How to know person has vertigo
Reading File
Finding Sources
Searching PubMed
vertigo diagnosis clinical assessment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough, evidence-based guide to recognizing vertigo in a person.
How to Know if a Person Has Vertigo
1. What is Vertigo?
Vertigo is a perceived sensation of spinning or motion when none is actually occurring - either the person feels they are spinning, or the world around them seems to spin. It is the most common type of dizziness. True vertigo always originates from a problem in the vestibular system (inner ear or brainstem/cerebellum). - Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
2. Key Symptoms (What the Person Reports)
Ask the person to describe their dizziness carefully. Vertigo specifically presents as:
| Symptom | Details |
|---|---|
| Spinning sensation | Feeling of rotating or moving, or environment rotating around them |
| Triggered/worsened by head movement | Turning in bed, looking up at a shelf, quick head turns |
| Nausea and vomiting | Common accompaniment |
| Tinnitus | Ringing in the ear (suggests Meniere disease) |
| Hearing loss | If present, points toward inner ear cause |
| Imbalance/unsteadiness | Mild-moderate in inner ear disease; severe in brainstem/cerebellar disease |
Important distinction: Ask whether head movement triggers the vertigo (starts it from nothing) or just makes it worse. If triggered, Benign Paroxysmal Positional Vertigo (BPPV) is the most likely cause.
3. Duration Pattern - Narrows the Diagnosis
The duration of each episode is one of the most useful clues. - Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
| Episode Duration | Likely Cause |
|---|---|
| Seconds to < 1 minute, triggered by head position | BPPV (most common cause of vertigo overall) |
| Minutes to hours, spontaneous | TIA, Vestibular migraine, Meniere disease |
| Continuous for days, worsened by motion | Vestibular neuritis, Brainstem stroke |
4. Physical Examination Findings
A clinician looking for vertigo performs these tests:
a. Neurological Exam (Rule out Central/Dangerous Causes First)
Check for signs of brainstem or cerebellar disease:
- Dysarthria (slurred speech), diplopia (double vision), facial weakness
- Abnormal gait or inability to tandem walk
- Finger-to-nose incoordination (dysmetria)
- Romberg test (instability when standing with eyes closed)
- Cranial nerve palsies
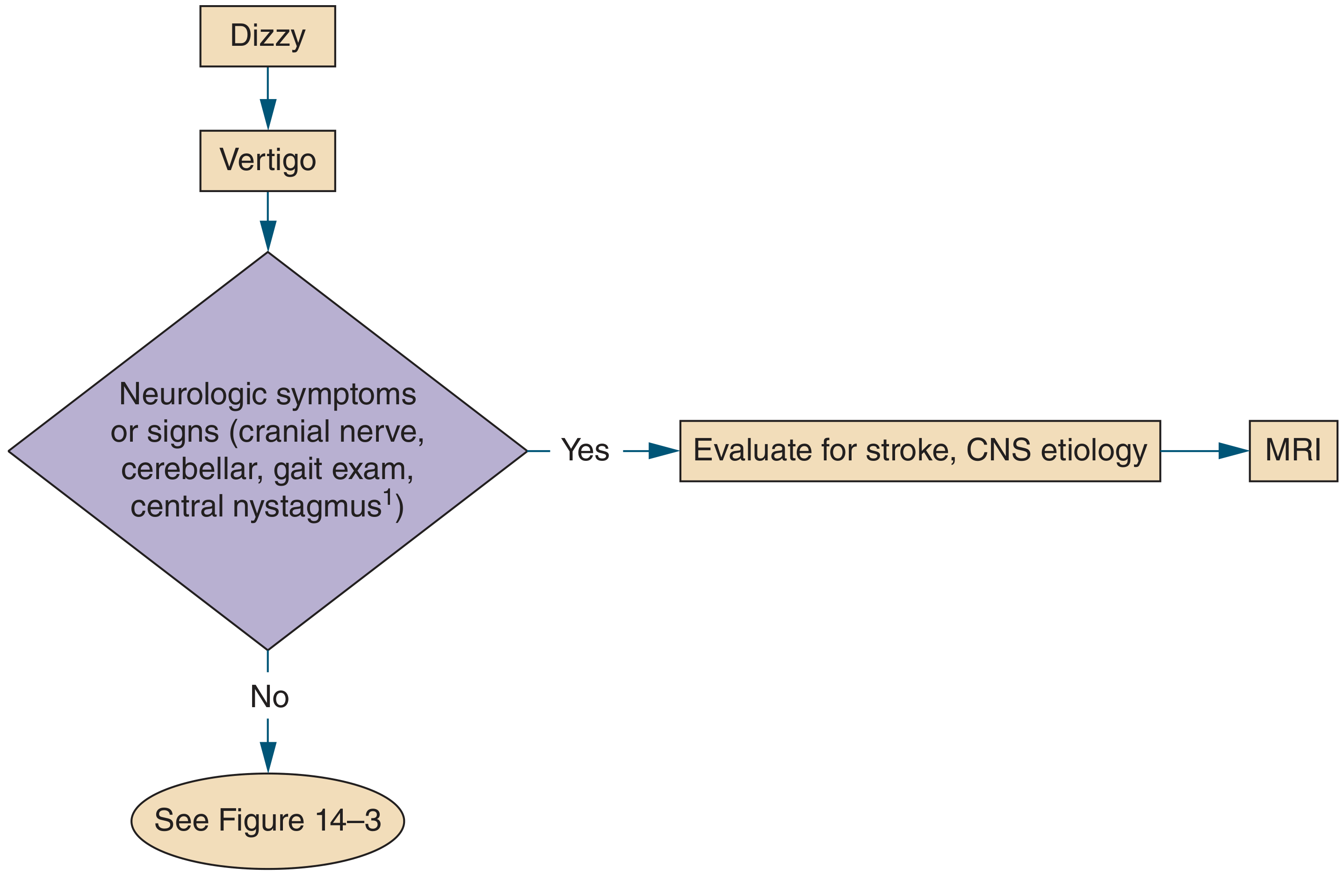
b. Nystagmus Assessment
Nystagmus (involuntary eye movements) is a hallmark finding. The pattern helps distinguish the cause:
| Nystagmus Feature | Peripheral (Inner Ear) | Central (Brain) |
|---|---|---|
| Direction | Unidirectional | May change direction (bidirectional) |
| Suppression by visual fixation | Yes - inhibited | No - persists |
| Duration | < 1 minute, fatigues | > 1 minute, does not fatigue |
| Vertical nystagmus | Absent | Present (central only) |
c. Dix-Hallpike Maneuver
- The most important test for BPPV
- The clinician rapidly moves the patient from sitting to lying with head turned 45 degrees to one side
- A positive result = brief burst of nystagmus + vertigo after a few seconds' delay, lasting < 1 minute, that fatigues on repetition
- This confirms BPPV with high accuracy
d. HINTS Plus Exam (for continuous vertigo lasting days)
Used to distinguish a dangerous stroke from benign vestibular neuritis:
- Head Impulse Test - Inspect Nystagmus - Test of Skew
- Plus: hearing test
- A normal head impulse test + direction-changing nystagmus = high suspicion for stroke
e. Additional Bedside Tests
- Romberg test - stand with feet together, eyes closed; excessive sway = abnormal
- Tuning fork tests (Weber, Rinne) - detect sensorineural vs conductive hearing loss
- Orthostatic blood pressure - to rule out presyncope masquerading as vertigo
- Pneumatic otoscopy - pressure in the ear canal triggers vertigo in perilymph fistula
5. Peripheral vs. Central Vertigo - Key Comparison
| Feature | Peripheral (inner ear) | Central (brainstem/brain) |
|---|---|---|
| CNS symptoms (headache, dysarthria, diplopia) | Rare | Common |
| Imbalance severity | Mild to moderate | Severe - cannot walk |
| Nystagmus | Inhibited by fixation, unidirectional, fatigues | Not inhibited, may change direction, persists |
| Onset | Episodic | Often continuous |
- Textbook of Family Medicine, 9th Ed.
6. Tests and Investigations
| Test | When Used |
|---|---|
| MRI brain | Any CNS symptoms, or vertigo unresponsive to treatment; detects stroke, MS, tumors |
| Audiogram | Assess hearing if no clear cause after history and exam |
| Electronystagmography (ENG) | Objective vestibular testing; locates a lesion via caloric testing and positional maneuvers |
| Blood tests | CBC, B12, folate, RPR, drug screens - for specific systemic causes |
7. Red Flag Symptoms - Seek Urgent Evaluation
These features suggest a central (dangerous) cause like stroke and need immediate MRI:
- New severe headache or neck pain
- Double vision, slurred speech, facial drooping
- Severe imbalance - cannot walk without falling
- Vertigo that is constant and does not fatigue
- First-ever vertigo in a person with cardiovascular risk factors
Bottom line: Vertigo is recognized by the characteristic spinning sensation, its relationship to head movement, and the presence of nystagmus on exam. The Dix-Hallpike maneuver confirms BPPV (the most common cause), while the neurological exam and nystagmus pattern screen for dangerous central causes requiring MRI. - Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.; Textbook of Family Medicine, 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.