Periodontitis
Reading File
Finding Sources
Searching PubMed
"periodontitis"[MeSH Terms] AND ("treatment" OR "management")
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full response.
Periodontitis
Definition
Periodontitis is a chronic inflammatory disease affecting the supporting structures of the teeth - the periodontal ligament, alveolar bone, and cementum. Unlike gingivitis (which is confined to the marginal gingiva and is reversible), periodontitis involves progressive, largely irreversible destruction of these supporting tissues.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 498
Etiology and Microbiology
Periodontitis is a polymicrobial infection primarily involving anaerobic gram-negative organisms derived from subgingival dental plaque. The key pathogens are:
| Organism | Notes |
|---|---|
| Porphyromonas gingivalis | Potent extracellular proteases; disrupts complement |
| Aggregatibacter (Actinobacillus) actinomycetemcomitans | Produces leukotoxin; implicated in aggressive/juvenile forms |
| Prevotella intermedia | Associated with adult chronic periodontitis |
| Treponema denticola | Binds serum factors to interfere with complement deposition |
-
Healthy gingival sites are colonized by facultative gram-positive organisms
-
Active periodontitis sites shift to anaerobic and microaerophilic gram-negative flora
-
Synergistic interactions between P. gingivalis, T. denticola, and other plaque members foster progression from gingivitis to chronic periodontitis
-
Robbins, Cotran & Kumar, p. 498-499; Sherris & Ryan's Medical Microbiology, p. 1509
Pathogenesis
The sequence of events:
- Dental plaque accumulation - a sticky biofilm of bacteria, salivary proteins, and epithelial cells collects in the gingival sulcus (subgingival plaque)
- Gingivitis - polymorphonuclear leukocytes, lymphocytes, and plasma cells infiltrate connective tissue adjacent to the gingival crevice; collagen is lost; this is reversible
- Progression to periodontitis - with continued inflammation, alveolar bone resorption begins; the sulcus deepens into a periodontal pocket
- Periodontal pocket deepening - creates a more anaerobic environment favoring pathogenic gram-negative flora
- Ligament destruction - periodontal ligament attachment is lost; teeth loosen
- Tooth loss - the endpoint if untreated; chronic periodontitis is the leading cause of tooth loss in adults >35-40 years
Key virulence mechanisms:
-
P. gingivalis proteases degrade collagen and tissue proteins
-
T. denticola evades complement
-
Bacterial Toll-like receptor (TLR) interactions trigger dysregulated host inflammatory responses
-
Sherris & Ryan's Medical Microbiology, p. 1509-1510
Clinical Presentation

Clinical features include:
- Gingival erythema, edema, bleeding on probing
- Periodontal pocket formation (probing depth >3 mm)
- Gingival recession, exposed root surfaces
- Tooth mobility and drifting
- Halitosis
- Eventual tooth loss if untreated
Disease progression is typically episodic - acute exacerbations separated by quiescent periods.
Classification
| Type | Features |
|---|---|
| Chronic (adult) periodontitis | Most common; slow progression; adults >35 years; closely linked to P. gingivalis, P. intermedia, T. denticola |
| Localized aggressive periodontitis | Adolescents; rapid loss of attachment; associated with A. actinomycetemcomitans leukotoxin |
| Generalized aggressive periodontitis | Young adults; widespread rapid bone loss |
| Necrotizing periodontal disease | Immunocompromised patients (HIV, poorly controlled diabetes); fusospirochetal organisms; painful ulcerative lesions with tissue necrosis |
A periodontal abscess can occur when a periodontal pocket becomes constricted, bacteria proliferate, and an acute inflammatory response develops within the occluded pocket.
Systemic Associations
Periodontitis is associated with a spectrum of systemic conditions:
-
Immunodeficiency: AIDS, neutrophil deficiency or dysfunction
-
Metabolic: Diabetes mellitus (bidirectional relationship - diabetes worsens periodontitis; periodontitis worsens glycemic control)
-
Inflammatory: Crohn disease, sarcoidosis, Down syndrome
-
Autoimmune: Rheumatoid arthritis (infection and smoking promote citrullination of self-proteins, contributing to RA pathogenesis)
-
Cardiovascular: Periodontal bacteria may seed infective endocarditis
-
Infectious: Periodontal bacteria can cause abscesses in the lungs and brain
-
Robbins, Cotran & Kumar, p. 500
Special note - HIV: Periodontal disease in HIV follows a staging:
- Linear gingival erythema - fiery red band disproportionate to plaque
- Necrotizing ulcerative gingivitis/periodontitis/stomatitis - progressive recession, bleeding, tissue sloughing, pain, malodor, loss of interdental papillae
- K.J. Lee's Essential Otolaryngology, p. 239
Investigations
- Dental probing - measures pocket depth (>3 mm = periodontitis)
- Dental X-rays / CT - assesses extent of alveolar bone resorption
- In necrotizing disease or new presentation: blood glucose and HIV testing
- If bony destruction is disproportionate to mucosal injury: biopsy to exclude malignancy or bacillary angiomatosis
Management
Non-Surgical (First-line)
| Intervention | Details |
|---|---|
| Oral hygiene | Twice-daily brushing and flossing |
| Scaling and root planing | Mechanical debridement of subgingival plaque and calculus (mainstay of treatment) |
| Chlorhexidine rinse | 0.12-0.2% preferred antibacterial rinse |
| Hydrogen peroxide | 3% diluted 1:1 with warm water (alternative) |
| Smoking cessation | Most important modifiable risk factor in HIV-negative patients |
| Analgesia | Ibuprofen 400-600 mg q6-8h or acetaminophen 650 mg q6h; topical viscous lidocaine for severe local pain |
Antibiotics (for severe disease, immunocompromise, or systemic symptoms)
| Antibiotic | Dose | Duration |
|---|---|---|
| Penicillin V | 500 mg TID-QID | 10 days |
| Amoxicillin/clavulanate | 500/125 mg TID (or 875/125 mg) | 10 days |
| Metronidazole | 500 mg BID (penicillin allergy) | 10 days |
| Clindamycin | 300 mg QID (penicillin allergy) | 10 days |
| Nystatin | 100,000 units/mL, 5 mL swish/spit QID | 10 days (immunocompromised) |
- Rosen's Emergency Medicine, p. 2720-2721
Necrotizing Disease
- Dentist-performed debridement of necrotic tissue
- Systemic antimicrobials
- In HIV: chlorhexidine + nystatin mouthwash (covers bacterial and fungal etiologies)
Surgical Options (refractory/advanced disease)
- Flap surgery for access to deeper pockets
- Bone grafting and guided tissue regeneration
- Tooth extraction when irreversibly compromised
Recent Evidence (2024-2026)
Recent systematic reviews note:
- Probiotics as adjuncts to non-surgical treatment show some benefit in reducing pocket depth (PMID: 39407177)
- PRP and injectable PRF as adjuncts in non-surgical treatment have emerging supportive evidence (PMID: 38928026)
- Electronic cigarette use is associated with worse periodontal outcomes - similar to conventional smoking (PMID: 39385155)
Key Points Summary
- Periodontitis = irreversible destruction of tooth-supporting structures (bone + ligament + cementum)
- The shift from gram-positive to gram-negative anaerobic flora is central to pathogenesis
- The "red complex" pathogens (P. gingivalis, T. denticola, T. forsythia) drive chronic disease
- Not reversible - lost bone does not regenerate; treatment halts progression
- Strong bidirectional links with diabetes, cardiovascular disease, and RA make it a systemic disease concern
- First-line treatment is mechanical (scaling/root planing) ± antibiotics for severe cases
Cirrhosis long answer in detail according to medicine Pathophysiology in flowchart form, clincial features system wise and also types of cirrhosis and their pathogenesis
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Let me compose it.
CIRRHOSIS - Detailed Long Answer
1. DEFINITION
Cirrhosis is the end-stage of any chronic liver disease, defined histopathologically as diffuse architectural distortion of the liver by fibrous bands that subdivide the hepatic parenchyma into regenerative nodules. It is characterized by:
- Irreversible (largely) destruction of normal liver architecture
- Fibrous replacement of hepatic parenchyma
- Formation of regenerative nodules
- Portosystemic vascular shunting
"Regardless of the cause of cirrhosis, the pathologic features consist of the development of fibrosis to the point that there is architectural distortion with the formation of regenerative nodules."
- Harrison's Principles of Internal Medicine 22E
2. ETIOLOGY / CAUSES
| Category | Specific Causes |
|---|---|
| Alcohol | Alcoholic liver disease (~48% of cirrhosis deaths) |
| Viral hepatitis | Chronic hepatitis B, Chronic hepatitis C |
| Metabolic | MASLD/NASH (Metabolic dysfunction-associated steatohepatitis) |
| Biliary | Primary biliary cholangitis (PBC), Primary sclerosing cholangitis (PSC), Biliary atresia, Cystic fibrosis |
| Autoimmune | Autoimmune hepatitis, Autoimmune cholangiopathy |
| Metabolic/Genetic | Hemochromatosis, Wilson's disease, Alpha-1 antitrypsin deficiency |
| Vascular | Budd-Chiari syndrome, Hepatic venous outflow obstruction, Right heart failure (cardiac cirrhosis) |
| Drugs/Toxins | Methotrexate, amiodarone, intestinal bypass |
| Cryptogenic | No identifiable cause (~10-15%) |
3. MORPHOLOGY
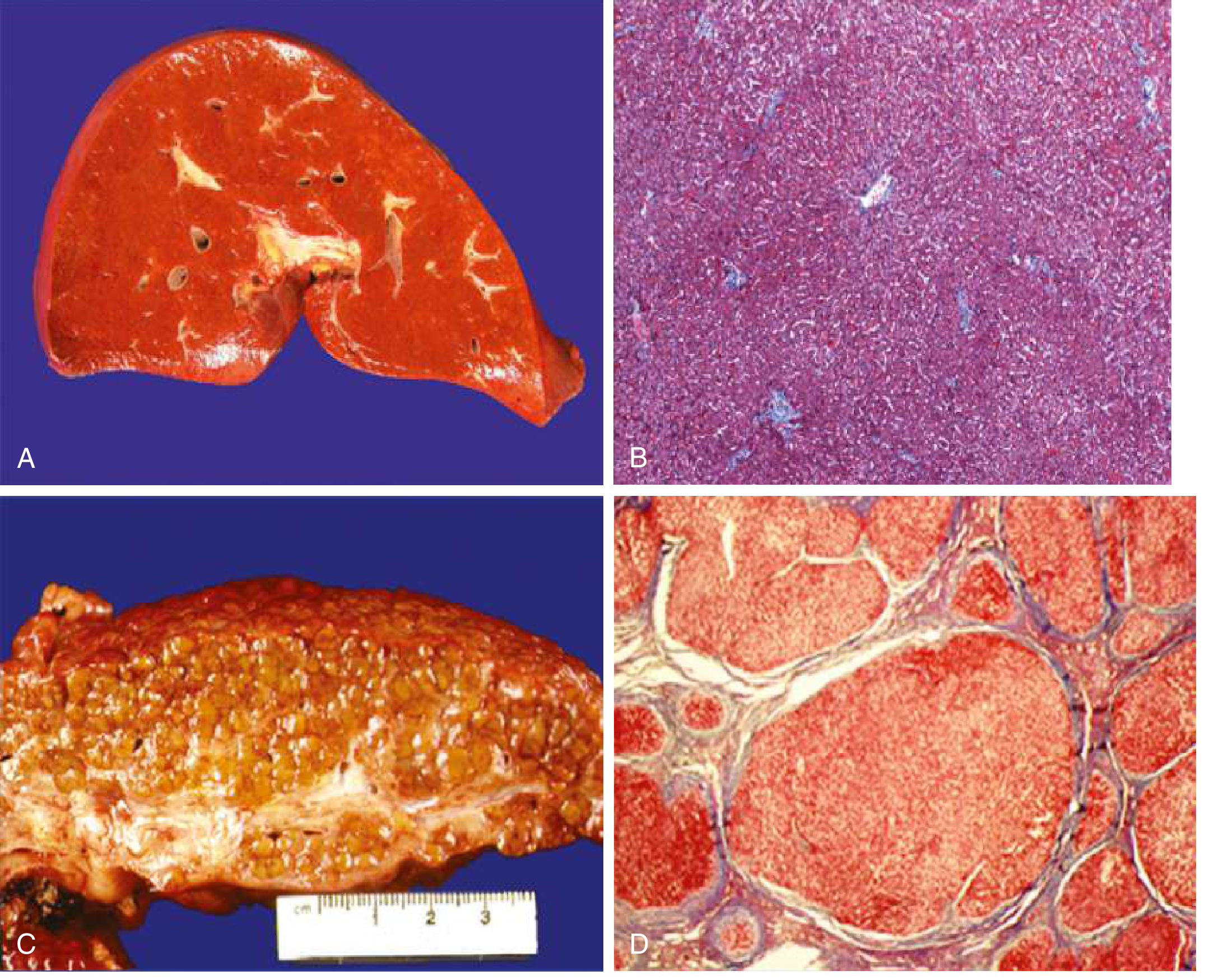

Gross:
- Nodular, bumpy liver surface
- Depressed areas of scarring alternating with bulging regenerative nodules
- May be small/shrunken (late) or enlarged (early/fatty)
Microscopic:
- Parenchymal nodules surrounded by dense fibrous bands
- Variable nodule size
- Fibrous bands linking portal tracts to each other (portal-portal bridging) or portal tracts to central veins (portal-central bridging)
- Vascular distortion with portosystemic shunts
Nodule classification by size:
| Type | Size | Causes |
|---|---|---|
| Micronodular | <3 mm | Alcoholic, hemochromatosis, biliary obstruction |
| Macronodular | >3 mm | Viral hepatitis, Wilson's disease |
| Mixed | Both | Late alcoholic (after abstinence), various |
4. PATHOPHYSIOLOGY - FLOWCHART
CHRONIC LIVER INJURY (alcohol / virus / fat / autoimmune / metabolic)
│
▼
HEPATOCYTE DAMAGE + INFLAMMATION
(necrosis, apoptosis, Kupffer cell activation → profibrogenic cytokines:
TGF-β, PDGF, TNF-α, IL-1)
│
▼
ACTIVATION OF HEPATIC STELLATE CELLS (Ito cells / perisinusoidal cells)
• Normally quiescent in space of Disse; store vitamin A (retinoids)
• On activation: lose vitamin A, proliferate, transform into myofibroblasts
• Secrete: Collagen types I & III, proteoglycans, glycoproteins
• Become contractile → vasoconstriction of sinusoids
│
▼
FIBROSIS DEPOSITION IN SPACE OF DISSE
• "Capillarization" of sinusoids (loss of sinusoidal fenestrae)
• ↓ Exchange between plasma and hepatocytes
• ↑ Sinusoidal resistance
│
▼
PROGRESSIVE ARCHITECTURAL DISTORTION
• Formation of fibrous septa bridging portal-portal and portal-central
• Hepatocyte regeneration → nodule formation (regenerative nodules)
• Normal vascular relationships destroyed → portosystemic shunts
│
▼
CIRRHOSIS (end-stage fibrosis)
│
┌─────┴──────┐
▼ ▼
PORTAL LIVER CELL
HYPERTENSION INSUFFICIENCY
│ │
▼ ▼
(see below) Jaundice, coagulopathy,
hypoalbuminemia, encephalopathy
Portal Hypertension - Detailed Mechanism:
CIRRHOSIS
│
├── FIXED COMPONENT
│ (Fibrous tissue + nodules compressing sinusoids)
│
└── FUNCTIONAL COMPONENT
(↓ Intrahepatic NO → active vasoconstriction by stellate cells)
│
▼
↑ SINUSOIDAL RESISTANCE
│
▼
↑ PORTAL VENOUS PRESSURE (>12 mmHg)
│
┌──────┴──────────────────────┐
▼ ▼
SPLANCHNIC VASODILATION PORTOSYSTEMIC
(↑ extrahepatic NO) COLLATERALS
│ (esophageal,
▼ gastric, rectal,
↓ Effective arterial caput medusae)
blood volume │
│ ▼
▼ VARICEAL BLEEDING
Activation of RAAS +
SNS + ADH
│
▼
Na⁺ and water retention
│
┌────┴─────┐
▼ ▼
ASCITES HYPONATREMIA
│
▼
HYPERDYNAMIC CIRCULATION
(↑ CO, ↓ SVR, ↑ heart rate)
│
▼
SBP / HEPATORENAL SYNDROME
"The paradox in portal hypertension is that a deficiency of NO in the intrahepatic vasculature leads to vasoconstriction and increased resistance, whereas overproduction of NO in the extrahepatic circulation leads to vasodilation and increased portal flow."
- Goldman-Cecil Medicine
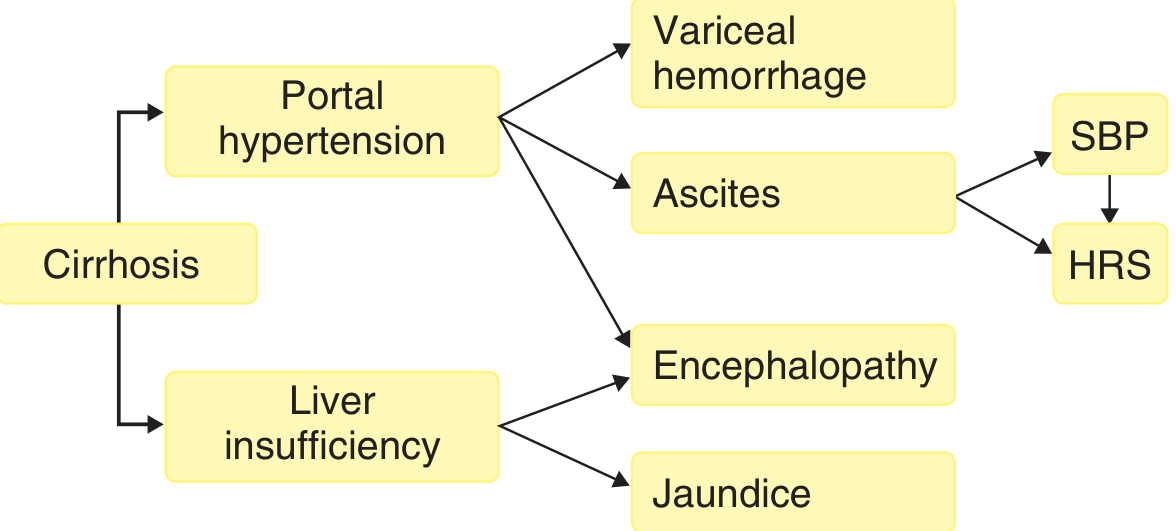
5. COMPLICATIONS OF CIRRHOSIS - OVERVIEW DIAGRAM
6. CLINICAL FEATURES - SYSTEM-WISE
A. General / Constitutional
- Fatigue, weakness, anorexia, weight loss
- Muscle wasting (sarcopenia)
- Fever (due to bacteremia or alcoholic hepatitis)
- ~40% are asymptomatic until advanced disease
B. Gastrointestinal System
| Feature | Mechanism |
|---|---|
| Right upper quadrant pain | Liver capsule stretching / hepatitis |
| Nausea, vomiting | Portal hypertension; alcohol toxicity |
| Anorexia, early satiety | Ascites compressing stomach |
| Hepatomegaly (early) → small liver (late) | Initially enlarged; shrinks with fibrosis |
| Splenomegaly | Portal hypertension → venous congestion |
| Hypersplenism | Splenic sequestration → thrombocytopenia, leukopenia, anemia |
| Esophageal/gastric varices | Portal-systemic collaterals |
| Variceal hemorrhage | Variceal rupture - most feared complication |
| Caput medusae | Periumbilical collateral veins (recanalization of umbilical vein) |
| Hemorrhoids (anorectal varices) | Portal-systemic collaterals |
| Peptic ulcers | Increased gastrin, impaired mucosal defense |
C. Skin and Integument
| Feature | Mechanism |
|---|---|
| Jaundice / Icterus | Impaired bilirubin conjugation and excretion |
| Palmar erythema | Hyperestrogenemia → local vasodilation |
| Spider angiomas (>5 = significant) | Hyperestrogenemia → arterial dilatation; central pulsating arteriole |
| Pruritus | Cholestasis → bile acid deposition in skin |
| Leukonychia (white nails) | Hypoalbuminemia |
| Terry's nails | Distal brown band |
| Clubbing | Hepatopulmonary syndrome |
| Dupuytren's contracture | Fibrosis of palmar fascia (alcohol) |
| Purpura / bruising | Coagulopathy, thrombocytopenia |
| Xanthelasma / xanthomata | Cholestasis → altered lipid metabolism (PBC) |
| Hyperpigmentation | Scratching from pruritus; hemochromatosis |
| Hair loss | Hormonal disturbance |
D. Endocrine / Reproductive System
| Feature | Mechanism |
|---|---|
| Gynecomastia | ↑ Estrogen (impaired hepatic metabolism) |
| Testicular atrophy / hypogonadism | Hyperestrogenemia + hypothalamic-pituitary axis disruption |
| Loss of body/axillary/pubic hair | Hormonal imbalance |
| Menstrual irregularity / amenorrhea | Disruption of hypothalamic-pituitary axis |
| Parotid enlargement | Alcoholic cirrhosis |
| Diabetes mellitus | Impaired hepatic glucose metabolism ("hepatogenous diabetes") |
| Hypoglycemia | Reduced glycogen stores |
E. Cardiovascular System (Hyperdynamic Circulation)
| Feature | Mechanism |
|---|---|
| ↑ Cardiac output | Splanchnic/systemic vasodilation (↑ NO) |
| ↓ SVR | Peripheral vasodilation |
| Tachycardia | Compensatory |
| Bounding pulse | Hyperdynamic state |
| Hepatopulmonary syndrome (HPS) | Intrapulmonary arteriovenous shunts; platypnea-orthodeoxia |
| Portopulmonary hypertension | Portal hypertension → pulmonary vasoconstriction |
| Cirrhotic cardiomyopathy | Reduced cardiac contractility despite high output state |
F. Respiratory System
| Feature | Mechanism |
|---|---|
| Dyspnea | Ascites → diaphragm elevation; pleural effusion (hepatic hydrothorax); HPS |
| Hepatic hydrothorax | Passage of ascitic fluid through diaphragmatic defects |
| Clubbing + cyanosis | HPS (platypnea-orthodeoxia) |
| Reduced SpO₂ on standing | HPS - improves lying down |
G. Renal System
| Feature | Mechanism |
|---|---|
| Ascites | Sinusoidal hypertension + Na⁺ retention (RAAS activation) |
| Hyponatremia | Free water retention (ADH activation) |
| Hepatorenal syndrome (HRS) | Renal vasoconstriction from systemic vasodilation; functional renal failure; reversible with liver transplantation |
| - Type 1 HRS | Rapid progressive renal failure (<2 weeks) |
| - Type 2 HRS | Slower course; linked to refractory ascites |
| Proteinuria / hematuria | IgA nephropathy (in alcoholic cirrhosis) |
H. Nervous System
| Feature | Mechanism |
|---|---|
| Hepatic encephalopathy (HE) | Portosystemic shunting + liver insufficiency → ammonia and other toxins bypass liver; reach brain |
| Grade I | Altered sleep, mild confusion, personality change |
| Grade II | Asterixis (flapping tremor), disorientation |
| Grade III | Somnolence, stupor, gross disorientation |
| Grade IV | Coma |
| Asterixis | Impaired motor inhibition; seen in Grade II HE |
| Peripheral neuropathy | Nutritional deficiency (B1, B12, folate); alcohol toxicity |
| Wernicke-Korsakoff syndrome | Thiamine (B1) deficiency in alcoholic cirrhosis |
I. Hematological System
| Feature | Mechanism |
|---|---|
| Anemia | Hypersplenism, GI blood loss, nutritional deficiency, bone marrow suppression (alcohol) |
| Thrombocytopenia | Hypersplenism + reduced thrombopoietin |
| Leukopenia | Hypersplenism |
| Coagulopathy (↑PT/INR) | Reduced synthesis of clotting factors II, V, VII, IX, X; factor VII has shortest half-life so affected first |
| ↓ Fibrinogen | Reduced hepatic synthesis |
| Disseminated intravascular coagulation (DIC) risk | In decompensated cirrhosis |
J. Musculoskeletal System
| Feature | Mechanism |
|---|---|
| Sarcopenia (muscle wasting) | Malnutrition, hyperammonemia, hormonal disturbance |
| Hepatic osteodystrophy | Osteoporosis/osteomalacia from malabsorption of fat-soluble vitamins (D); common in PBC/PSC |
| Dupuytren's contracture | Palmar fibromatosis (alcohol-related) |
| Hypertrophic osteoarthropathy | Clubbing and periosteal thickening |
7. TYPES OF CIRRHOSIS AND THEIR PATHOGENESIS
A. Alcoholic Cirrhosis
Pathogenesis:
Chronic Alcohol Ingestion
│
▼
Metabolism via:
• ADH → Acetaldehyde
• MEOS (CYP2E1 induction) → ROS + more acetaldehyde
• Catalase (peroxisomal)
│
▼
Acetaldehyde (highly reactive):
• Forms acetaldehyde-protein adducts
• Disrupts microtubular function
• Impairs protein secretion/trafficking
│
▼
Hepatocyte damage + ↑ Triglycerides (steatosis)
↑ ROS → Oxidative membrane damage
│
▼
Kupffer cell activation → TGF-β, TNF-α, IL-1
│
▼
Stellate cell activation → Collagen deposition
│
▼
Centrilobular fibrosis → Pericellular fibrosis → Periportal fibrosis
│
▼
Bridging fibrosis (portal-central) → MICRONODULAR CIRRHOSIS
(nodules <3 mm)
Key features:
- Micronodular pattern initially; mixed macro/micronodular after abstinence
- Mallory-Denk bodies (cytokeratin inclusions) on histology
- AST:ALT ratio typically >2:1 (alcoholic cirrhosis hallmark)
- Associated with Zieve's syndrome (hemolytic anemia + jaundice + hyperlipidemia)
B. Viral Cirrhosis (Hepatitis B and C)
Pathogenesis - HBV:
HBV Chronic Infection
│
▼
Direct cytopathic effect + Immune-mediated hepatocyte destruction
(CD8+ T cell attack on HBsAg/HBeAg-expressing hepatocytes)
│
▼
Cycles of necrosis-inflammation-regeneration
│
▼
Progressive portal-portal and portal-central bridging fibrosis
│
▼
MACRONODULAR CIRRHOSIS (nodules >3 mm)
│
▼
↑↑ Risk of HCC (HBV can be directly oncogenic - integrates into genome)
Pathogenesis - HCV:
HCV Chronic Infection
│
▼
Immunological injury (mainly immune-mediated, not direct cytopathic)
Steatosis (especially genotype 3)
│
▼
Periportal inflammation (interface hepatitis)
Lymphoid follicles in portal tracts (HCV hallmark)
│
▼
Periportal fibrosis → Bridging fibrosis → MACRONODULAR CIRRHOSIS
│
▼
↑ HCC risk (requires cirrhosis as intermediary - unlike HBV)
Note: With successful HCV cure (SVR with DAAs), cirrhosis can regress (75% regression at year 5 with TDF in HBV).
C. Biliary Cirrhosis
Two main types:
Primary Biliary Cholangitis (PBC)
Autoimmune attack on intrahepatic bile duct epithelium
(Anti-mitochondrial antibodies - AMA in >95%)
│
▼
Progressive destruction of small/medium intrahepatic bile ducts
(Granulomatous cholangitis - "florid duct lesion")
│
▼
Cholestasis → bile acid accumulation → hepatocyte injury
│
▼
Periportal fibrosis → Portal-portal bridging → CIRRHOSIS
Key features: Middle-aged women; AMA positive; ALP/GGT elevated; pruritus, fatigue, xanthelasma; ↑IgM; treat with UDCA (13-15 mg/kg/day)
Primary Sclerosing Cholangitis (PSC)
Fibro-obliterative inflammation of intra- AND extra-hepatic bile ducts
(Onion-skin periductal fibrosis)
│
▼
"Beaded" appearance on MRCP (strictures alternating with dilatation)
│
▼
Progressive biliary obstruction → BILIARY CIRRHOSIS
│
▼
↑ Risk of cholangiocarcinoma (10-15% lifetime risk)
Key features: Young men; ~80% associated with IBD (UC > Crohn's); pANCA positive; no proven effective medical therapy; liver transplantation definitive.
D. MASLD/NASH Cirrhosis (Metabolic Cirrhosis)
Obesity / Insulin Resistance / Metabolic Syndrome
│
▼
Hepatic steatosis (First Hit: ↑ FFA delivery to liver)
│
▼
Oxidative stress + Mitochondrial dysfunction + Gut dysbiosis
(Second Hit)
│
▼
Lobular inflammation + Hepatocyte ballooning + Mallory-Denk bodies
(Steatohepatitis = NASH)
│
▼
Progressive fibrosis (perisinusoidal/pericellular "chicken-wire" pattern)
│
▼
MACRONODULAR/MIXED CIRRHOSIS
│
▼
↑ HCC risk (can occur even without cirrhosis in MASLD)
E. Cardiac (Congestive) Cirrhosis
Chronic right-sided heart failure / Constrictive pericarditis /
Tricuspid regurgitation / Budd-Chiari syndrome
│
▼
Hepatic venous outflow obstruction
│
▼
Sinusoidal congestion (centrilobular) → Centrilobular necrosis
"Nutmeg liver" (gross appearance: yellow-red mottling)
│
▼
Pericentral fibrosis → "Reversed lobule" pattern
│
▼
CARDIAC CIRRHOSIS (rare - requires many years)
Key features: Hepatomegaly, pulsatile liver (TR), elevated JVP, peripheral edema preceding ascites; AST/ALT may be very elevated acutely ("shock liver").
F. Metabolic/Genetic Cirrhosis
Hemochromatosis (Hereditary)
HFE gene mutation (C282Y most common) → ↑ GI iron absorption
│
▼
Iron deposition in hepatocytes, Kupffer cells, bile duct epithelium
│
▼
ROS generation → Hepatocyte damage → Fibrosis
│
▼
MICRONODULAR CIRRHOSIS
- Triad: Cirrhosis + Diabetes ("bronze diabetes") + Skin pigmentation
- ↑ Serum ferritin, ↑ Transferrin saturation (>45%)
- Treatment: Phlebotomy
Wilson's Disease
ATP7B mutation → ↓ Hepatic copper excretion into bile
│
▼
Copper accumulation → Oxidative liver injury
│
▼
Acute hepatitis → Chronic hepatitis → MACRONODULAR CIRRHOSIS
+ Neuropsychiatric features (basal ganglia) + Kayser-Fleischer rings
- Young patients (<40 years)
- ↓ Serum ceruloplasmin, ↑ Urinary copper, liver biopsy (quantitative copper)
Alpha-1 Antitrypsin Deficiency
PiZZ phenotype → Misfolded AAT accumulates in hepatocytes (ER stress)
(instead of being secreted into blood)
│
▼
Hepatocyte injury → PAS-positive diastase-resistant globules in hepatocytes
│
▼
Progressive fibrosis → CIRRHOSIS
+ Emphysema (↓ AAT in lung → ↑ elastase → alveolar destruction)
8. STAGING AND PROGNOSIS
Child-Turcotte-Pugh (CTP) Score
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Bilirubin (mg/dL) | <2 | 2-3 | >3 |
| Albumin (g/dL) | >3.5 | 2.8-3.5 | <2.8 |
| PT prolongation (sec) | <4 | 4-6 | >6 |
| Ascites | None | Mild | Moderate-severe |
| Encephalopathy | None | Grade I-II | Grade III-IV |
- Class A (5-6 pts): 1-year survival ~100%; compensated
- Class B (7-9 pts): 1-year survival ~80%
- Class C (10-15 pts): 1-year survival ~45%; decompensated
MELD Score
MELD = 3.78 × ln[Bilirubin] + 11.2 × ln[INR] + 9.57 × ln[Creatinine] + 6.43
- Used for organ allocation in liver transplantation
- Predicts 90-day mortality
Compensated vs. Decompensated
| Compensated | Decompensated |
|---|---|
| No major complications | Ascites, variceal bleed, encephalopathy, jaundice |
| Median survival >12 years | Median survival 2 years |
| Stage 1 & 2 | Stage 3 & 4 |
9. INVESTIGATIONS
| Investigation | Finding |
|---|---|
| LFTs | ↑ Bilirubin, ↑ ALP, ↑ GGT; AST & ALT elevated (AST>ALT in alcohol) |
| Albumin | Low (<3.5 g/dL) - marker of synthetic failure |
| PT/INR | Prolonged - reduced clotting factor synthesis |
| CBC | Thrombocytopenia, anemia, leukopenia (hypersplenism) |
| Serum Na⁺ | Hyponatremia in advanced disease |
| Creatinine | Elevated in HRS |
| AFP | Elevated in HCC surveillance |
| Ultrasound | Nodular liver, splenomegaly, ascites, portal vein diameter >13 mm |
| Doppler | Portal vein flow reversal (hepatofugal) in advanced disease |
| Upper GI endoscopy | Varices grading |
| Liver biopsy (gold standard) | Confirms diagnosis; Metavir staging F0-F4 |
| Fibroscan (TE) | Non-invasive liver stiffness measurement (>12.5 kPa = cirrhosis) |
| HVPG | Hepatic venous pressure gradient (>5 mmHg = portal HTN; >12 mmHg = varices/ascites risk) |
10. MANAGEMENT SUMMARY
| Complication | Treatment |
|---|---|
| Ascites | Low-sodium diet + Spironolactone ± Furosemide; therapeutic paracentesis + IV albumin for large-volume ascites |
| SBP | IV Cefotaxime or Pip-Tazo; secondary prophylaxis with Norfloxacin/Ciprofloxacin |
| Variceal hemorrhage | Terlipressin/Octreotide; endoscopic band ligation; TIPS; primary prophylaxis: non-selective beta-blockers (propranolol/carvedilol) |
| HE | Identify precipitant; Lactulose; Rifaximin; low-protein diet (avoid excessive restriction) |
| HRS | Terlipressin + IV albumin; TIPS; definitive = liver transplantation |
| Coagulopathy | Vitamin K (if responsive); FFP/cryoprecipitate for active bleeding |
| HCC | Locoregional therapy (TACE, ablation); sorafenib; liver transplantation (Milan criteria) |
| Definitive | Liver Transplantation - only cure |
Sources:
- Harrison's Principles of Internal Medicine 22E, Chapter 355 (Cirrhosis and its Complications)
- Goldman-Cecil Medicine International Edition, Chapter 139 (Liver Fibrosis and Cirrhosis)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 18 (Chronic Liver Failure and Cirrhosis)
- Robbins & Kumar Basic Pathology, Chapter 18 (Portal Hypertension)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.