilation is present - ideally started weeks before surgery
- Chest infections must be cleared - surgery should be delayed
- Nutritional supplementation if malnourished (PEG feeding in severe neuromuscular cases)
- Cardiac optimisation - treat cor pulmonale, optimise heart failure
- Blood conservation strategies: Preoperative autologous donation (PAD), erythropoietin, iron therapy (oral or IV) to maximise haemoglobin
- Preoperative TIVA assessment - if neuromuscular disease is present (risk of malignant hyperthermia-like reactions with volatiles)
- Discussion with neurophysiology team - baseline neurological recording for IONM
- Detailed consent - including risk of neurological injury (0.5-7.5%), visual loss, massive transfusion, re-intubation, ICU admission
PART 3: INTRAOPERATIVE MANAGEMENT
Positioning
Scoliosis surgery is performed in the prone position using a specialised frame (Wilson frame or Jackson table):
- All pressure points carefully padded (knees, ankles, elbows, forehead)
- Eyes must be protected - direct pressure on the eye is strictly prohibited (risk of CRAO and perioperative visual loss)
- Head in neutral position - no extreme flexion, extension, or rotation (risk of vertebral artery injury and vision loss)
- Abdomen must hang free - reduces epidural venous pressure and reduces blood loss
- Arms positioned carefully - shoulder at < 90° abduction to prevent brachial plexus stretch
Anaesthetic Technique
Induction
- Standard IV induction with propofol + opioid (fentanyl/remifentanil)
- Avoid succinylcholine in neuromuscular scoliosis (risk of hyperkalaemic cardiac arrest, malignant hyperthermia trigger)
- Use rocuronium (reversible with sugammadex) as the neuromuscular blocker for intubation
- Standard ETT (not LMA) mandatory - surgery is long and in prone position
- Fibreoptic intubation if difficult airway anticipated (syndromic patients, limited neck movement)
- For anterior thoracic approaches: double-lumen ETT or bronchial blocker for lung isolation
Maintenance
TIVA (Total Intravenous Anaesthesia) is the technique of choice when IONM is required:
- Propofol + Remifentanil infusion (TCI) - minimal effect on SSEP/MEP signals
- Volatile agents (especially halothane/isoflurane/desflurane) significantly suppress SSEP and MEP signals in a dose-dependent manner - particularly dangerous with MEPs
- If TIVA is not available: low-dose volatile (< 0.5 MAC) may be acceptable but is suboptimal
- Nitrous oxide should be avoided - suppresses MEPs and increases the risk of venous air embolism
- Ketamine (subanesthetic doses) and dexmedetomidine are useful adjuncts - preserve IONM signals and provide analgesia/sedation
Neuromuscular blockers during surgery:
- Should be avoided during IONM as they suppress MEPs
- Single-dose for intubation only, then allow full reversal
- Monitor NMB with a train-of-four before IONM readings
Monitoring
Standard Monitoring
- ECG, SpO₂, EtCO₂, temperature (core - nasopharyngeal or oesophageal)
- Invasive arterial line (A-line) - mandatory for continuous BP monitoring, frequent ABG sampling, blood conservation
- Central venous access - for fluid management, CVP monitoring, vasopressor infusion
- Urinary catheter - hourly urine output
- Warm air blanket / fluid warmer - normothermia essential (hypothermia suppresses IONM, exacerbates coagulopathy)
Intraoperative Neurophysiological Monitoring (IONM)
This is one of the most important aspects of scoliosis anaesthesia.
Why is IONM needed?
Surgical distraction, derotation, or instrumentation can compress or stretch the spinal cord, causing ischaemia. Neurological injury (paraplegia/paraparesis) occurs in 0.5-7.5% of cases. IONM detects this in real time before permanent damage occurs.
Modalities:
| Modality | What it monitors | Pathway | Signal characteristics |
|---|---|---|---|
| SSEP (Somatosensory Evoked Potentials) | Sensory pathway | Dorsal columns | Stimulate peripheral nerves (ulnar, median, posterior tibial); record at cortex |
| MEP (Motor Evoked Potentials) | Motor pathway | Corticospinal tract | Stimulate motor cortex; record from distal muscle groups |
| D-waves | Corticospinal axons directly | Corticospinal tract | Epidural recording electrode; resistant to anaesthetic suppression |
| EMG (triggered) | Nerve root integrity | - | Confirms correct pedicle screw placement |
SSEP Alarm Criteria: >50% amplitude decrease or >10% latency increase is significant
MEP Alarm Criteria: Any consistent decrease in amplitude or loss of response
Anaesthetic effects on IONM:
| Agent | Effect on SSEP | Effect on MEP |
|---|---|---|
| Propofol | Mild suppression | Mild suppression |
| Volatile agents | Dose-dependent suppression | More severe suppression |
| Nitrous oxide | Moderate suppression | Marked suppression |
| Ketamine | Preserves / enhances | Preserves |
| Dexmedetomidine | Minimal | Minimal |
| Opioids/benzodiazepines | Minimal | Minimal |
| Neuromuscular blockers | No effect | Abolishes muscle MEPs |
If IONM changes occur (sudden loss/significant change in signals):
- Immediately communicate with surgeon and neurophysiologist
- Implement predetermined checklist:
- Optimise mean arterial pressure (MAP ≥ 65-70 mmHg; consider higher target ≥ 80 mmHg)
- Correct anaemia - transfuse to Hb > 8-10 g/dL
- Correct temperature, pH, PaCO₂ abnormalities
- Lighten the anaesthetic plane (check TIVA doses)
- Ensure no NMB in effect
- Wake-up test (Stagnara test) if IONM changes persist despite optimisation:
- Lighten anaesthesia
- Ask patient to move hands (control) then feet (test)
- Inability to move feet = cord injury → immediate surgical reversal (remove instrumentation, decompress)
- Risks: inadvertent extubation, dislodgement of instrumentation, air embolism on deep inspiration, patient awareness
Blood Conservation and Haemostasis
Scoliosis surgery is a major blood loss procedure (typically 20-50% of estimated blood volume).
Strategies:
-
Antifibrinolytics:
- Tranexamic acid (TXA) - drug of choice; more effective than EACA and aprotinin in reducing total blood loss, intraoperative blood loss, and transfusion requirements. Administer as a loading dose + infusion.
- EACA (epsilon-aminocaproic acid) - alternative when TXA is contraindicated
- Avoid in patients with thromboembolic history, coronary stents, or significant renal impairment
-
Cell salvage (intraoperative autologous blood recovery) - blood from the surgical field is processed and re-infused
-
Deliberate controlled hypotension:
- Reduces blood loss by lowering perfusion pressure at the surgical site
- Target MAP 55-65 mmHg (used judiciously)
- Caution: must not be used during IONM monitoring periods (hypotension compromises spinal cord perfusion); avoid in elderly, cardiovascular disease, prior stroke; avoid in patients at risk for perioperative visual loss (ION)
- Mean arterial pressure must be maintained ≥ 65-70 mmHg to protect the spinal cord
-
Preoperative autologous donation (PAD) - patient donates their own blood weeks before surgery for re-infusion intraoperatively
-
Positioning - free-hanging abdomen reduces IVC compression and epidural venous engorgement → less blood loss
-
Normovolaemia - must be maintained throughout; hypovolaemia in prone position can rapidly cause cardiovascular collapse; patients with neuromuscular scoliosis are 3 times more likely to have intraoperative cardiac arrests than idiopathic scoliosis patients
Transfusion Trigger:
- Hb < 7-8 g/dL in otherwise healthy patients
- Hb < 10 g/dL in patients with pulmonary hypertension or cardiac disease (they tolerate anaemia poorly)
- Guide transfusion with TEG/ROTEM for coagulation status
Fluid Management
- Balanced crystalloids (Hartmann's/PlasmaLyte) as maintenance
- Colloids - albumin/Gelofusine alongside crystalloids when blood loss is substantial (reduces risk of perioperative visual loss)
- Avoid excessive crystalloid - worsens tissue oedema, can impair IONM signals
- Consider vasopressors (noradrenaline/vasopressin) to maintain MAP without fluid overloading
Temperature Management
- Active warming throughout (forced air warming blanket, warmed IV fluids)
- Hypothermia depresses IONM signals, causes coagulopathy, increases infection risk, prolongs NMB
- Target normothermia (core temperature 36-37°C)
Venous Air Embolism (VAE)
- Risk is significant during wide paravertebral dissection and vertebral distraction
- Detection: fall in EtCO₂, hypotension, mill-wheel murmur on precordial doppler
- Management: pack wound, flood field with saline, stop N₂O if in use, left lateral decubitus + Trendelenburg if possible (difficult in prone - have plan ready)
PART 4: POSTOPERATIVE MANAGEMENT
Extubation Criteria
The decision to extubate vs. elective postoperative ventilation is critical:
Extubate in the operating room if:
- Preoperative FVC > 50% predicted
- Short surgery with minimal blood loss
- Warm, haemodynamically stable
- Reversible NMB confirmed (TOF ratio > 0.9)
- Good cough reflex
- No significant intraoperative complications
Elective postoperative ventilation (ICU/HDU) if any of:
- Preoperative FVC < 35% predicted
- Neuromuscular scoliosis with baseline respiratory muscle weakness
- Intraoperative blood loss > 33% of total blood volume
- Massive transfusion
- Prolonged surgery (> 6 hours)
- Multiple vertebral levels fused (> 6 levels)
- Significant intraoperative haemodynamic instability
- Low body weight / severe malnutrition
- Baseline hypercapnia (PaCO₂ > 45 mmHg preoperatively)
Respiratory Management
- Supplemental oxygen in all patients postoperatively
- Incentive spirometry - early, to prevent atelectasis
- Chest physiotherapy - particularly important in neuromuscular cases
- Non-Invasive Ventilation (NIV/BiPAP) - preferred over re-intubation in patients who fail to maintain ventilation; particularly useful in DMD, SMA
- Cough assist devices (mechanical insufflation-exsufflation) - in patients with neuromuscular weakness and ineffective cough
- Anticipate significant postoperative atelectasis - it will not improve immediately after scoliosis correction; in fact, may worsen transiently
- Early and successful weaning from ventilator should be prioritised to reduce risk of ventilator-associated pneumonia (VAP) and tracheal stenosis
Pain Management
Scoliosis surgery involves a long posterior incision with extensive paravertebral muscle dissection - it is extremely painful.
Multimodal analgesia approach:
| Analgesic | Role |
|---|---|
| IV opioids (morphine/oxycodone PCA) | Mainstay of early postoperative analgesia |
| Paracetamol (IV/oral) | Regular, opioid-sparing |
| NSAIDs (e.g., ketorolac) | Opioid-sparing; caution in renal impairment and bone fusion (theoretical concern about impaired fusion) |
| Ketamine (low-dose IV infusion) | Reduces opioid requirements, prevents central sensitisation |
| Dexmedetomidine | Sedation + analgesia with opioid-sparing |
| Gabapentin/pregabalin | Neuropathic pain component |
| Intrathecal morphine | Administered before skin closure; provides excellent 12-24 hr analgesia |
| Wound infiltration / ERAS | Local anaesthetic infiltration at skin closure |
| Epidural | Less commonly used due to posterior spinal surgery |
ERAS (Enhanced Recovery After Surgery) principles now incorporated into scoliosis protocols: optimise preoperative nutrition, early mobilisation, multimodal analgesia, minimise opioid use.
Haemodynamic Monitoring
- Continuous ECG, SpO₂, non-invasive BP postoperatively
- Invasive arterial line maintained until haemodynamically stable
- In unstable patients: invasive BP, CVP, hourly urine output monitoring
- Watch for postoperative haemorrhage - surgical wound drainage, falling Hb, haemodynamic instability
- Neurological checks - regular lower limb neurological assessment (can patient move toes/feet?)
Neurological Assessment
- Immediate postoperative neurological exam - assess lower limb power, sensation; compare with preoperative baseline
- Any new neurological deficit = surgical emergency → urgent imaging and possible return to theatre
- Wake-up test (if not done intraoperatively) can be performed in recovery
Fluid and Renal Management
- Maintain adequate urine output (> 0.5 mL/kg/hr)
- Avoid hypovolaemia (risk of spinal cord ischaemia persists postoperatively)
- Monitor for acute kidney injury - especially if antifibrinolytics used, prolonged hypotension, contrast media
ICU/HDU Admission Criteria
ICU admission is indicated in:
- Neuromuscular scoliosis (particularly DMD, SMA)
- FVC < 35% preoperatively
- Prolonged surgery or massive transfusion
- Intraoperative complications (haemodynamic instability, IONM changes)
- Baseline hypercapnia
ICU admission rates in scoliosis surgery: ~15-25%.
Specific Complications to Watch For
| Complication | Detection | Management |
|---|---|---|
| Neurological deficit | Neurological exam, IONM | Emergency surgical exploration |
| Perioperative Visual Loss (POVL) | Visual assessment postoperatively | Avoid/correct: anaemia, hypotension, direct eye pressure, prolonged prone position |
| Massive haemorrhage | Drain output, Hb, haemodynamics | Blood products, return to theatre |
| Pulmonary atelectasis/pneumonia | SpO₂, CXR | Physiotherapy, NIV, antibiotics |
| Deep wound infection | Wound inspection, fever, CRP | IV antibiotics, surgical washout |
| Venous thromboembolism (DVT/PE) | Clinical, CTPA | LMWH prophylaxis, treatment anticoagulation |
| Implant failure | Pain, imaging | Revision surgery |
| Junctional kyphosis | Late finding | Possible revision |
SUMMARY FRAMEWORK
SCOLIOSIS ANAESTHESIA: THREE PILLARS
1. RESPIRATORY 2. BLOOD 3. SPINAL CORD
Assessment (PFT, ABG) Conservation (TXA, Protection (IONM,
↓ cell salvage) SSEP + MEP)
Optimise pre-op ↓ ↓
(chest physio, NIV) Normovolaemia TIVA (propofol +
↓ Controlled remifentanil)
Post-op ventilation plan hypotension ↓
(extubate vs ICU) (avoid if cord risk) Wake-up test
if needed
Key Points to Remember
- Scoliosis surgery carries 0.5-7.5% risk of neurological injury - IONM is non-negotiable
- TIVA (propofol + remifentanil) is the gold standard for maintenance when IONM is used - volatile agents suppress MEPs
- Succinylcholine is contraindicated in neuromuscular scoliosis - risk of hyperkalaemic arrest and malignant hyperthermia
- TXA is the most effective antifibrinolytic - reduces blood loss and transfusion significantly
- Postoperative respiratory failure is the most common serious postoperative complication, especially in neuromuscular scoliosis
- Patients with neuromuscular scoliosis are 3x more likely to suffer intraoperative cardiac arrest compared to idiopathic scoliosis patients
- The "rib hump" is caused by vertebral rotation - not just lateral curvature
- Early-onset scoliosis is more devastating because it restricts alveolar development during childhood - a permanent effect
- Cor pulmonale is the end-stage of untreated severe scoliosis respiratory disease - echocardiography is mandatory before surgery
Sources: Miller's Anesthesia 10e (p. 9237-9242), Bailey & Love's Short Practice of Surgery 28e (p. 651), Campbell's Operative Orthopaedics 15e (2026)
This is a shared conversation. Sign in to Orris to start your own chat.