Introduction to water and electrolyte balai with clinical importance
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the material needed for a comprehensive, well-structured answer. Here it is:
Water and Electrolyte Balance - Introduction with Clinical Importance
1. Total Body Water (TBW)
Total body water (TBW) is defined as the overall percentage of water relative to total body weight. In a healthy adult, TBW accounts for 50-60% of body weight, with variation based on body composition and sex:
| Population | TBW (% body weight) |
|---|---|
| Adult male | ~60% |
| Adult female | ~50-55% |
| Obese individuals | Lower (fat has less water than muscle) |
| Neonates | ~75% |
In a standard 70 kg male: TBW = 42 L total.
2. Fluid Compartments
The body's water is distributed across two major compartments, subdivided further:
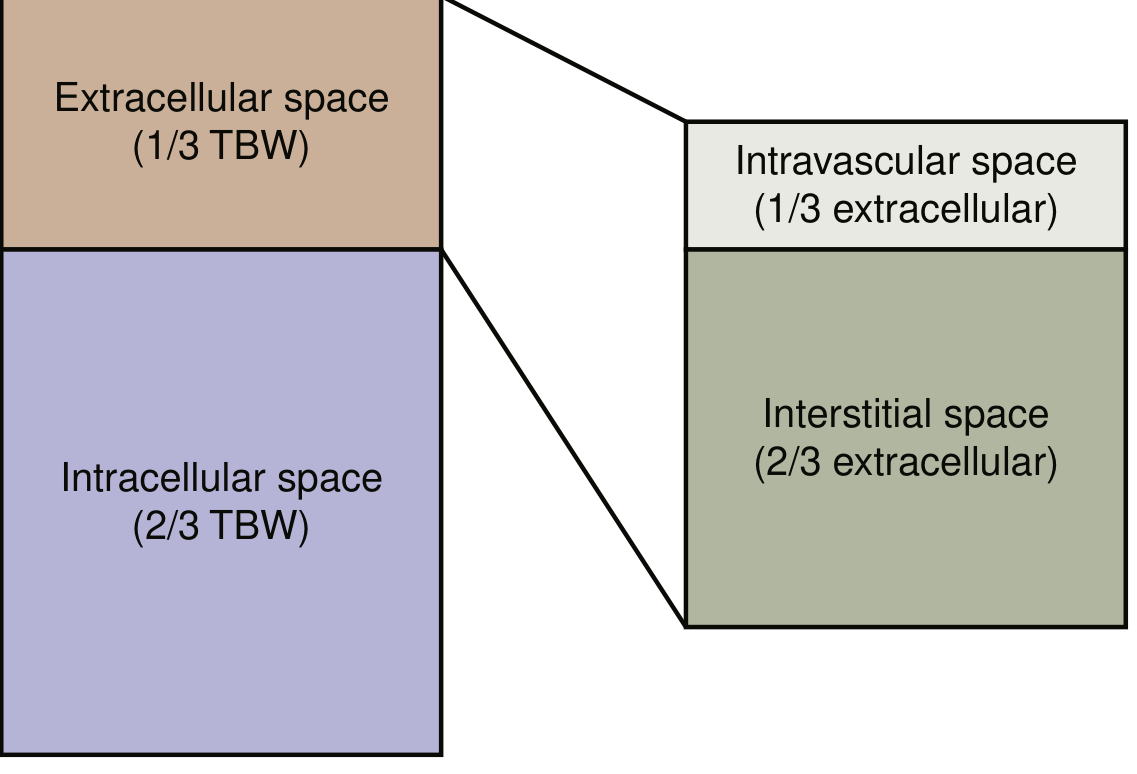
In a 70 kg male:
- Intracellular fluid (ICF): 28 L (2/3 of TBW)
- Extracellular fluid (ECF): 14 L (1/3 of TBW)
- Intravascular (plasma): ~4.7 L (1/3 of ECF)
- Interstitial: ~9.3 L (2/3 of ECF)
- Transcellular (CSF, pleural, peritoneal): ~1 L
- Current Surgical Therapy 14e, p. 1492
3. Electrolyte Distribution
The key principle is that while overall osmolality is equal across compartments (~280-295 mOsm/kg), the type of solutes differs:
| Compartment | Primary Cation | Primary Anion |
|---|---|---|
| Extracellular (ECF) | Na+ (142 mEq/L) | Cl-, HCO3- |
| Intracellular (ICF) | K+ (150 mEq/L) | Phosphate, proteins |
This gradient is maintained by the Na+/K+-ATPase pump, which actively transports:
- 3 Na+ out of the cell
- 2 K+ into the cell
This creates a net negative resting membrane potential, essential for nerve conduction and muscle contraction. Because Na+ and K+ cannot freely cross the lipid membrane, they serve as effective osmoles that drive water movement between compartments.
4. Osmolality and Its Regulation
Serum osmolality is estimated by:
Serum Osmolality = 2([Na+] + [K+]) + [BUN]/2.8 + [Glucose]/18
Normal range: 275-290 mOsm/kg H2O (physiologic variation: 1-2%)
Osmoregulation
Variations in osmolality are sensed by osmoreceptors in the hypothalamus:
- Hyperosmolality → stimulates thirst + releases ADH (vasopressin) from the posterior pituitary
- ADH acts on V2 receptors in the distal collecting tubule → upregulates aquaporin channels → increases water reabsorption → concentrated urine (up to 1200 mOsm/kg)
- Hypo-osmolality → suppresses ADH → dilute urine
- Current Surgical Therapy 14e, p. 1493
5. Volume Regulation - The RAAS Axis
While osmolality is regulated by ADH, volume is primarily regulated by the Renin-Angiotensin-Aldosterone System (RAAS):
- Renal hypoperfusion or low Na+ → detected by the juxtaglomerular apparatus (macula densa)
- Renin release → cleaves angiotensinogen → Angiotensin I → converted by ACE to Angiotensin II
- Angiotensin II → stimulates aldosterone release from adrenal zona glomerulosa
- Aldosterone → acts on distal convoluted tubule and collecting duct → promotes Na+ reabsorption and K+ excretion
- Na+ retention → water follows osmotically → volume expansion
The competing axis is Atrial Natriuretic Peptide (ANP) and Brain Natriuretic Peptide (BNP):
- Released from atrial/ventricular myocytes in response to volume overload
- Promotes natriuresis (Na+ excretion) and opposes RAAS
- Harrison's Principles of Internal Medicine 22E, p. 324; Current Surgical Therapy 14e, p. 1493
6. Starling's Law and Capillary Fluid Exchange
Transcapillary water movement follows Starling's Law:
Jv ∝ K [(Pc - Pi) - σ(πc - πi)]
Where:
- Pc = capillary hydrostatic pressure (pushes fluid OUT into interstitium)
- Pi = interstitial hydrostatic pressure
- πc = capillary oncotic pressure (pulls fluid IN - generated by plasma proteins, mainly albumin)
- πi = interstitial oncotic pressure
- K = membrane filtration coefficient
- σ = reflection coefficient
In normal physiology, hydrostatic pressure moves fluid into the interstitium, while plasma oncotic pressure returns it to the vasculature. Lymphatics drain any excess. Disruption of this balance causes edema.
- Current Surgical Therapy 14e, p. 1492
7. Key Electrolytes and Clinical Significance
Sodium (Na+) - Normal: 135-145 mEq/L
| Disorder | Serum Na | Key Features | Treatment |
|---|---|---|---|
| Hyponatremia | < 135 mEq/L | Nausea, headache, confusion, seizures (if severe); brain swelling | Water restriction (if hypotonic); treat underlying cause; hypertonic saline (3%) if severe/symptomatic |
| Hypernatremia | > 145 mEq/L | Thirst, lethargy, seizures; cellular shrinkage | Administer water, hypotonic saline (0.45%), or 5% dextrose |
Potassium (K+) - Normal: 3.5-5.0 mEq/L
| Disorder | ECG Findings | Treatment |
|---|---|---|
| Hypokalemia (< 3.5) | Flattened T waves, U waves, ST depression | Oral/IV K+ replacement; address cause |
| Hyperkalemia (> 5.5) | Peaked T waves, widened QRS, loss of P waves, sine wave pattern | IV Calcium gluconate (cardioprotection) + Insulin/dextrose + Albuterol nebulizer + Kayexalate/patiromer + Dialysis if refractory |
Emergency management of hyperkalemia (stepwise):
- IV Calcium gluconate - stabilizes cardiac membrane (immediate)
- IV Insulin (10-20 U) + 25-50g Dextrose - shifts K+ intracellularly (within 15-30 min)
- Inhaled Albuterol (10-20 mg nebulizer) - promotes intracellular K+ uptake
- Exchange resins (patiromer, sodium zirconium cyclosilicate) - remove K+ from GI tract
- Emergent dialysis if resistant
- Brenner & Rector's The Kidney, p. (block 16)
Aldosterone and Mineralocorticoid Balance
Hyperaldosteronism results in:
- Positive Na+ balance → extracellular volume expansion
- Low K+ (hypokalemia)
- Alkalosis
- Hypertension (chronic)
Aldosterone deficiency (Addison's disease) results in:
- Na+ wasting, volume contraction
- Hyponatremia, hyperkalemia, acidosis
- Hypotension / vascular collapse
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1030
8. Gastrointestinal Fluid and Electrolyte Losses
Each day, 8-10 L of fluid enters the duodenum: 2 L from diet, the rest from GI secretions. The small intestine absorbs ~8-9 L, delivering 1.5 L to the colon. The colon absorbs all but ~100 mL.
Electrolyte composition of GI secretions (clinically important for replacement):
| Fluid | Daily Vol (mL) | Na+ (mEq/L) | K+ (mEq/L) | Cl- (mEq/L) | HCO3- (mEq/L) |
|---|---|---|---|---|---|
| Saliva | 1000 | 30-80 | 15 | 70 | 30 |
| Gastric | 1000-2000 | 60-80 | 10 | 100 | 0 |
| Pancreas | 1000 | 140 | 20 | 60-90 | 40-100 |
| Bile | 1000 | 140 | 75 | 100 | 40 |
| Small bowel | 2000-5000 | 140 | 20 | 100 | 25-50 |
| Large bowel | 200-1500 | 75 | 30 | 30 | 0 |
Clinical pearl: Vomiting (gastric losses) → hypochloremic, hypokalemic metabolic alkalosis. Diarrhea (colonic/small bowel losses) → hyperchloremic metabolic acidosis with hypokalemia.
- Current Surgical Therapy 14e, p. 1494
9. Common IV Fluids and Their Composition
| Fluid | Na+ (mEq/L) | K+ | Cl- | HCO3- | Osmolality | Use |
|---|---|---|---|---|---|---|
| Normal Saline (0.9%) | 154 | 0 | 154 | 0 | 308 | Volume expansion, resuscitation |
| Lactated Ringer's (LR) | 130 | 4 | 109 | 28 | 275 | Closest to ECF; preferred for surgery/burns |
| 0.45% NaCl (½NS) | 77 | 0 | 77 | 0 | 154 | Hypotonic maintenance |
| 3% NaCl (Hypertonic saline) | 513 | 0 | 513 | 0 | 1026 | Severe symptomatic hyponatremia, cerebral edema |
| Normal ECF | 142 | 4 | 103 | 27 | 280 | (reference) |
- Current Surgical Therapy 14e, p. 1494
10. Acid-Base Considerations
Electrolyte disorders are closely tied to acid-base status:
- Metabolic acidosis (HCO3- < 15 mEq/L or pH < 7.15) requires urgent treatment - IV bicarbonate for AKI-related acidosis; treat the underlying cause in lactic acidosis
- Bicarbonate therapy risks: metabolic alkalosis, hypocalcemia, hypokalemia, hypernatremia, volume overload
- Hypokalemia typically accompanies metabolic alkalosis (H+ and K+ exchange at the tubule)
- Hyperkalemia accompanies metabolic acidosis (H+ moves intracellularly, K+ moves out)
11. Summary: Clinical Importance at a Glance
| Concept | Clinical Relevance |
|---|---|
| TBW distribution | Guides fluid replacement calculations |
| Na+ as primary ECF osmole | Governs volume status assessment |
| ADH/AVP | Target in SIADH, diabetes insipidus |
| RAAS | Target of ACE inhibitors, ARBs, spironolactone |
| Starling forces | Explains edema in heart failure, hypoalbuminemia, nephrotic syndrome |
| GI electrolyte losses | Guides appropriate IV fluid and electrolyte replacement |
| Hyperkalemia ECG | Cardiac arrest risk - requires emergency management |
| Osmolality formula | Detects osmolar gap (toxins, unmeasured osmoles) |
Sources:
- Current Surgical Therapy 14e - Fluid and Electrolyte Therapy
- Harrison's Principles of Internal Medicine 22E - RAAS and Edema
- Brenner & Rector's The Kidney - Hyponatremia, Hyperkalemia, Metabolic Acidosis
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Mineralocorticoids and Electrolyte Balance
- Goldman-Cecil Medicine - Fluid and Electrolyte Transport
This is a shared conversation. Sign in to Orris to start your own chat.