Necrosis
Reading File
Finding Sources
Searching PubMed
necrosis cell death mechanisms types
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a thorough answer. Here is the full response:
Necrosis
Necrosis is a pathologic form of cell death resulting from severe, irreversible injury. It is distinguished from apoptosis (programmed cell death) by membrane destruction, enzymatic digestion of the cell, leakage of intracellular contents, and a local inflammatory reaction.
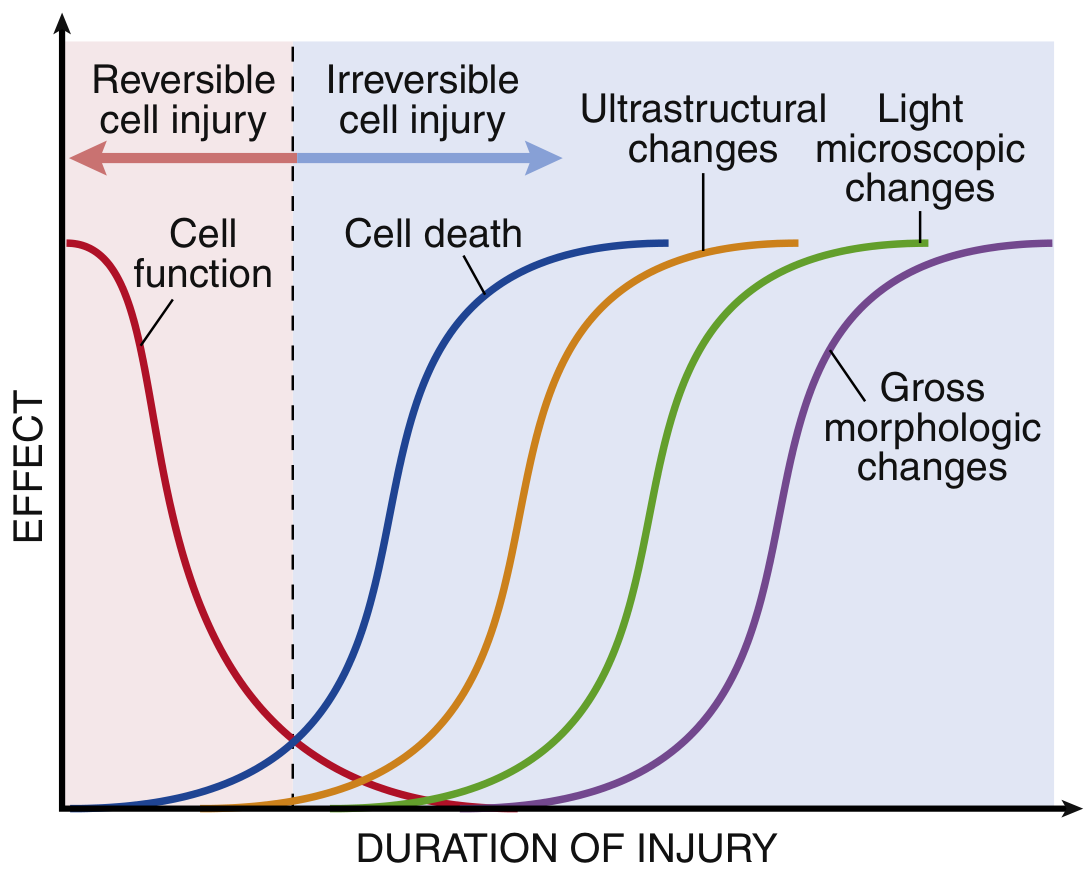
Note that cell function is lost well before actual cell death, and morphologic changes (ultrastructural, then light microscopic, then gross) appear progressively later. - Robbins & Kumar Basic Pathology
Definition and Causes
Necrosis results from severe, irreparable damage to cellular components. Major causes include:
- Ischemia (loss of oxygen supply - most common)
- Microbial toxins and infections
- Burns, chemical, and physical injury
- Active proteases leaking from cells (e.g., acute pancreatitis)
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
Pathogenesis - What Actually Happens
Two phenomena consistently define the point of no return (reversible → irreversible injury):
- Irreversible mitochondrial dysfunction - failure of oxidative phosphorylation and ATP generation even after the original insult resolves
- Profound membrane dysfunction - lysosomal membrane rupture releases enzymes into the cytoplasm, causing enzymatic dissolution of the cell
When plasma membrane integrity is lost, intracellular contents leak into the extracellular space and trigger the host inflammatory response. Released molecules - called damage-associated molecular patterns (DAMPs) - include:
- ATP (from damaged mitochondria)
- Uric acid (DNA breakdown product)
- Other normally intracellular molecules
These are recognized by macrophage receptors, triggering phagocytosis and cytokine release, which amplifies the inflammatory response and eventually clears necrotic debris.
Clinical Relevance of Membrane Leakage
Necrosis-associated leakage of intracellular proteins into the circulation is the basis for widely used biomarkers:
- Cardiac troponins - detectable in blood as early as 2 hours after myocardial cell necrosis (before histologic evidence appears)
- Transaminases (ALT/AST) - hepatocyte necrosis
- Alkaline phosphatase - bile duct epithelium necrosis
(Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 55)
Morphology of Necrosis
Cytoplasmic Changes
| Feature | Mechanism |
|---|---|
| Increased eosinophilia (pink on H&E) | Binding of eosin to denatured proteins + loss of basophilic RNA |
| Glassy, homogeneous appearance | Loss of glycogen particles |
| Vacuolated, "moth-eaten" cytoplasm | Enzymatic digestion of organelles |
| Myelin figures (phospholipid whorls) | Replacement of dead cells |
Nuclear Changes (three patterns)
- Pyknosis - nuclear shrinkage and increased basophilia; DNA condenses into a dark, shrunken mass
- Karyorrhexis - fragmentation of the pyknotic nucleus
- Karyolysis - fading basophilia from DNase-mediated digestion of DNA; complete nuclear dissolution within 1-2 days
Ultrastructural Changes (EM)
- Discontinuities in plasma and organelle membranes
- Marked mitochondrial dilation with large amorphous intramitochondrial densities
- Disruption of lysosomes
- Abundant intracytoplasmic myelin figures
(Robbins & Kumar Basic Pathology)
Patterns of Tissue Necrosis
When large numbers of cells die, the tissue or organ is said to be necrotic. Six distinct morphologic patterns are recognized:
1. Coagulative Necrosis
- Hallmark: Architecture of dead tissue is preserved for days
- Firm texture; injury denatures structural proteins AND enzymes, blocking proteolysis
- Eosinophilic cells with indistinct nuclei persist for days-weeks
- Eventually cleared by leukocyte lysosomal enzymes and phagocytosis
- Cause: Ischemia in almost all organs (except the brain)
- A localized area = infarct
2. Liquefactive Necrosis
- Hallmark: Dead cells are digested, tissue transforms into a viscous liquid
- Seen in: focal bacterial or fungal infections (leukocytes release degradative enzymes); pus = creamy yellow necrotic material
- Exception: CNS hypoxic death manifests as liquefactive necrosis (for unknown reasons)
3. Gangrenous Necrosis
- Not a distinct cell death pattern - a clinical term
- Applied to a limb (usually lower leg) that has lost blood supply and undergone coagulative necrosis across multiple tissue planes
- Wet gangrene: bacterial superinfection adds liquefactive necrosis
4. Caseous Necrosis
- Classic association: Tuberculosis (and other mycobacterial infections)
- "Caseous" = cheeselike, friable white gross appearance
- Microscopy: structureless, fragmented/lysed cells in amorphous granular debris, enclosed within epithelioid cell granuloma
5. Fat Necrosis
- Focal fat destruction from activated pancreatic lipases leaking into peritoneum (acute pancreatitis)
- Pancreatic enzymes liquefy fat cell membranes → triglycerides split by lipases → fatty acids combine with calcium → chalky-white areas (saponification)
- Histology: shadowy necrotic fat cell outlines + basophilic calcium deposits + inflammation
6. Fibrinoid Necrosis
- Special form of vascular damage in immune reactions (antigen-antibody complexes deposited in artery walls)
- Immune complexes + leaked plasma proteins → bright pink, amorphous "fibrin-like" appearance on H&E
- Seen in vasculitis, malignant hypertension, polyarteritis nodosa
(Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 54-56)
Necrosis vs. Apoptosis - Key Differences
| Feature | Necrosis | Apoptosis |
|---|---|---|
| Cause | Pathologic (severe injury) | Physiologic or pathologic |
| Membrane integrity | Destroyed | Maintained (initially) |
| Cell size | Swelling | Shrinkage |
| Nuclear change | Pyknosis/karyorrhexis/karyolysis | Chromatin condensation, fragmentation |
| Inflammation | Yes - prominent | No - absent |
| Cell fragments | Amorphous debris | Apoptotic bodies |
| Mechanism | Passive enzymatic digestion | Active, regulated caspase activation |
Fate of Necrotic Cells
In a living patient, necrotic cells and debris are eventually cleared by enzymatic digestion and leukocyte phagocytosis. If debris is not promptly cleared, it becomes a nidus for deposition of calcium salts - a process called dystrophic calcification.
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
This is a shared conversation. Sign in to Orris to start your own chat.