Tracheobronchial tree and diaphragm. Anatomy and anaesthetic, clinical importance. Viva points
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full viva-style response.
Tracheobronchial Tree and Diaphragm: Anatomy and Anaesthetic/Clinical Importance
PART 1: TRACHEOBRONCHIAL TREE
Basic Anatomy
Trachea
- Fibromuscular tube, 10-12 cm long in adults, outer diameter ~20 mm
- Begins at vertebral level C6 (continuous with the larynx/cricoid cartilage above)
- Supported by U-shaped hyaline cartilage rings - the opening of the U faces posteriorly (where the posterior wall is membranous/muscular - the trachealis muscle)
- Lies directly anterior to the oesophagus
- Bifurcates at the sternal angle (angle of Louis) / T4-T5 disc level - this point is the carina
- Half the trachea is intrathoracic, half extrathoracic
Carina
- The ridge of cartilage at the bifurcation (T4-T5 level / sternal angle)
- Highly sensitive - stimulation causes severe cough reflex and bronchospasm
- Can move superiorly up to 5 cm from its resting position
Right Main Bronchus
- Wider, shorter (~2.5 cm before first branch), more vertical (25° from vertical axis)
- Departs at ~25 degrees from tracheal axis
- Right upper lobe bronchus branches almost directly posterior (~90° from right main bronchus)
- In 10% of adults, the right upper lobe bronchus departs less than 2.5 cm from the carina
- In 2-3% of adults, the right upper lobe bronchus opens into the trachea superior to the carina (anomaly important for double-lumen tubes)
Left Main Bronchus
- Narrower, longer (~5 cm before first branch)
- More horizontal - departs at ~45 degrees from tracheal axis
Bronchioles
- ~1 mm diameter, no cartilaginous support - highest proportion of smooth muscle
- Terminal bronchiole = last generation incapable of gas exchange
Anaesthetic/Clinical Importance: Tracheobronchial Tree
| Point | Detail |
|---|---|
| ETT depth and neck movement | With neck flexion, the ETT tip moves 3.8 cm toward the carina; with extension, it moves away - "tip away, base toward" |
| Endobronchial intubation | More likely to enter the right bronchus because it is wider and more vertical |
| Foreign body aspiration | Goes to the right (erect) or either side (supine); right lower lobe most common site |
| Double-lumen tube | Right-sided DLT technically harder due to short right main bronchus and variable right upper lobe take-off |
| Paediatric angles | In children <3 years, right and left bronchial angles are approximately equal (~55°) - aspiration can go either way |
| Carina sensitivity | Lightest anaesthetic plane - touching the carina causes bucking, coughing, laryngospasm, bronchospasm |
| Airway resistance | As cross-sectional area of tracheobronchial tree increases peripherally, resistance drops from central to peripheral airways |
| Turbulent vs laminar flow | Turbulent flow at branch points (carina, lobar bronchi) - turbulence increased by high-flow rates; Reynolds number >4000 = turbulent |
| Helium-oxygen | Lower gas density → promotes laminar flow → reduces resistance in upper airway oedema/narrowing |
| Suction catheter tip | When inserted through ETT without bias, preferentially enters right bronchus - deliberately turning head left helps access left bronchus |
Viva point: "Which side does unintentional endobronchial intubation occur, and why?"
Right side - the right main bronchus is wider and departs at only 25° from vertical (vs 45° for the left). - Barash Clinical Anesthesia, 9e, p.1116
PART 2: DIAPHRAGM
Basic Anatomy
The diaphragm is a musculotendinous sheet that seals the inferior thoracic aperture. It is the principal muscle of inspiration.
Shape and Position
- Dome-shaped - balloons superiorly on both sides
- Right dome is higher than left, reaching as far as rib V (due to liver below)
- Posterior attachment is more inferior than anterior (oblique inferior thoracic aperture)
- On contraction, dome height decreases → thoracic volume increases
Origins (peripheral muscular attachments)
- Sternal part: posterior surface of xiphoid process
- Costal part: inner surfaces of ribs 7-12 and costal cartilages
- Lumbar part: crura (medial - from L1-L3 vertebral bodies) + arcuate ligaments (medial, lateral)
Central tendon: fibres converge centrally; the IVC passes through it
The Three Major Openings (High-Yield Viva Table)
| Opening | Level | Structures passing through |
|---|---|---|
| Caval hiatus | T8 | IVC, right phrenic nerve, lymphatic vessels |
| Oesophageal hiatus | T10 | Oesophagus, anterior & posterior vagal trunks, left gastric artery & vein |
| Aortic hiatus | T12 | Aorta, thoracic duct (+ occasionally azygos vein) |
Memory aid: 8, 10, 12 → I Eat Aorta / Vena cava (8) - Oesophagus (10) - Aorta (12)
Additional openings:
- Sternocostal hiatus (foramen of Morgagni): between sternal and costal fibres - lymphatics from liver pass through (site of Morgagni hernia)
- Lumbocostal triangle (Bochdalek): potential weak area posterolaterally - site of Bochdalek hernia (most common congenital diaphragmatic hernia, usually left-sided)
Why does aorta not transmit pulse pressure to diaphragm? The aorta passes posterior to the median arcuate ligament, not through the diaphragm muscle - so diaphragmatic contraction does not compress it.
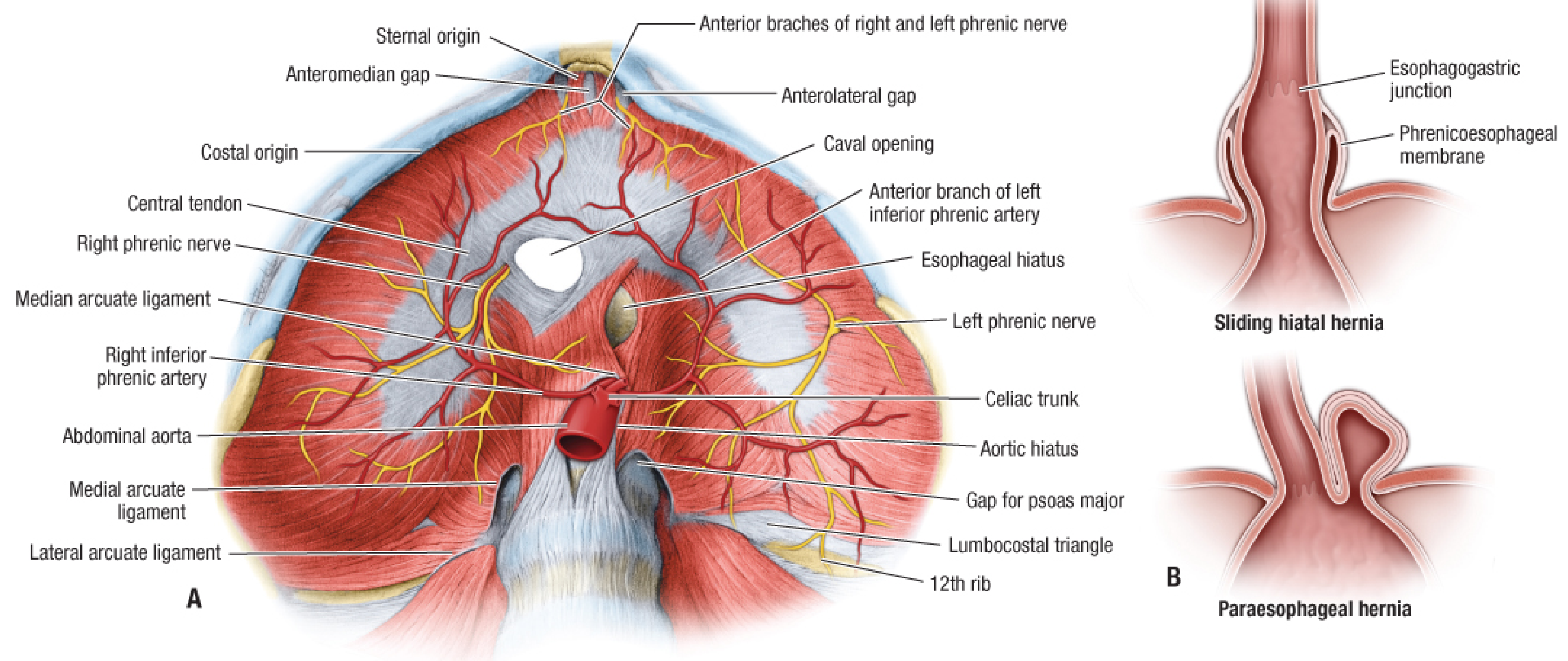
Inferior view of the diaphragm - Fischer's Mastery of Surgery, 8e
Innervation
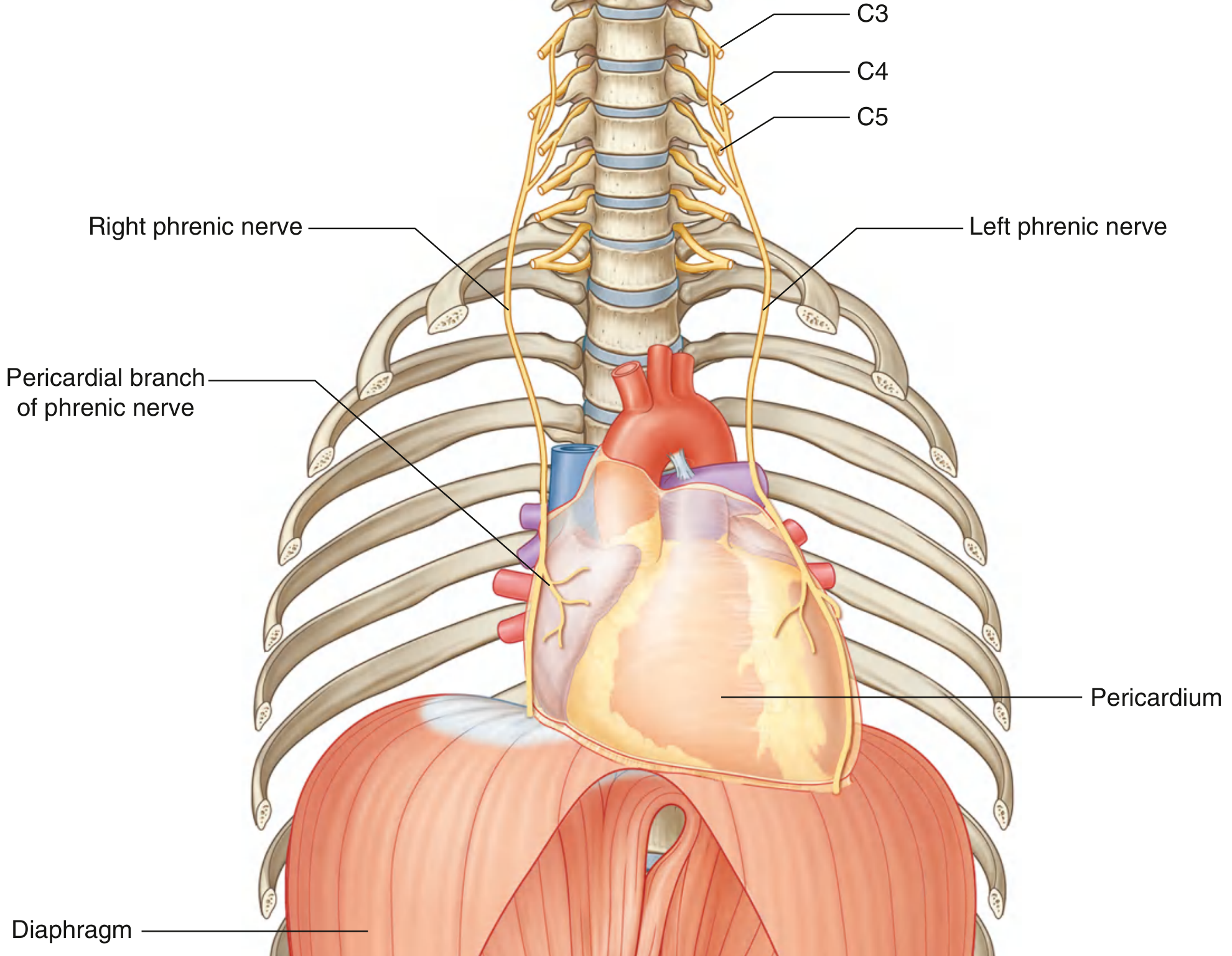
Phrenic nerve origin from C3, C4, C5 - Gray's Anatomy for Students
| Component | Detail |
|---|---|
| Motor | Entire diaphragm via phrenic nerve (C3, C4, C5 - major from C4) |
| Sensory (central) | Phrenic nerve (C3-C5) - referred pain to shoulder tip |
| Sensory (peripheral) | Lower intercostal nerves (T9-T11) |
| Course | Down anterior surface of scalenus anterior → thoracic inlet → mediastinum (anterior to lung roots) → diaphragm |
| Left phrenic | Enters muscular part of left hemidiaphragm, lateral to left cardiac surface |
| Right phrenic | Courses through the caval opening or central tendon |
Mnemonic for level: "C3, 4, 5 keeps the diaphragm alive"
Blood Supply
| Surface | Arteries | Veins |
|---|---|---|
| Superior | Superior phrenic arteries; pericardiophrenic and musculophrenic branches of internal thoracic artery | Pericardiophrenic and musculophrenic veins → IVC |
| Inferior | Inferior phrenic arteries (from abdominal aorta / celiac trunk) | Inferior phrenic veins → IVC (right) / left suprarenal vein (left) |
Lymphatics:
- Superior surface → anterior, middle, posterior phrenic nodes
- Inferior surface → phrenic nodes + aortic nodes (follow inferior phrenic vessels)
Anaesthetic/Clinical Importance: Diaphragm
| Scenario | Relevance |
|---|---|
| Spinal cord injury | Injuries at C2 and above require immediate ventilatory support. Between C3-C5, variable; below C5 diaphragm function preserved |
| Referred shoulder tip pain | Diaphragmatic irritation (blood, pus, inflammation) → pain referred to shoulder tip via C3-C4 (phrenic nerve) - e.g., ruptured ectopic, subphrenic abscess, ruptured spleen |
| Phrenic nerve palsy | Unilateral: raised hemidiaphragm, 20-25% reduced VC. Bilateral: respiratory failure requiring ventilation |
| Hiatal hernia | Sliding (commonest, 95%) vs paraesophageal - sliding type causes GORD; paraesophageal risks strangulation |
| Congenital diaphragmatic hernia (CDH) | Usually left Bochdalek hernia (gut herniates into chest) → pulmonary hypoplasia, neonatal respiratory distress - anaesthetic challenge: avoid high airway pressures, treat pulmonary hypertension |
| Diaphragm position in anaesthesia | Supine position and GA → diaphragm shifts cephalad (~4 cm), reducing FRC - especially important in obese patients, pregnant patients |
| Pneumoperitoneum (laparoscopy) | CO₂ insufflation pushes diaphragm cephalad → increased airway pressure, reduced compliance, potential basal atelectasis |
| Incisions near diaphragm | Below the 8th rib (midclavicular line) / 10th rib (midaxillary line) may enter abdominal cavity without entering pleural cavity |
| Phrenic nerve block | Occurs as a complication in ~100% of interscalene brachial plexus blocks - bilateral blocks contraindicated in severe respiratory compromise |
| Morgagni hernia | Anterior/retrosternal; Bochdalek hernia = posterior/lateral. Bochdalek more common (left > right) |
| Tracheal intubation effect | ETT and IPPV bypasses normal diaphragmatic breathing mechanics; in COPD hyperinflation flattens diaphragm → poor mechanical advantage |
QUICK VIVA SUMMARY POINTS
- Trachea begins at C6, bifurcates at T4-T5 (sternal angle / carina)
- Trachea is 10-12 cm, half intrathoracic, half extrathoracic
- Right bronchus: wider, shorter, 25° - preferred side for foreign bodies, endobronchial intubation
- ETT moves 3.8 cm toward carina on neck flexion
- Children <3 years: equal bronchial angles (~55°) - aspiration equal both sides
- Bronchioles have no cartilage - highest smooth muscle content - prone to spasm
- Carina at T4-T5; exquisitely sensitive - light anaesthesia + carina contact = bronchospasm
- Diaphragm = principal muscle of inspiration; dome-shaped; right dome higher (rib V)
- Three openings: T8 (IVC), T10 (oesophagus + vagus), T12 (aorta + thoracic duct)
- Aorta passes behind median arcuate ligament - not through muscle - no compression
- Phrenic nerve: C3, C4, C5 - motor to whole diaphragm; sensory to central part
- Peripheral diaphragm sensation: T9-T11 intercostals
- Referred shoulder tip pain from diaphragmatic irritation = via C3-C4 phrenic nerve
- Spinal injury at C2 or above = immediate ventilatory support needed
- GA + supine → diaphragm shifts cephalad ~4 cm → FRC falls
- Interscalene block → 100% ipsilateral phrenic nerve palsy - avoid bilateral blocks
Sources: Barash Clinical Anesthesia 9e, pp. 1115-1117 | Gray's Anatomy for Students | Fischer's Mastery of Surgery 8e, pp. 2589-2591 | Gray's Anatomy for Students (Innervation of Diaphragm, p. 174)
This is a shared conversation. Sign in to Orris to start your own chat.