Can u give me the decision making flowchart on finding out the type of heamoglobinopathy and how to guide to treatment. In peadiatrics. Very simple easy to understand one
A clean, simple pediatric decision-making flowchart titled "Diagnosing & Treating Haemoglobinopathy in Children". The flowchart should flow top to bottom with clear boxes and arrows, easy to read, medical style, white background, blue and orange color scheme. The flowchart structure: START box: "Child with suspected haemoglobinopathy (anaemia, jaundice, failure to thrive, family history)" Arrow down to: "Step 1: Initial Tests — CBC + Peripheral Blood Film + Reticulocyte Count" Then splits into TWO paths: LEFT PATH label: "Microcytic anaemia (low MCV)" RIGHT PATH label: "Normocytic / haemolytic anaemia (normal MCV)" LEFT PATH continues to: Box: "Step 2: Check Serum Ferritin & Iron Studies" Then splits: - "Iron deficiency → Treat with oral iron" (end box, green) - "Iron normal/high → Proceed to Hb Electrophoresis" RIGHT PATH goes to: Box: "Step 2: Hb Electrophoresis + HbF, HbA2 levels" Both Hb Electrophoresis paths merge into a central decision diamond: "What does Hb Electrophoresis show?" This splits into 4 branches: Branch 1: "HbSS or HbSβ0 — Sickle Cell Anaemia (Severe)" → Treatment box: "Penicillin prophylaxis, Hydroxyurea, Folic acid, Vaccinations, Refer Haematologist, Transfusion if needed" Branch 2: "HbSC or HbSβ+ — Milder Sickle Variant" → Treatment box: "Monitor, Hydroxyurea if symptomatic, Folic acid, Annual eye/TCD screening" Branch 3: "High HbA2 (>3.5%) ± low MCV — Beta-Thalassaemia" → Sub-branch: "HbA2 3.5-7% = Beta Thal Trait → Genetic counselling only" → Sub-branch: "HbF high, HbA absent = Beta Thal Major → Lifelong transfusions + Chelation + BMT consideration" Branch 4: "Normal Hb pattern but Haemolytic signs — Consider: HbH disease (alpha thal), G6PD, or other RBC defect" → Treatment box: "Genetic testing, Avoid triggers, Supportive care, Specialist referral" At the bottom: A note box: "All cases: Genetic counselling + Family screening recommended"
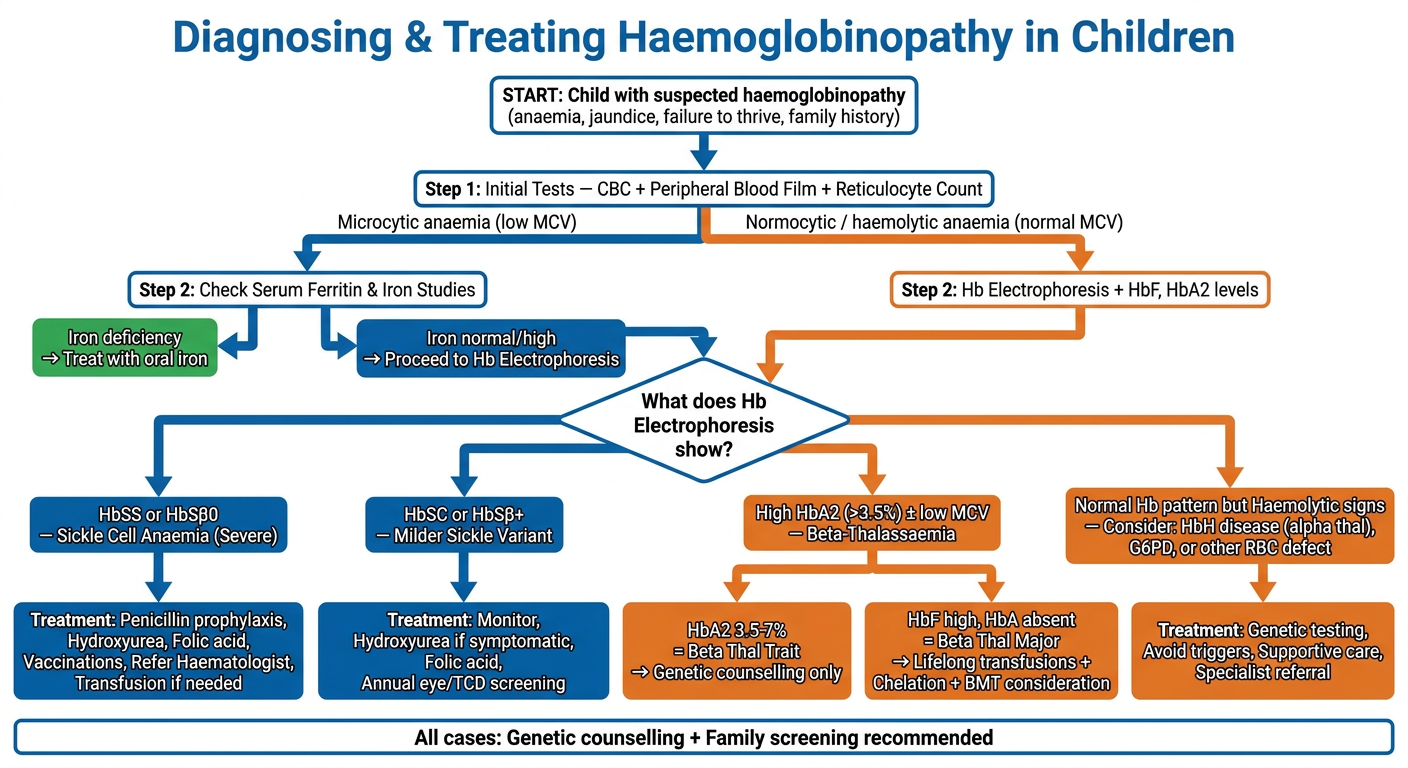
How to Use This Flowchart
Step 1 - Start with CBC + Film + Reticulocyte Count
Step 2 - Is the MCV low (microcytic)?
- Yes (low MCV): Check ferritin and iron studies first to rule out iron deficiency anaemia. If iron is normal or high, move to Hb electrophoresis.
- No (normal/haemolytic pattern): Go straight to Hb electrophoresis.
Step 3 - Hb Electrophoresis is the KEY test
| Electrophoresis Result | Diagnosis | Severity |
|---|---|---|
| HbSS, HbA absent | Sickle Cell Anaemia | Severe |
| HbSS + low MCV | HbSβ0-thalassaemia | Moderate-Severe |
| HbS + HbC | HbSC Disease | Mild-Moderate |
| HbS + some HbA | HbSβ+-thalassaemia | Mild-Moderate |
| High HbA2 (>3.5%), low MCV, HbA present | Beta Thal Trait | Carrier only |
| High HbA2, HbF dominant, no HbA | Beta Thal Major | Severe |
| Normal Hb pattern + haemolysis | Alpha thal (HbH), G6PD, other | Varies |
Treatment Guide by Type
- Penicillin prophylaxis from 2 months of age
- Hydroxyurea - reduces vaso-occlusive crises and chest syndrome
- Folic acid daily
- Up-to-date vaccinations (pneumococcal, meningococcal, Hib)
- Transfusion: for stroke, acute chest syndrome, severe aplastic crisis
- Transcranial Doppler (TCD) screening from age 2 yearly
- Haematologist referral essential
- Monitor growth, vision (annual eye exam - retinopathy risk in HbSC)
- Hydroxyurea if symptomatic
- Folic acid
- Fewer transfusions needed
- Lifelong regular transfusions (every 2-4 weeks, target HbA >9-10 g/dL)
- Iron chelation therapy (deferoxamine or deferasirox) once iron overloads
- Bone marrow transplant - curative option, best results in young children with matched sibling donor
- Folic acid, endocrine monitoring (growth, thyroid, glucose)
- No treatment needed
- Genetic counselling for parents - risk of major in offspring if both parents carry trait
- Avoid oxidant drugs (same as G6PD)
- Folic acid
- Transfusions for severe anaemia episodes
- Specialist referral
One Rule for All Cases
Always offer genetic counselling and family screening. If one child is diagnosed, siblings and parents should be tested. Carrier couples have a 1-in-4 chance of an affected child with each pregnancy.