Explain aki in detail
Reading File
Finding Sources
Searching PubMed
"acute kidney injury"[MeSH Terms] AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a detailed explanation of AKI. Let me compile this into a thorough, well-organized response.
Acute Kidney Injury (AKI)
Definition
AKI is a clinical syndrome defined as a rapid decline in kidney function within approximately 1 week of an injurious stimulus. The current standard is the KDIGO (Kidney Disease: Improving Global Outcomes) definition, which requires any of the following:
- Serum creatinine rise ≥ 0.3 mg/dL within 48 hours, OR
- Serum creatinine rise ≥ 1.5× baseline within 7 days, OR
- Urine output < 0.5 mL/kg/hour for ≥ 6 hours
— Goldman-Cecil Medicine, 27th Edition
KDIGO Staging
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5–1.9× baseline OR ≥0.3 mg/dL increase | < 0.5 mL/kg/hr for 6–12 hrs |
| 2 | 2.0–2.9× baseline | < 0.5 mL/kg/hr for ≥12 hrs |
| 3 | ≥3.0× baseline OR ≥4.0 mg/dL OR initiation of RRT | < 0.3 mL/kg/hr for ≥24 hrs OR anuria ≥12 hrs |
Prior classification systems (RIFLE, AKIN) are still encountered; KDIGO represents the current consensus.
Epidemiology
- ~20–25% of all hospitalized adults have an elevated serum creatinine
- Up to 45% of ED admissions and 55–65% of ICU patients are affected
- Community-acquired AKI is far less common (<1% annual incidence)
- Prerenal azotemia accounts for 40% of hospital-acquired and 60–70% of community-acquired AKI cases
- Intrinsic AKI requiring dialysis has increased substantially over the past three decades
— Goldman-Cecil Medicine
Classification & Etiology
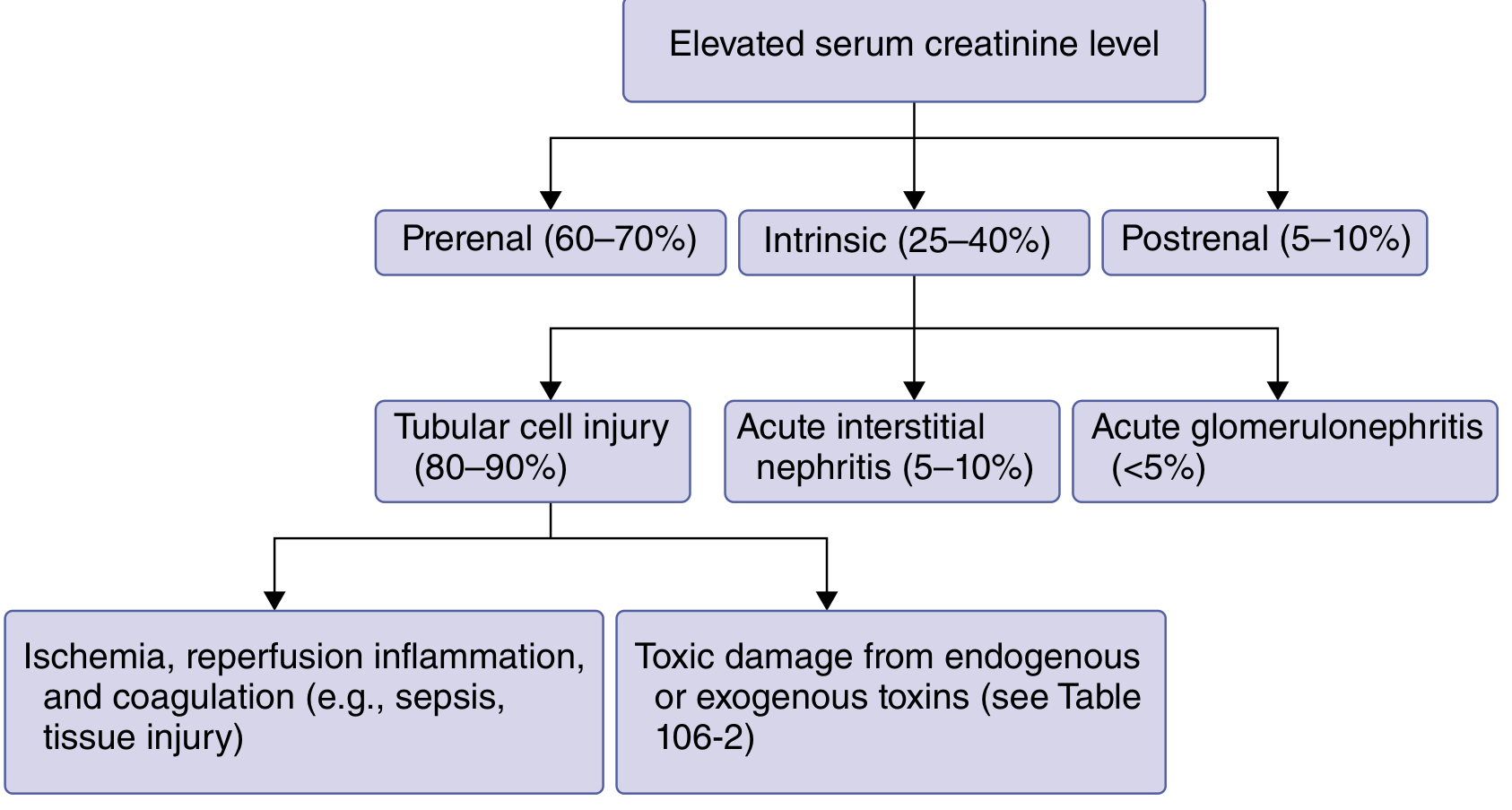
1. Prerenal AKI (60–70%)
Caused by renal hypoperfusion — kidney function is structurally intact but GFR falls due to inadequate perfusion pressure.
Mechanisms and causes:
| Mechanism | Example |
|---|---|
| True volume depletion | Hemorrhage, diarrhea, burns, diuretics, poor oral intake, fever |
| Decreased effective circulating volume | Heart failure, cirrhosis, hepatorenal syndrome |
| Systemic vasodilation/renal vasoconstriction | Sepsis, hepatorenal syndrome |
| Medications impairing renal autoregulation | NSAIDs, ACE inhibitors, ARBs, radiocontrast, cyclosporine |
| Large-vessel renal vascular disease | Renal artery thrombosis/embolism, renal artery stenosis |
Key feature: reversible within hours of restoring perfusion; urinary biomarkers of damage are NOT significantly elevated.
Labs: BUN:Cr ratio >20:1; FENa <1% (or FEurea <35% if on diuretics)
2. Intrinsic AKI (25–40%)
Structural damage to the kidney parenchyma — divided by primary site of injury:
| Subtype | Frequency | Key Causes |
|---|---|---|
| Acute Tubular Injury (ATI/ATN) | 80–90% of intrinsic | Ischemia/reperfusion, sepsis, nephrotoxins |
| Acute Interstitial Nephritis (AIN) | 5–10% | Antibiotics (penicillins, cephalosporins, sulfonamides), NSAIDs, PPIs, checkpoint inhibitors |
| Acute Glomerulonephritis | <5% | Vasculitis, IgA nephropathy, anti-GBM disease |
| Vascular | Rare | TTP/HUS, malignant hypertension, scleroderma, cholesterol emboli |
Common renal tubular toxins include: aminoglycosides, vancomycin, amphotericin B, cisplatin, radiocontrast agents, myoglobin/hemoglobin, uric acid crystals, cyclosporine/tacrolimus, methotrexate, ethylene glycol.
Labs: FENa >1% (but may be <1% in early sepsis, contrast nephropathy, GN); granular/muddy brown casts in urinalysis for ATN; eosinophiluria in AIN (unreliable); biomarkers markedly elevated.
3. Postrenal AKI (5–10%)
Caused by obstruction of urinary outflow. Should be suspected with oliguria (<450 mL/day) or anuria (<100 mL/day).
Common causes: prostatic hypertrophy (most common in older men), prostate/cervical/bladder cancer, retroperitoneal fibrosis, bilateral ureteric obstruction, urethral stricture.
Diagnosis: renal ultrasound (hydronephrosis), bladder catheterization.
Pathophysiology
Phases of ATI/ATN
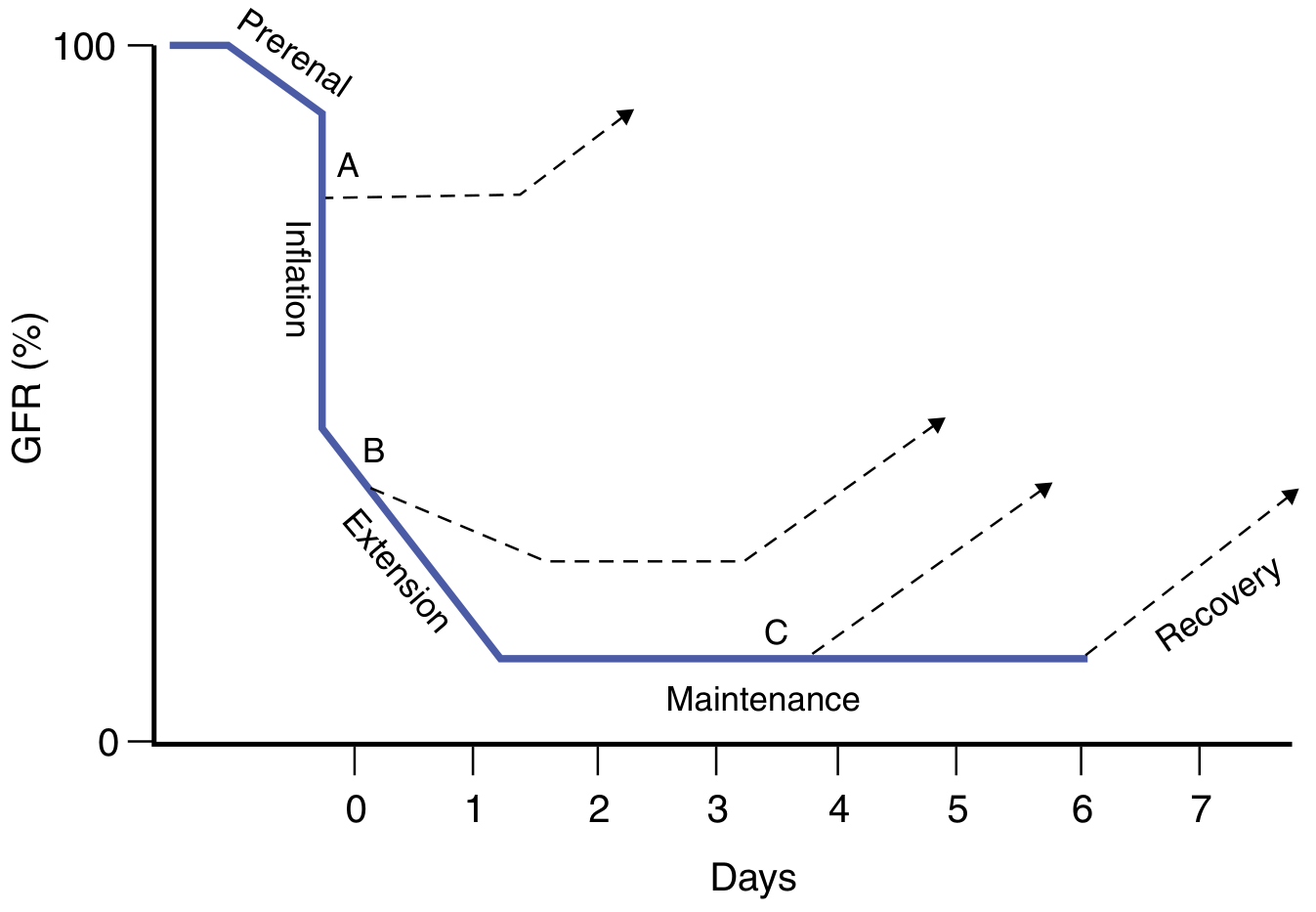
- Initiation phase: Ischemia/toxin → ATP depletion → tubular cell injury + cytokine release → afferent arteriolar vasoconstriction
- Extension phase: Continued inflammation, endothelial dysfunction, necrosis and apoptosis → further GFR fall. This is the key window for therapeutic intervention.
- Maintenance phase: GFR stabilizes at nadir; cell repair and regeneration begin; blood flow normalizes
- Recovery phase: Cellular differentiation, restoration of epithelial polarity, GFR improves
Most vulnerable tubular segments: S3 segment of the proximal tubule and the thick ascending limb of Henle in the outer medullary stripe — both have limited oxygen delivery.
Cell death occurs via two pathways:
- Necrosis: triggers profound inflammatory response
- Apoptosis: programmed cell death without major inflammation
— National Kidney Foundation Primer on Kidney Diseases, 8th Edition
Biomarkers
Serum creatinine is a late and insensitive marker — it may not rise for 8–48 hours after injury. Novel biomarkers allow earlier detection:
| Biomarker | Type | Notes |
|---|---|---|
| NGAL (neutrophil gelatinase-associated lipocalin) | Damage | Rises within 2–4 hrs; highly sensitive for ischemic/toxic AKI |
| KIM-1 (kidney injury molecule-1) | Damage | Shed from injured proximal tubule cells; specific for ischemia/toxin AKI |
| Cystatin C | Functional | More sensitive than creatinine for small GFR changes |
| TIMP-2 × IGFBP-7 | Cell stress/damage | Best combined predictor of stage 2–3 AKI in critically ill patients; measured from urine within 12 hrs |
| IL-18 | Damage | Tubular inflammation marker |
| Proenkephalin A | Functional | Newer functional marker |
KDIGO now recognizes a subclinical stage (1S) — biomarkers positive without meeting creatinine/UO criteria.
Furosemide stress test: IV furosemide 1–1.5 mg/kg; failure to produce >200 mL urine in 2 hours strongly predicts progression to stage 3 and need for dialysis.
— Comprehensive Clinical Nephrology, 7th Edition
Clinical Evaluation
History & Physical
- Volume depletion clues: vomiting, diarrhea, bleeding, poor PO intake, diuretic use
- Medications: NSAIDs, ACE-I/ARBs, aminoglycosides, contrast, PPI
- Signs of underperfusion: orthostatic hypotension, tachycardia, dry mucous membranes, flat JVP
- Signs of hypervolemia: peripheral edema, pulmonary crackles
- Rash → allergic AIN; skin emboli → cholesterol emboli
Key Lab/Urinary Investigations
| Test | Prerenal | Intrinsic ATI | Postrenal |
|---|---|---|---|
| BUN:Cr ratio | >20:1 | 10–15:1 | Variable |
| FENa | <1% | >1% (usually) | Variable |
| FEurea | <35% | >35% | — |
| Urinalysis | Normal/hyaline casts | Granular/muddy brown casts; RBC casts (GN) | Often normal |
| Urine biomarkers | Not elevated | Markedly elevated | — |
- Renal ultrasound: first-line imaging; evaluates for hydronephrosis, obstruction, kidney size
- Biopsy: indicated when cause is unclear, particularly for glomerulonephritis or atypical AIN
Treatment
General Principles
- Remove offending agents (nephrotoxins, NSAIDs, ACE-I/ARBs if hemodynamically unstable)
- Optimize intravascular volume: prompt but careful fluid resuscitation (balanced crystalloids preferred; avoid fluid overload, particularly in heart failure/cirrhosis/sepsis)
- Relieve obstruction: bladder catheter for BPH; ureteral stent or percutaneous nephrostomy for upper tract obstruction
Electrolyte & Metabolic Management
| Problem | Treatment |
|---|---|
| Hyperkalemia | Sodium zirconium cyclosilicate (Lokelma) or patiromer; low-K diet |
| Volume overload | Furosemide 40–80 mg IV; low-sodium diet |
| Hyperphosphatemia | Oral phosphate binders |
| Metabolic acidosis | Sodium bicarbonate tablets |
| Hypocalcemia | Oral calcium tablets |
Specific Treatments
- Glomerulonephritis / vasculitis / AIN: immunosuppressive therapy (e.g., prednisone 1 mg/kg for AIN, with gradual taper over 1 month)
- Septic/ischemic ATI: no specific pharmacotherapy; supportive care is the cornerstone
Renal Replacement Therapy (RRT)
Indications (the AEIOU of dialysis):
- Volume overload unresponsive to diuretics
- Hyperkalemia refractory to medical management
- Acidosis (metabolic)
- Uremic symptoms: encephalopathy, pericarditis, asterixis, myoclonus, seizures
- Serum creatinine ~10 mg/dL in symptomatic patients
Timing: Early initiation in stage 3 AKI showed no reduction in mortality in major trials; delayed initiation often allows spontaneous recovery with earlier diuresis and fewer adverse events — RRT should not be started routinely on a creatinine threshold alone.
Modalities:
- Intermittent hemodialysis (IHD): standard; hemodynamically stable patients
- Continuous RRT (CRRT): preferred in hemodynamically unstable patients (ICU)
- Peritoneal dialysis: alternative in selected settings
Complications
- Electrolyte disturbances: hyperkalemia, hyperphosphatemia, hypocalcemia
- Metabolic acidosis
- Pulmonary edema / volume overload
- Uremia: pericarditis, encephalopathy, bleeding (platelet dysfunction)
- Anemia
- Increased susceptibility to infections
- Progression to CKD: AKI independently accelerates CKD progression even after apparent recovery
Prognosis
- Many cases are mild and self-limited — ~⅓ resolve within 24 hours, ~60% by 48 hours, ~70% by 72 hours
- Prerenal AKI: excellent prognosis if perfusion is restored promptly
- Postrenal AKI: good prognosis if obstruction is relieved early; prolonged obstruction carries worse outcomes
- Intrinsic AKI: less favorable; even a 0.3 mg/dL creatinine rise increases mortality risk significantly; ICU-associated AKI carries mortality rates up to 50–70%
- Risk factors for poor outcome: older age, comorbidities (CKD, diabetes, heart failure), severity of AKI stage, oliguria, need for dialysis
- Survivors of AKI have higher long-term risk of CKD, cardiovascular events, and death
— Goldman-Cecil Medicine, 27th Edition; National Kidney Foundation Primer on Kidney Diseases, 8th Edition; Comprehensive Clinical Nephrology, 7th Edition
Prevention
- Identify high-risk patients: elderly, CKD, diabetes, heart failure, volume depletion
- Minimize nephrotoxin exposure; optimize hydration before contrast procedures
- Monitor creatinine and urine output in at-risk patients
- Avoid NSAID + ACE-I + diuretic "triple whammy" combination in volume-depleted patients
- AKI alert systems (electronic alerts in hospital) have been shown to improve detection — Electronic Alert Systems for AKI (JAMA Network Open, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.