Terbinfen
Reading File
Finding Sources
Searching the Web
terbinafine antifungal mechanism uses pharmacology
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a complete overview of Terbinafine drawn from multiple authoritative textbooks (Goodman & Gilman, Lippincott, Harrison's, Fitzpatrick's, Dermatology 5e).
Terbinafine
Drug Class & Mechanism
Terbinafine is a synthetic allylamine antifungal (brand name: Lamisil). Its mechanism is unique among antifungals:
- Inhibits squalene epoxidase (also called squalene monooxygenase), a fungal enzyme that converts squalene to squalene epoxide - an early step in ergosterol biosynthesis.
- Critically, this is not a CYP450 enzyme (unlike azoles which inhibit CYP51/lanosterol demethylase), so it has minimal impact on human sterol synthesis.
- Squalene accumulates intracellularly to toxic levels, and ergosterol is depleted - both effects contribute to fungicidal (not just fungistatic) activity, particularly against dermatophytes.
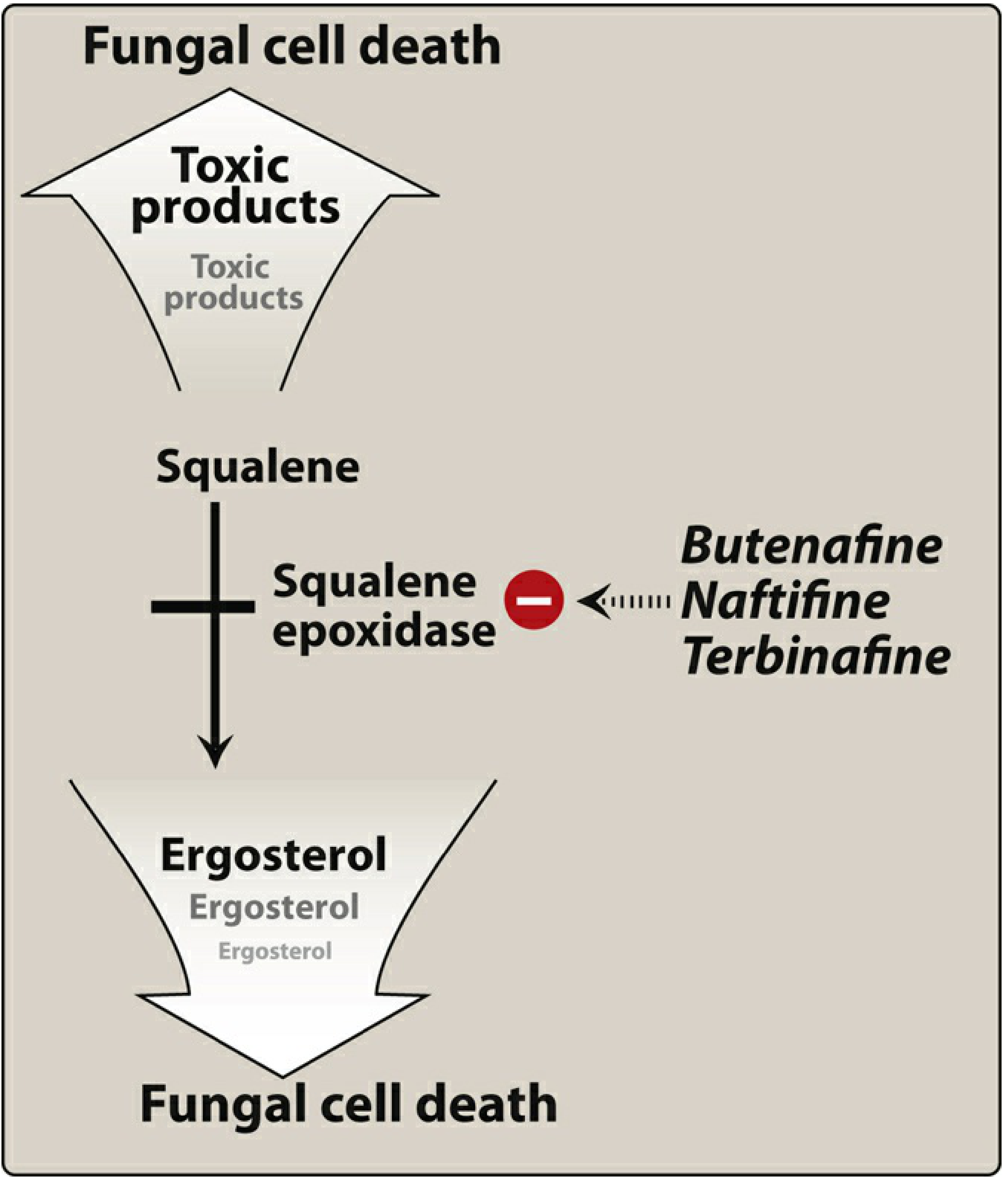
Figure: Mode of action of squalene epoxidase inhibitors (Lippincott Pharmacology)
Antifungal Spectrum
| Organism | Activity |
|---|---|
| Dermatophytes (Trichophyton, Microsporum, Epidermophyton) | Excellent (drug of choice) |
| Malassezia furfur | Active (topical) |
| Candida species | Less active; less preferred |
| Systemic fungi | Poor tissue penetration beyond skin/nails - not preferred |
Formulations & Therapeutic Uses
Oral (250 mg once daily)
- Onychomycosis (nail fungal infection) - drug of choice; more effective than itraconazole or griseofulvin for Trichophyton
- Fingernails: ~6 weeks
- Toenails: ~12 weeks
- Tinea capitis (scalp ringworm) - oral therapy required; topicals are ineffective
- Tinea corporis/cruris (off-label)
Topical (1% cream, gel, spray, solution)
- Tinea pedis (athlete's foot)
- Tinea corporis (ringworm)
- Tinea cruris (jock itch)
- Tinea versicolor (Malassezia furfur)
- Duration: typically 1 week for topical use
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Oral bioavailability | ~40% (extensive first-pass metabolism) |
| Protein binding | High; widely deposited in skin, nails, adipose tissue |
| Half-life | Initial ~12 h; extends to 200-400 hours at steady state (slow release from tissues explains persistent nail levels) |
| Metabolism | Multiple CYP450 isoenzymes |
| Excretion | Mainly urine |
| Avoid in | Moderate-severe hepatic dysfunction; moderate-severe renal impairment |
Drug Interactions
- CYP2D6 inhibitor: Terbinafine inhibits CYP2D6 and can raise levels of:
- Beta-blockers
- Tricyclic antidepressants (TCAs)
- SSRIs
- MAO inhibitors
- Type 1B antiarrhythmics
- Rifampin decreases terbinafine plasma levels
- Cimetidine increases terbinafine plasma levels
Adverse Effects
| Severity | Effect |
|---|---|
| Common | GI distress (diarrhea, dyspepsia, nausea), headache, rash |
| Notable | Taste disturbances, visual disturbances, elevated liver transaminases, lymphocyte count decrease |
| Serious (rare) | Hepatotoxicity (including fatal cases), severe neutropenia, Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), AGEP, subacute cutaneous lupus erythematosus, exacerbation of psoriasis |
- Pregnancy: Systemic therapy should be postponed until after delivery.
- Topical formulations are well tolerated with minimal systemic effects.
Key Comparisons
| Feature | Terbinafine | Azoles (e.g. itraconazole) |
|---|---|---|
| Mechanism | Squalene epoxidase | CYP51 (lanosterol 14α-demethylase) |
| Action | Fungicidal (dermatophytes) | Fungistatic |
| Onychomycosis efficacy | Superior | Good |
| CYP involvement | Not target enzyme; inhibits CYP2D6 | Target is CYP51; many CYP interactions |
| Systemic mycoses | Not preferred | Yes (e.g. itraconazole) |
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1224
- Lippincott Illustrated Reviews: Pharmacology, p. 1098-1099
- Harrison's Principles of Internal Medicine 22E (2025)
- Fitzpatrick's Dermatology, 9e
- Dermatology 5e (Elsevier)
Clotramozol
Finding Sources
Searching the Web
clotrimazole antifungal mechanism uses pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a complete overview of Clotrimazole drawn from multiple authoritative textbooks (Goodman & Gilman, Lippincott, Fitzpatrick's Dermatology, Katzung, Goldman-Cecil, Harrison's).
Clotrimazole
Drug Class
Clotrimazole is a synthetic imidazole antifungal - the first topical imidazole ever developed. Trade names include Lotrimin, Mycelex, and Canesten. It is on the WHO List of Essential Medicines.
Mechanism of Action
Clotrimazole works through two complementary effects:
-
Primary - Ergosterol synthesis inhibition: Like all azoles, it inhibits lanosterol 14α-demethylase (CYP51), a fungal cytochrome P450 enzyme that converts lanosterol to ergosterol. This depletes ergosterol, disrupts cell membrane integrity, and allows accumulation of toxic 14α-methylated sterol precursors.
-
Additional membrane effects: Clotrimazole specifically disrupts mycotic phospholipids, causing leakage of intracellular iron, degradation of nucleic acids, and suppression of cell respiration.
At normal concentrations it is fungistatic; at higher concentrations it becomes fungicidal through direct membrane damage. - Fitzpatrick's Dermatology, p. 4292-4301
Antifungal Spectrum
| Organism Group | Examples | Activity |
|---|---|---|
| Dermatophytes | Trichophyton, Microsporum, Epidermophyton | High |
| Yeasts | Candida albicans, other Candida spp. | High |
| Malassezia furfur | (tinea versicolor) | Active |
| Gram-positive bacteria | - | Some activity |
Formulations & Therapeutic Uses
Topical Skin (1% cream, lotion, spray, powder, solution)
Applied twice daily for 2-6 weeks:
- Tinea corporis (ringworm)
- Tinea pedis (athlete's foot)
- Tinea cruris (jock itch)
- Tinea versicolor
- Cutaneous candidiasis
Cure rates: 60-100% in dermatophytosis, 80-100% in cutaneous candidiasis.
Vaginal (1% or 2% cream; 100 mg, 200 mg, 500 mg tablets/suppositories)
For vulvovaginal candidiasis:
- 100 mg tablet once daily for 7 days
- 200 mg tablet daily for 3 days
- 500 mg single-dose tablet (once only)
- 2% cream x 3 days, or 1% cream x 7 days
Oral Troche/Lozenge (10 mg)
For oropharyngeal candidiasis only:
- Dissolved slowly in the mouth 5 times daily for 14 days
- This is considered topical therapy - activity is entirely local; no systemic absorption
- Also a first-line option for mild thrush (alongside nystatin), per Goldman-Cecil Medicine
Combination Product
- Clotrimazole + Betamethasone dipropionate (Lotrisone cream) - for tinea corporis, tinea cruris, and tinea pedis when inflammation is prominent
Pharmacokinetics
| Route | Absorption |
|---|---|
| Skin (topical) | < 0.5% - negligible |
| Vaginal | 3-10% absorbed systemically |
| Oral troche | Local effect only; no significant systemic levels |
- Fungicidal concentrations remain in the vagina for up to 3 days after a single application.
- Not used systemically (oral tablet form was abandoned due to poor systemic profile and hepatotoxicity).
Adverse Effects
| Route | Side Effects |
|---|---|
| Topical skin | Stinging, erythema, edema, vesication, pruritus, urticaria, contact dermatitis (rare) |
| Vaginal | Burning sensation (~1.6%), lower abdominal cramps, urinary frequency; partner may experience penile/urethral irritation |
| Oral troche | GI irritation (~5% of patients) |
- Pregnancy Category B - topical and vaginal use is considered safe in pregnancy; no evidence of fetal harm from vaginal use.
Key Comparisons: Clotrimazole vs. Other Antifungals
| Feature | Clotrimazole | Terbinafine | Fluconazole |
|---|---|---|---|
| Class | Imidazole (azole) | Allylamine | Triazole (azole) |
| Target | CYP51 (lanosterol demethylase) | Squalene epoxidase | CYP51 |
| Action | Fungistatic (fungicidal at high conc.) | Fungicidal | Fungistatic |
| Route | Topical / vaginal / oral troche only | Topical + oral systemic | Oral systemic (+ topical) |
| Onychomycosis | Topical - usually not effective | Drug of choice (oral) | Alternative |
| Systemic use | No | No (not preferred) | Yes |
| Pregnancy | Category B (safe topically) | Avoid systemic | Caution |
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1225-1226
- Lippincott Illustrated Reviews: Pharmacology, p. 1102
- Fitzpatrick's Dermatology 9e, p. 4291-4313
- Katzung's Basic & Clinical Pharmacology 16e, p. 1195-1208
- Goldman-Cecil Medicine (Candidiasis chapter)
- Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.