cushings syndrome k sembulingam edition 10 physiology book answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching the Web
K Sembulingam physiology 10th edition Cushing syndrome adrenal cortex
I now have comprehensive content from the top physiology textbooks (Guyton & Hall and Ganong's) that directly mirrors what Sembulingam covers in Chapter 70 (Adrenal Cortex). K. Sembulingam's "Essentials of Medical Physiology" is not in the library, but the content below is drawn from Guyton & Hall and Ganong's - both standard references that cover identical concepts to Sembulingam. Here is the full answer:
Cushing Syndrome - Physiology (As per Standard Medical Physiology Textbooks)
Note: K. Sembulingam's Essentials of Medical Physiology (10th ed.) is not available in this library, but Cushing's syndrome is covered under Chapter 70 - Adrenal Cortex in Sembulingam. The content below is drawn from Guyton & Hall and Ganong's Review of Medical Physiology, which cover identical concepts and serve as the standard references for this topic.
Definition
Cushing syndrome is a complex clinical condition resulting from prolonged hypersecretion of glucocorticoids (mainly cortisol) by the adrenal cortex, or from prolonged exogenous glucocorticoid administration.
Causes / Etiology
| Type | Mechanism | ACTH Level |
|---|---|---|
| Cushing disease (most common) | ACTH-secreting pituitary adenoma → adrenal hyperplasia | High |
| Hypothalamic dysfunction | Excess CRH → excess ACTH | High |
| Ectopic ACTH syndrome | Tumor (e.g., lung carcinoma) secreting ACTH | High |
| Adrenal adenoma/carcinoma | Primary adrenal cortex overproduction | Low (suppressed by feedback) |
| Iatrogenic (exogenous) | Prolonged therapeutic glucocorticoid use (e.g., rheumatoid arthritis) | Low |
- Excess ACTH secretion (ACTH-dependent) is the most common cause overall.
- Primary adrenal overproduction accounts for about 20-25% of cases.
-
- Guyton & Hall, p. 958
Clinical Features / Signs and Symptoms
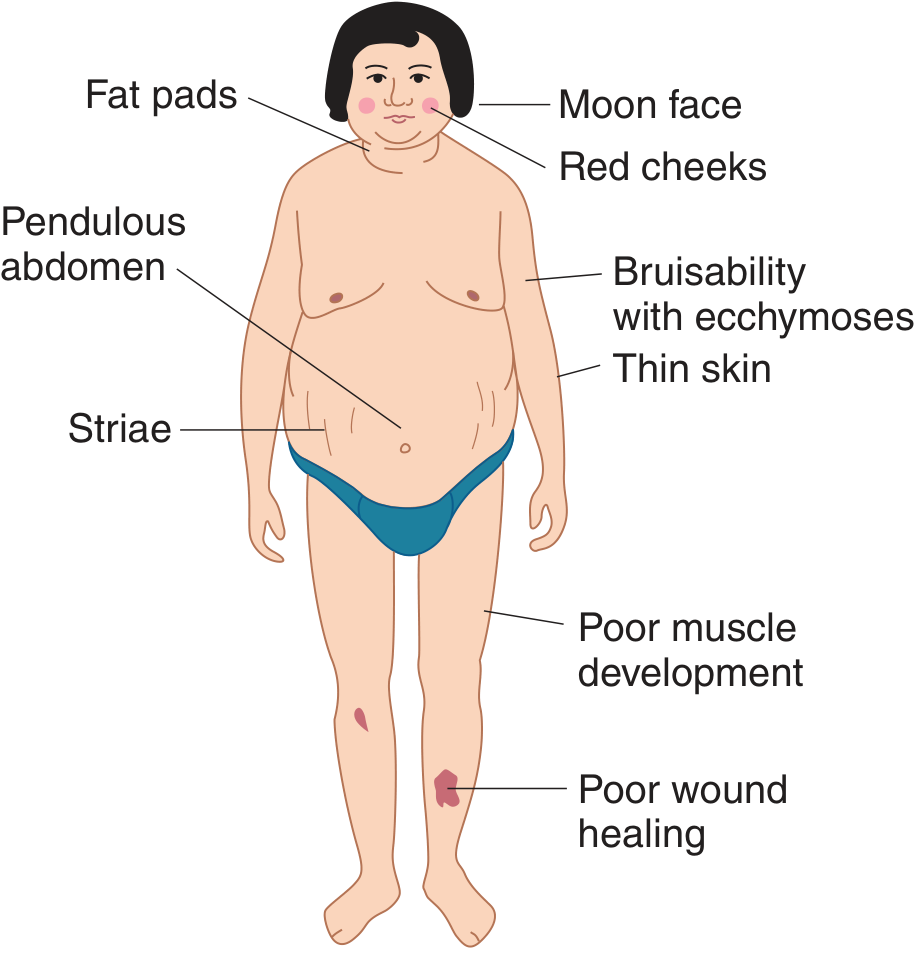
1. Fat Distribution Changes
- Central (truncal) obesity with fat mobilized from limbs toward the trunk and upper abdomen
- Buffalo hump - fat deposition over the upper back
- Moon face - rounded, plethoric, edematous appearance from fat deposition and salt/water retention
- Pendulous abdomen
- Thin, poorly developed extremities
2. Skin Changes
- Striae - reddish-purple stretch marks on the abdomen; the thin skin tears as subcutaneous fat expands
- Thin, fragile skin prone to easy bruising and ecchymoses
- Poor wound healing
- Acne and hirsutism (from excess adrenal androgens)
- Hair is thin and scraggly
3. Cardiovascular
- Hypertension in ~80-85% of patients
- Mechanisms: mineralocorticoid effect of excess cortisol, increased deoxycorticosterone secretion, increased angiotensinogen, direct glucocorticoid effect on blood vessels
4. Metabolic - Carbohydrate
- Hyperglycemia - blood glucose may reach 200 mg/dL after meals
- Caused by increased gluconeogenesis and decreased peripheral glucose utilization
- Insulin-resistant diabetes mellitus may develop (especially in genetically predisposed individuals)
- Hyperlipidemia and ketosis may accompany the diabetes
5. Metabolic - Protein
- Excess protein catabolism throughout the body (except liver and plasma proteins)
- Leads to:
- Muscle wasting and weakness (protein lost from muscles)
- Thin skin and subcutaneous tissues
- Diminished collagen in subcutaneous tissue (causes striae)
- Osteoporosis - decreased protein deposition in bones leads to vertebral collapse and fractures; glucocorticoids decrease bone formation and increase bone resorption
6. Immune System
- Suppression of the immune system due to loss of protein synthesis in lymphoid tissues
- Patients are highly susceptible to infections
7. Electrolytes
- Hypokalemia - from mineralocorticoid action of excess cortisol and elevated deoxycorticosterone
- Muscle weakness
- Mild metabolic alkalosis
8. Neuropsychiatric
- Acceleration of basic EEG rhythms
- Mental aberrations ranging from increased appetite, insomnia, euphoria to frank toxic psychoses
Dexamethasone Suppression Test (Differential Diagnosis)
| Test | Pituitary (Cushing Disease) | Primary Adrenal | Ectopic ACTH |
|---|---|---|---|
| Low-dose dexamethasone | No suppression | No suppression | No suppression |
| High-dose dexamethasone | Suppression (eventually) | No suppression | No suppression |
| ACTH level | High | Low/undetectable | Very High |
- The dexamethasone test is a first-step screening tool; some pituitary tumors may still respond to dexamethasone, and ectopic ACTH tumors are typically not responsive to feedback.
-
- Guyton & Hall, p. 958
Summary of Key Features (Sembulingam-style mnemonic)
"ABCDEFGH" of Cushing's:
- Adrenal hyperplasia / Androgens (hirsutism, acne)
- Buffalo hump
- Central obesity
- Diabetes (steroid-induced)
- Edema and hypertension
- Fragile skin (striae, bruising)
- Gluconeogenesis increased
- Hypokalemia, Hypertension, Hirsutism
Treatment
- Surgical removal of adrenal adenoma (if primary adrenal cause)
- Pituitary surgery or radiation for Cushing disease (ACTH-secreting pituitary tumor)
- Drugs that block steroidogenesis: metyrapone, ketoconazole, aminoglutethimide
- Drugs that inhibit ACTH secretion: serotonin antagonists, GABA-transaminase inhibitors
- Bilateral adrenalectomy (partial or total) as last resort, followed by steroid replacement
-
- Guyton & Hall, p. 959
Sources:
- Guyton and Hall Textbook of Medical Physiology (pp. 958-959) - Section: Hyperadrenalism - Cushing Syndrome
- Ganong's Review of Medical Physiology, 26th Ed. (pp. 354-355) - Section: Cushing Syndrome
This is a shared conversation. Sign in to Orris to start your own chat.