Charcot’s joint
Reading File
Finding Sources
Searching PubMed
"Charcot joint" OR "neuropathic arthropathy"
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, well-illustrated answer.
Charcot's Joint (Neuropathic Arthropathy)
Definition: Charcot's joint - also called neuropathic arthropathy - is a progressive, destructive joint disease that occurs in the setting of peripheral sensory and/or autonomic neuropathy. It is characterized by bone fragmentation, joint subluxation/dislocation, and a consolidating deformity that can threaten both function and limb viability. Jean-Martin Charcot first described it in 1868 in the context of tabes dorsalis.
Etiology / Causes
The leading cause today is diabetes mellitus. Other conditions include:
| Category | Examples |
|---|---|
| Infections | Syphilis (tabes dorsalis), leprosy, yaws |
| Congenital | Congenital insensitivity to pain, spina bifida, myelomeningocele |
| Spinal cord | Syringomyelia, spinal cord injury |
| Peripheral nerve | Alcoholic neuropathy, avitaminosis, amyloid neuropathy, peripheral nerve injury |
| Iatrogenic | Repeated intraarticular steroid injections, postrenal transplant arthropathy |
Syphilis is an infrequent but increasingly recognized cause because inadequate treatment of primary/secondary syphilis or antibiotic exposure for unrelated infections can mask classic signs - a high index of suspicion and appropriate serologic testing are required.
Pathogenesis
The exact etiology is multifactorial. Two classic theories have been proposed:
1. Neurovascular (French) theory - originally proposed by Charcot: neurologic damage causes autonomic dysfunction → increased local blood flow via arteriovenous shunting → bone resorption. This theory emphasizes the role of neurogenic vasodilation.
2. Neurotraumatic (German) theory - supported by Virchow and Volkman: neuropathy abolishes protective reflexes and proprioception → repetitive unrecognized microtrauma → progressive joint destruction. Joint tissue mechanoreceptors and nociceptors normally form a reflex arc to surrounding muscles to maintain stability; this is disrupted by neuropathy.
Current understanding: Pathogenesis is likely a combination of both. The inflammatory cascade has been increasingly emphasized: joint insult triggers inflammatory cytokines → increased osteoclastogenesis → progressive bone loss → further fractures and potentiation of inflammation. Histology of Charcot bone shows inflammatory myxoid infiltration, decreased trabeculae, and disorganized trabecular patterns compared with diabetic controls.
Joint Distribution
- Diabetes: Preferentially involves the small joints of the foot - especially the tarsometatarsal (Lisfranc) joints. Unlike syphilitic Charcot, the large weight-bearing joints are less commonly affected.
- Syphilis/tabes dorsalis: Classically affects large weight-bearing joints - knee (most common in tabes), hip, ankle.
- Syringomyelia: Typically affects upper limb joints (shoulder, elbow).
Anatomic Classification (Brodsky - Foot & Ankle)
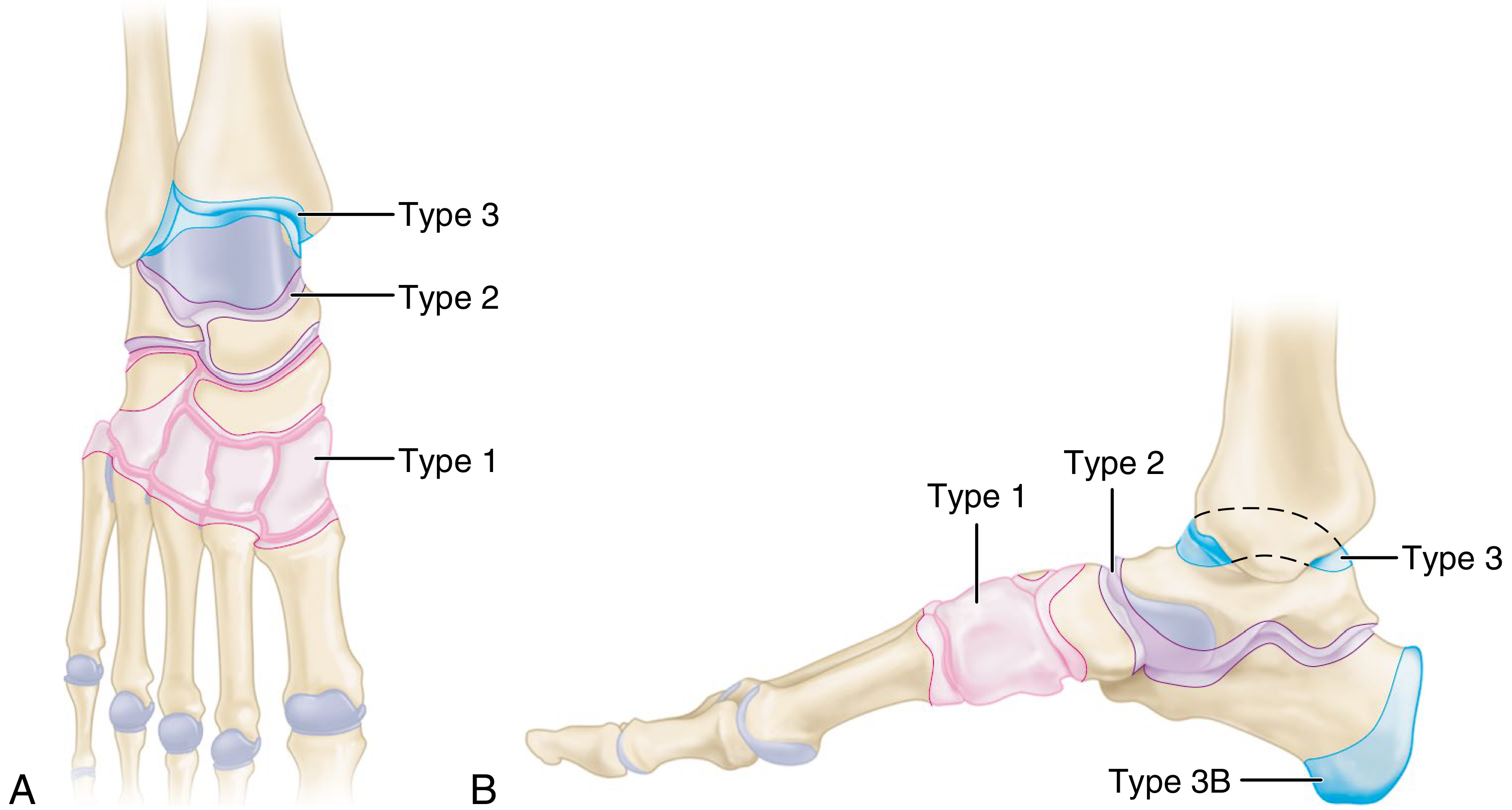
| Type | Location | Frequency | Key Features |
|---|---|---|---|
| 1 | Tarsometatarsal + naviculocuneiform joints (midfoot) | 60% | Most common; hindfoot valgus, forefoot abduction; risk of "rocker-bottom" deformity |
| 2 | Hindfoot (subtalar, talonavicular, calcaneocuboid) | 25% | Marked varus/valgus hindfoot; may progress to rocker-bottom from plantar flexion of talar head |
| 3A | Ankle joint | 10% | Ulcers over prominent malleoli; marked instability - usually requires surgery |
| 3B | Calcaneal tuberosity | 5% | Pathologic avulsion fracture |
The medial column of the foot fails before the lateral column due to the pull of the posterior tibial tendon. Sagittal plane deformities are more likely to cause ulceration than transverse plane abnormalities.
Eichenholtz Staging (Disease Stage Classification)
| Stage | Name | Clinical Features | Radiographic Features |
|---|---|---|---|
| 0 (prodromal) | Inflammatory | Erythema, warmth, swelling; no radiographic changes | Normal X-ray; MRI/bone scan may show edema |
| 1 | Development/Fragmentation | Acute hot swollen foot; patient often continues walking | Periarticular fragmentation, subluxation, joint debris |
| 2 | Coalescence | Swelling begins to decrease | Bone resorption decreases; early sclerosis; fragments begin to coalesce |
| 3 | Reconstruction/Consolidation | Minimal warmth; deformity has stabilized | Dense sclerosis, consolidation, residual deformity |
Some authors have questioned the validity of the Eichenholtz classification and prefer MRI or PET/CT-based systems to detect Stage 0 changes missed on plain radiographs.
Clinical Features
- The classic presentation is a warm, swollen, erythematous foot in a diabetic patient - often mistaken for cellulitis or gout
- Pain is typically disproportionately mild relative to the degree of destruction due to sensory neuropathy
- The patient may continue weight-bearing, accelerating destruction
- Skin temperature difference >2°C between feet is a clinical clue
- Associated foot ulcers and autonomic impairment are common
Radiographic features (hip example):

Key radiographic findings: rapid joint destruction, bone fragmentation, periarticular debris ("bag of bones"), subluxation/dislocation, new bone formation, and sclerosis. Charcot of the hip shows fragmentation of the femoral head and acetabular dome with subluxation.
Histology: Osteochondral fragments embedded within the synovium - this is considered diagnostic of neuropathic arthropathy on biopsy.
Diagnosis
- Clinical: Warm, swollen, relatively painless foot in a neuropathic patient
- Plain radiographs: Fragmentation, subluxation, debris - but may be normal in Stage 0
- MRI: Best for early detection (Stage 0) - periarticular edema, occult fractures
- Bone scan (Tc-99m): Increased uptake; used when MRI contraindicated
- PET/CT: Useful for early stages and differentiating from osteomyelitis
- Serology: If syphilis suspected (RPR/VDRL, confirmatory FTA-ABS)
- Histology: Osteochondral fragments in synovium is diagnostic
Key diagnostic challenge: Distinguishing Charcot from osteomyelitis - both cause bone destruction in diabetic feet. MRI signal patterns and clinical context help, but sometimes indistinguishable without biopsy.
Treatment
Nonoperative (Eichenholtz-guided)
- Stage 1 (Active/Fragmentation): Total contact cast (TCC) or orthosis - offloads the region and maintains alignment through healing. This is the cornerstone of management.
- Stage 2 (Coalescence): Transition to prefabricated boot or custom-molded ankle-foot orthosis (AFO) as radiographic signs of healing appear.
- Stage 3 (Consolidation): Accommodative shoe with molded orthosis once swelling completely resolves.
Additional medical measures:
- Glycemic optimization (poor glucose control worsens bone quality)
- Vitamin D supplementation (hypovitaminosis D is common in diabetic patients and plays a role in pathogenesis)
- Bisphosphonates and calcitonin have shown limited effectiveness and are not current standard of care
- Patients should be counseled that up to 50% may still require surgical intervention despite intensive conservative treatment
Operative
Traditionally avoided due to high risks (infection, nonunion, delayed healing). However, over the past decade operative management has increased with improvements in glycemic control and fixation techniques.
Indications for surgery:
- Instability with soft-tissue compromise
- Ulceration that cannot be off-loaded
- Failed conservative management (particularly Type 3A ankle involvement)
- Limb-threatening deformity
Hip: Total joint arthroplasty is rarely indicated - recurrent dislocation and loosening are frequent complications. Surgery is reserved for severe disability only.
Principles: Maintain a plantigrade foot with closed soft-tissue envelope able to withstand weight-bearing. Many surgeons prefer to delay surgery until the inflammatory phase resolves because bone quality is poor during active inflammation.
Key Points for Exams
| Feature | Detail |
|---|---|
| First described by | Charcot (1868), in tabes dorsalis |
| Commonest cause today | Diabetes mellitus |
| Classic mnemonic (D's) | Diabetes, Destruction, Dislocation, Dense bones (sclerosis), Debris |
| Radiologic hallmark | "Bag of bones" - fragmentation, sclerosis, debris, subluxation |
| Histologic finding | Osteochondral fragments in synovium (diagnostic) |
| Foot type most common | Type 1 - tarsometatarsal (Lisfranc) - 60% |
| Syphilis vs. DM joints | Syphilis: large joints (knee, hip); DM: small foot joints |
| Stage 0 best seen on | MRI |
| Conservative mainstay | Total contact cast |
| Up to 50% eventually need | Surgical intervention |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, pp. 465 and 5068-5073; Bradley and Daroff's Neurology in Clinical Practice, p. 2685; Goldman-Cecil Medicine.
SICKLE CELL ANEMIA IN ORTHOPAEDICS
Finding Sources
Finding Sources
Searching PubMed
"sickle cell disease" AND osteonecrosis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-illustrated material from multiple authoritative sources. Let me compile the full answer.
Sickle Cell Anemia in Orthopaedics
Sickle cell disease (HbSS) produces a wide range of musculoskeletal complications driven by two main mechanisms: vaso-occlusion (causing infarction) and haemolysis (causing chronic anaemia and compensatory marrow expansion). Bone pain is the most common reason for hospital admission in sickle cell patients.
Pathophysiological Basis
| Mechanism | Orthopaedic Consequence |
|---|---|
| Vaso-occlusion / sickling crisis | Bone infarcts, bone marrow infarcts, avascular necrosis, joint effusions |
| Marrow hyperplasia (compensatory) | Medullary expansion, cortical thinning, coarse trabeculations, osteopenia |
| Splenic dysfunction (functional asplenia) | Predisposition to osteomyelitis and septic arthritis |
| Chronic haemolysis | Hyperuricaemia → gout; anaemia |
| Growth plate infarction | Limb length discrepancy, growth failure |
Complete Orthopaedic Manifestations of Sickle Cell Disease
1. Sickle Cell Dactylitis (Hand-Foot Syndrome)
- Age: Children under 5 years; rarely seen after age 5
- Pathology: Infarction of bone marrow and cortical bone of the small tubular bones → periostitis and soft tissue swelling
- Clinical: Diffuse, painful swelling, tenderness and warmth of the hands and feet lasting 1-3 weeks
- Radiographs: Periosteal elevation, subperiosteal new bone formation, areas of radiolucency and increased density in metacarpals, metatarsals, and proximal phalanges - "moth-eaten" appearance

- Prognosis: Resolves in weeks with little or no residual damage; also seen in sickle cell thalassemia
2. Bone Infarction (Vaso-occlusive Crisis)
- Mechanism: Sickling of red cells → vascular occlusion → sterile infarction of bone cortex and marrow
- Presentation: Periarticular and long bone pain; warm tender joints; knees and elbows most often affected; joint effusions (usually non-inflammatory unless synovial infarction occurs)
- Radiographic features: Periosteal elevation, irregular cortical thickening, bone marrow lysis → fibrosis → new bone formation
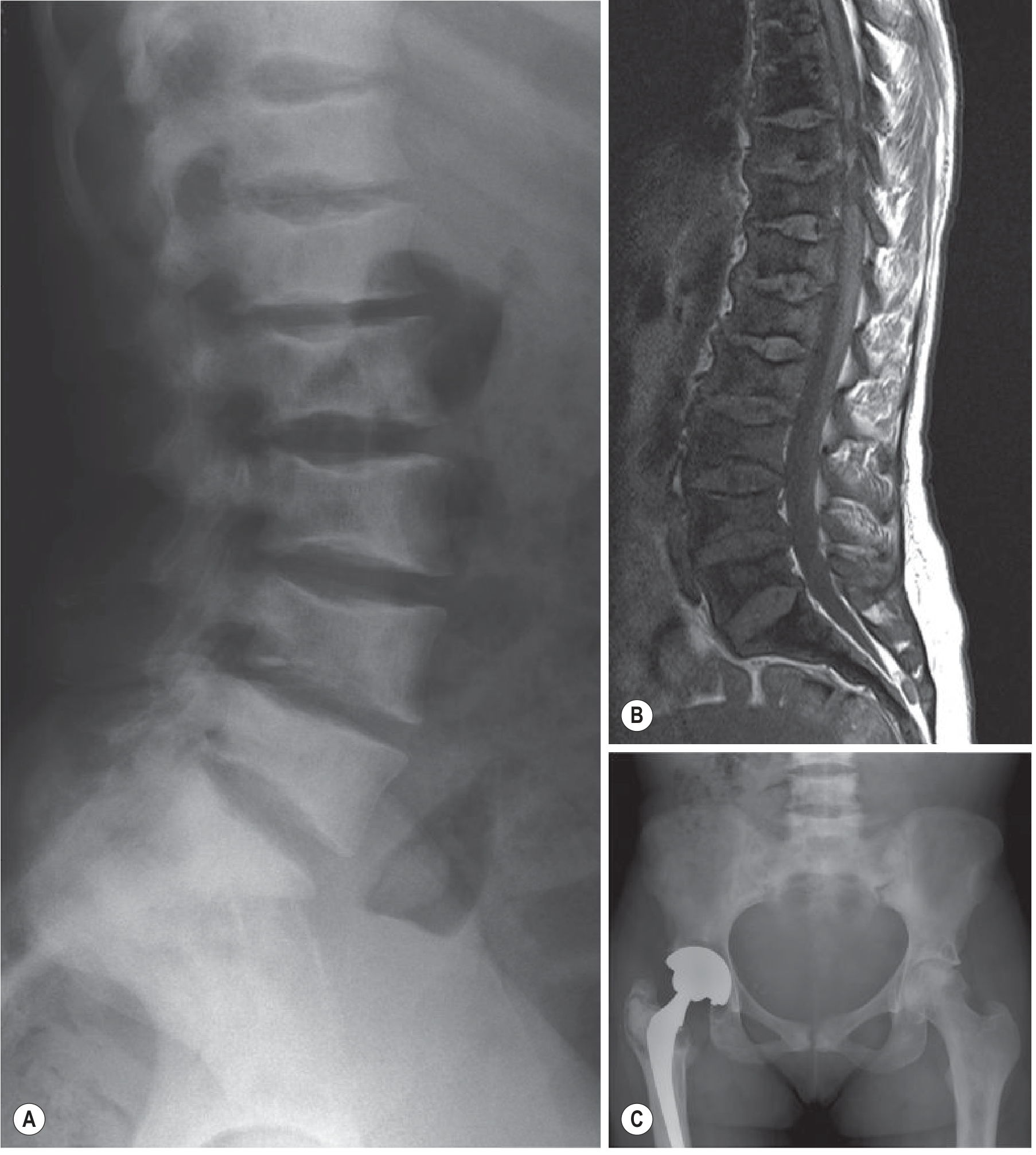
- Special variant - Vertebral infarction: Infarction of vertebral end plates → central depression of the endplate while periphery remains elevated = "H-shaped" or "cod-fish" vertebrae - pathognomonic of sickle cell disease
- Children: Epiphyseal growth plate infarction can cause growth disturbance and limb length discrepancy
3. Osteomyelitis
- Incidence: Significantly elevated due to functional asplenia (splenic infarction → impaired opsonization of encapsulated organisms)
- Most common organism: Salmonella species - isolated in up to 70% of cases in sickle cell osteomyelitis; this is the classic high-yield exam fact (contrast with the general population where Staphylococcus aureus is most common)
- S. aureus and Streptococcus also occur
- Most common site: Diaphysis of long tubular bones (unlike typical haematogenous osteomyelitis which preferentially affects metaphysis)
- Radiographs: Periosteal elevation → cortical disruption
Critical diagnostic challenge: The clinical and radiological features of osteomyelitis and bone infarction in sickle cell disease are nearly identical - both cause pain, swelling, fever, elevated inflammatory markers, and periosteal changes. No single test reliably differentiates them. The presence of a cortical break or periosteal collection favors infection. Empiric antibiotic therapy should be started when diagnosis is uncertain.
4. Avascular Necrosis (Osteonecrosis)
This is the most orthopaedically significant complication of sickle cell disease.
- Incidence: ~5% of patients develop AVN of the femoral head; significantly higher in HbSS + HbS-alpha thalassemia
- Sites affected (in order of frequency):
- Femoral head (most common)
- Humeral head
- Distal femur
- Tibial condyles
- Vertebral bodies, distal radius, other juxtaarticular sites
- Mechanism: Vaso-occlusion → ischaemia of subchondral bone → death of bone → subchondral collapse
Ficat & Arlet Staging (Femoral Head)
| Stage | Radiograph | MRI/Bone Scan | Symptoms |
|---|---|---|---|
| 0 | Normal | Normal | None |
| 1 | Normal | Abnormal (edema on MRI; increased uptake on bone scan) | Initiating |
| 2 | Cystic / sclerotic changes | Abnormal | Yes |
| 3 | Crescent sign (subchondral fracture); joint space preserved | Abnormal | Yes |
| 4 | Femoral head collapse; joint space lost | Abnormal | Severe |
The crescent sign represents a subchondral fracture with separation of articular cartilage from necrotic bone - pathognomonic of Stage 3 AVN.
- Natural history: The vast majority of untreated patients with AVN progress to femoral head collapse within 5 years; symptoms nearly always precede collapse
- Imaging: MRI is far more sensitive than plain radiograph for early detection
Treatment of AVN in Sickle Cell Disease
| Stage | Treatment |
|---|---|
| Early (Stages 0-2) | Core decompression (± bone grafting); reduces intraosseous pressure, may prevent collapse |
| Stage 3 | Vascularized fibular grafting; osteotomy; core decompression with stem cells |
| Stage 4 (collapse) | Total hip arthroplasty (THA) |
THA in sickle cell disease - important caveats:
- Associated with higher rates of orthopaedic and medical complications in most studies
- Early prosthetic loosening is a recognized complication - mechanism is extended bone infarct disease causing poor bone stock
- Higher risk of periprosthetic joint infection (PJI) due to underlying immunodeficiency
- Structural bone disease makes joint replacement technically challenging
- Pre-operative exchange transfusion to raise HbA levels and reduce HbS <30% is generally recommended perioperatively
5. Septic Arthritis
- Prevalence: ~3% of adults with sickle cell disease develop septic arthritis
- Most commonly affected joint: Hip (36/59 infections in one large series)
- Organisms: S. aureus and gram-negative organisms most common; Salmonella less commonly causes septic arthritis than osteomyelitis
- Diagnosis triggers: WBC >15,000/mm³, ESR >24 mm/hr, CRP >20 mg/L in context of fever and joint pain
- Source: More often distant osteomyelitis via bacteraemia rather than contiguous spread
- When epiphysis is infarcted during crisis, joint effusion develops that is clinically indistinguishable from septic arthritis → diagnostic arthrocentesis is mandatory
6. Bone Changes from Marrow Hyperplasia
Compensatory erythroid hyperplasia to offset haemolysis causes expansion of the marrow cavity:
- Widening of medullary cavities with thinning of cortices
- Coarse trabeculations throughout skeleton
- Central cupping of vertebral bodies
- In normal individuals red marrow is in the axial skeleton; in sickle cell disease it extends to long bones, tarsals, and carpals
- Vertebral compression → dorsal kyphosis
- Protrusio acetabuli from softening of the acetabulum
- In the skull: widening of diploic spaces (though less dramatic than thalassaemia)
7. Osteopenia and Osteoporosis
- Common in HbSS, especially as marrow hyperplasia competes with normal bone remodeling
- Lumbar spine is the most commonly affected site
- Low BMI and low vitamin D levels are consistent correlates
- Delayed skeletal maturation and puberty (by 12-24 months) in children
8. Growth Disturbance
- Majority of children with sickle cell disease show growth declines vs. peers
- Epiphyseal infarction in children can cause leg length discrepancy
- Delayed puberty and skeletal maturation are common
9. Gouty Arthritis
- Up to 40% of sickle cell patients are hyperuricaemic - due to increased urate generation from haemolysis + interstitial renal disease
- Attacks may be polyarticular
- Diagnostic arthrocentesis required to distinguish from septic arthritis or synovial infarction
Key Radiological Features Summary
| Finding | Significance |
|---|---|
| "H-shaped" / "Cod-fish" vertebrae | Vertebral end-plate infarction - pathognomonic |
| Crescent sign at femoral head | Stage 3 AVN - subchondral fracture |
| Periosteal elevation + cortical disruption | Osteomyelitis vs. bone infarct (overlap) |
| "Moth-eaten" metacarpals/phalanges in child | Sickle cell dactylitis |
| Medullary widening + thin cortices | Marrow hyperplasia |
| Generalized increased bone density | Chronic infarction and sclerosis |
Perioperative Considerations in Sickle Cell Disease
Any surgical procedure in a sickle cell patient carries elevated risk. Key principles:
| Factor | Consideration |
|---|---|
| Pre-op transfusion | Exchange transfusion to reduce HbS to <30%, raise HbA |
| Anaesthesia | Avoid hypothermia, hypoxia, acidosis, dehydration - all precipitate sickling |
| Tourniquet use | Controversial/avoid - tourniquets cause local hypoxia and stasis, precipitating sickling distal to tourniquet |
| Infection risk | Prophylactic antibiotics; high index of suspicion for PJI post-arthroplasty |
| Bone quality | Expect poor bone stock from infarcts; cementless fixation may have higher loosening rates |
High-Yield Summary for Exams
| Topic | Key Fact |
|---|---|
| Commonest cause of osteomyelitis | Salmonella spp. (in sickle cell) |
| Most common site of osteomyelitis | Diaphysis of long bones |
| Most common site of AVN | Femoral head |
| Pathognomonic vertebral sign | "H-shaped" or cod-fish vertebrae |
| Dactylitis occurs in | Children <5 years |
| AVN natural history | Most progress to femoral head collapse within 5 years |
| Key perioperative measure | Exchange transfusion; avoid tourniquet, hypothermia, hypoxia |
| THA complication in sickle cell | Early loosening (bone infarct), higher PJI risk |
| Septic arthritis vs. crisis | Arthrocentesis mandatory - cannot be clinically distinguished |
| Hyperuricaemia prevalence | Up to 40% → gout possible |
Sources: Harrison's Principles of Internal Medicine 22nd Ed 2025, pp. 3011-3012; Firestein & Kelley's Textbook of Rheumatology, pp. 2784-2898; Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed, pp. 48, 464; Grainger & Allison's Diagnostic Radiology, pp. 1915-1916.
Acetabula’s fracture undisplaced
Finding Sources
Finding Sources
Searching PubMed
"acetabular fracture" AND "nonoperative" AND management
Reading File
Reading File
Reading Article
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I have now gathered comprehensive material from both Rockwood & Green 2025 and Campbell's 2026 on undisplaced/nonoperative acetabular fracture management. Let me compile the full answer.
Undisplaced Acetabular Fractures - Assessment & Nonoperative Management
Background
Acetabular fractures occur when force transmitted through the femoral head is sufficient to fracture the articular surface. The overall goal of treatment - operative or nonoperative - is identical: achieve and maintain a stable, concentric (congruent) relationship between the femoral head and the weight-bearing dome of the acetabulum until bony healing.
The landmark work of Judet, Judet, and Letournel (1964) established that outcomes are primarily determined by:
- Whether the weight-bearing dome is involved
- The degree of articular displacement (threshold: <2 mm = acceptable)
- Whether the hip is stable and congruent
Classification - Letournel System (The International Standard)
5 Elementary Types
| Type | Description |
|---|---|
| Posterior wall | Fracture of the articular surface of the posterior column only |
| Posterior column | Entire posterior column separated from innominate |
| Anterior wall | Articular surface of anterior column only |
| Anterior column | Entire anterior column separated |
| Transverse | Single fracture line traversing both anterior and posterior columns |
5 Associated Types
| Type | Components |
|---|---|
| Posterior column + posterior wall | Combined |
| Transverse + posterior wall | Most common associated type requiring surgery |
| T-shaped | Transverse + vertical limb |
| Anterior column/wall + posterior hemitransverse | AC + PHT |
| Both-column | Entire articular surface detached from the intact axial skeleton ("floating acetabulum") |
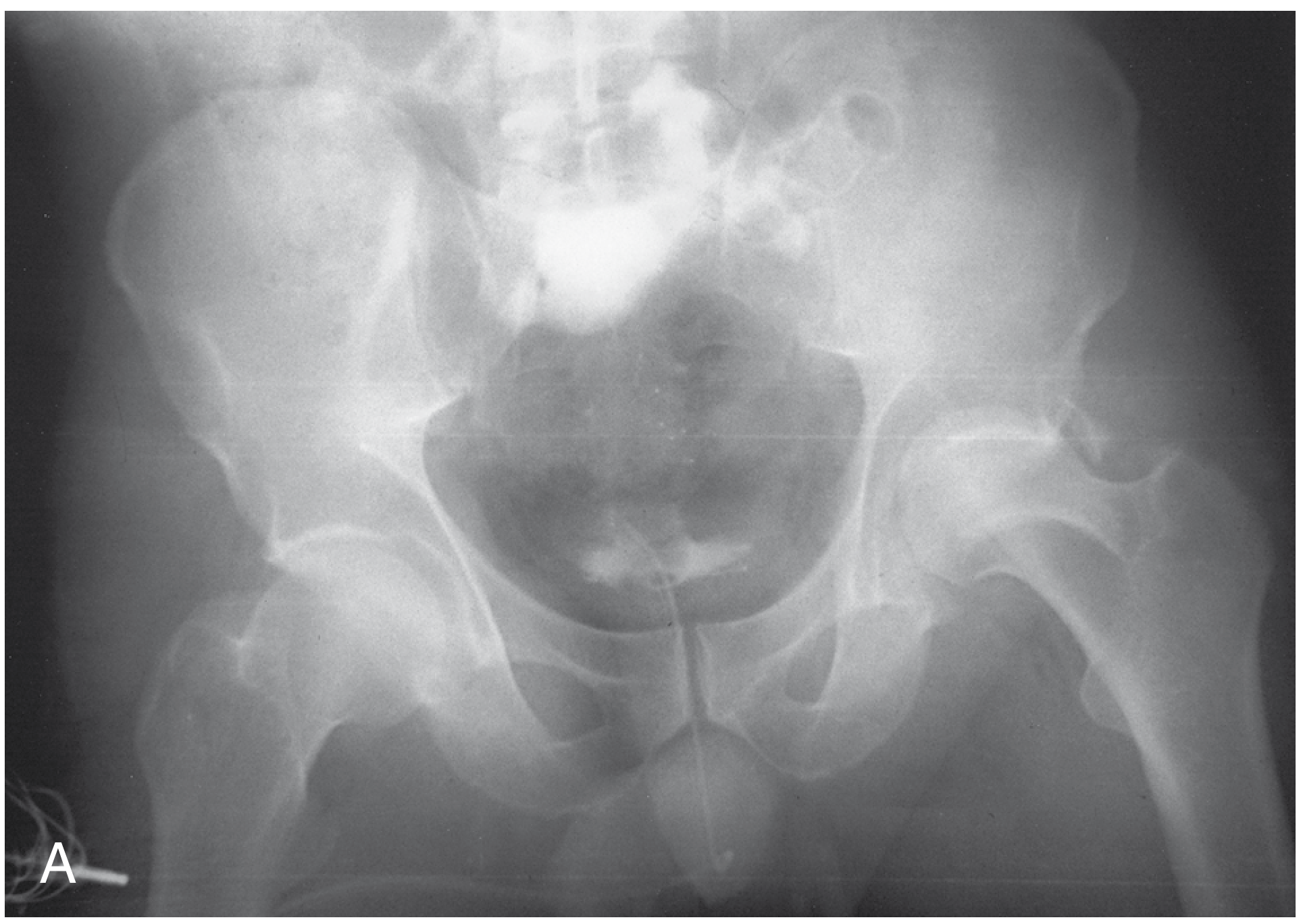
Imaging Assessment
Radiographic Views
- AP pelvis - standard; gives overview; measures medial roof arc
- Judet views (45° obliques):
- Iliac oblique - shows posterior column and anterior wall; measures posterior roof arc
- Obturator oblique - shows anterior column and posterior wall; measures anterior roof arc
- CT scan - mandatory once acetabular fracture is diagnosed:
- Defines fracture pattern precisely
- Identifies articular impaction
- Detects intraarticular fragments
- Assesses displacement at the weight-bearing dome (superior 10 mm of acetabular articular surface)
- Guides treatment decision
The Weight-Bearing Dome - Key Prognostic Concept
Rowe and Lowell first identified the superior dome (roof) of the acetabulum as the critical prognostic structure. It is defined as the superior third of the weight-bearing area and corresponds radiographically to the superior 10 mm of the acetabular articular surface on axial CT (Olson and Matta).
Core principle: Fractures that do NOT involve the weight-bearing dome can be considered for nonoperative management if the hip is stable and congruent. Fractures that DO involve the dome require a decision based on the degree of displacement.
Criteria for Nonoperative (Conservative) Management
Absolute Indications for Nonoperative Treatment
- Undisplaced fractures (or displacement <2 mm) - including those involving the weight-bearing dome
- Displaced fractures in regions NOT involving the weight-bearing dome - confirmed by roof arc measurements >45° (or revised criteria - see below)
- Both-column fractures with secondary congruence (see below)
- Wall fractures that do not compromise hip stability (confirmed by dynamic stress examination)
- Patients unable to withstand surgery - significant medical comorbidities
The Roof Arc Measurement (Matta)
The roof arc quantifies how much of the weight-bearing dome remains intact. It is measured on all three views with the leg out of traction and the femoral head concentrically reduced.
Method: Draw a vertical line through the center of the femoral head. Then draw a line from the center of the femoral head to the fracture line at the articular surface. The angle between these two lines = the roof arc angle.
| View | Roof Arc Measured | Classic Criterion (Matta) | Revised Biomechanical Criterion |
|---|---|---|---|
| AP view | Medial roof arc | >45° | >45° |
| Obturator oblique | Anterior roof arc | >45° | >25° |
| Iliac oblique | Posterior roof arc | >45° | >70° |
If the roof arc exceeds these values on all three views, the weight-bearing dome is intact and nonoperative management is appropriate regardless of displacement below the dome.
Note (Rockwood & Green 2025): The classic 45° value has been questioned. Subsequent biomechanical studies produced different criteria (45° medial, 25° anterior, 70° posterior). Even newer sit-to-stand loading studies suggest significantly higher critical angles may be needed, though clinical implications remain uncertain.
Roof arc is NOT applicable to: both-column fractures (no intact acetabulum to measure) or posterior wall fractures.
Special Situations
Both-Column Fractures with "Secondary Congruence"
Both-column fractures disconnect the entire articular surface from the intact axial skeleton ("floating acetabulum"). In some cases, the displaced acetabular fragments still maintain a congruent relationship with the femoral head even without traction - this is called secondary congruence.
Criteria for nonoperative management of both-column fractures:
- Parallelism between femoral head and acetabular articular surface in all three radiographic views (AP and both Judet views), without traction
- Fragment displacement and medial joint displacement not so excessive as to limit motion
- Limb shortening must be acceptable
Secondary congruence is necessary but not sufficient for nonsurgical treatment. These fractures do not have as good a prognosis as anatomically reduced fractures, but outcomes are acceptable in appropriate patients.
Posterior Wall Fractures
- Cannot be assessed by roof arc measurements
- May only be treated nonoperatively if the hip is completely stable
- Previously thought that <20% posterior wall involvement (on axial CT) was stable - but hip instability can still occur in some cases
- Mandatory dynamic stress examination under anaesthesia is the only reliable way to determine hip stability in posterior wall fractures - assumed unstable until proved otherwise
- Special hazard - cranial/peripheral posterior wall fragments: occur after falls from height with hip in extension; maximal instability in extension and adduction (walking position); even small fragments carry high complication rates
Nonoperative Treatment Protocol (Campbell's Operative Orthopaedics 2026)
Stage 1 - Acute Phase
| Parameter | Details |
|---|---|
| Weight bearing | Non-weight bearing for 6 to 12 weeks (depending on fracture characteristics) |
| Early mobilization | Allowed, but with non-weight bearing precautions |
| Radiograph at first mobilization | Mandatory - AP pelvis immediately after patient is first mobilized |
| Serial radiographs | Frequently thereafter to confirm no displacement |
| Repeat CT | May be needed to confirm maintenance of reduction |
| Traction | Distal femoral skeletal traction (10% of body weight, max 20-25 lb) if needed for unstable fracture-dislocation patterns pending definitive treatment |
Stage 2 - Transition (Weeks 6-12)
- When radiographic and clinical signs suggest healing - begin progressive weight bearing
- Typically partial weight bearing from ~6 weeks if no displacement on serial X-rays
- Full weight bearing usually by 10-12 weeks when fracture consolidated
Stage 3 - Rehabilitation
- Gait training, hip strengthening exercises
- Return to activities as tolerated
Indications for URGENT/EMERGENCY Surgery (i.e., cannot be managed conservatively)
Even an "undisplaced" fracture may require emergency surgery if:
| Indication | Rationale |
|---|---|
| Irreducible hip dislocation | Femoral head locked between fragments |
| Progressive sciatic nerve deficit after fracture or reduction | Despite variable nerve recovery, emergent decompression indicated |
| Associated vascular injury requiring repair | Life-threatening |
| Open fracture | Contamination, infection risk |
| Ipsilateral femoral neck fracture | Compromises blood supply to femoral head |
| Persistent hip instability that cannot be controlled by traction | Joint at risk of further damage |
Outcomes of Nonoperative Treatment
Prognostic factors:
- Best outcomes: No dome involvement; secondary congruence in both-column; stable posterior wall; fractures below the weight-bearing dome
- Displacement <2 mm (even at the dome): acceptable outcomes with nonoperative treatment
- Main risk of nonoperative treatment: Secondary displacement - hence mandatory serial radiographic follow-up
From 2025 meta-analysis (Khalifa et al., Int J Surg 2025, 5680 patients - geriatric cohort): Operative management carries higher complication rates and higher THA conversion risk, but is associated with lower 1-year mortality compared to nonoperative management in elderly patients. The decision between operative and nonoperative in the geriatric patient cannot be justified on mortality data alone.
Follow-Up Protocol (Summary)
Day 0 → AP pelvis + Judet views + CT; establish diagnosis and displacement
Week 0-2 → Skeletal traction if needed; non-weight bearing
Week 2-6 → Serial AP pelvis radiographs (every 1-2 weeks)
First mobilization → Immediate AP pelvis post-mobilization
Week 6 → Radiograph + clinical review; consider partial weight bearing
Week 10-12 → Full weight bearing if healed
Month 6 → Final radiograph; assess for post-traumatic arthritis / AVN
Year 1-2 → Long-term surveillance (post-traumatic OA develops in 10-25%)
Key Points for Exams
| Concept | Detail |
|---|---|
| Standard classification | Letournel: 5 elementary + 5 associated = 10 types |
| Displacement threshold for nonoperative | <2 mm (universally accepted) |
| Weight-bearing dome on CT | Superior 10 mm of acetabular articular surface |
| Roof arc measurement - classic values | All >45° on AP, obturator oblique, iliac oblique |
| Roof arc NOT applicable to | Both-column fractures; posterior wall fractures |
| Secondary congruence | Both-column: articular fragments still congruent with femoral head without traction |
| Posterior wall stability test | Dynamic stress examination under anaesthesia |
| Non-weight bearing duration | 6-12 weeks |
| Fracture pattern most commonly requiring ORIF | Posterior wall; transverse + posterior wall |
| Geriatric operative vs. nonoperative | Operative: higher complications, but lower 1-year mortality |
Sources: Rockwood and Green's Fractures in Adults 10th Ed 2025, pp. 2441-2483; Campbell's Operative Orthopaedics 15th Ed 2026, pp. 3498-3502; Miller's Review of Orthopaedics 9th Ed; Khalifa et al., Int J Surg 2025 [PMID 40540452].
This is a shared conversation. Sign in to Orris to start your own chat.