Erythropoiesis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the key information needed for a comprehensive answer. Let me compile everything into a thorough, well-structured response.
Erythropoiesis
Erythropoiesis is the process by which red blood cells (erythrocytes) are produced from hematopoietic stem cells in the bone marrow. Under normal conditions, approximately 1% of circulating erythrocytes is replaced daily - corresponding to about 250 billion cells, with 2.5-3.0 million erythrocytes produced every second.
Sites of Erythropoiesis
| Stage of Life | Site |
|---|---|
| Yolk sac (primitive) | 0-2 months gestation |
| Liver, spleen | 2nd-7th month gestation |
| Bone marrow (red marrow) | From ~5th month onwards and throughout adult life |
In adults, active red marrow is found in the vertebrae, sternum, ribs, pelvis, proximal femur, and proximal humerus.
Regulation by Erythropoietin (EPO)
The central regulator of erythropoiesis is erythropoietin (EPO), a 30.4-kDa glycoprotein produced primarily in the kidney (peritubular interstitial cells). The oxygen-sensing feedback loop operates as follows:
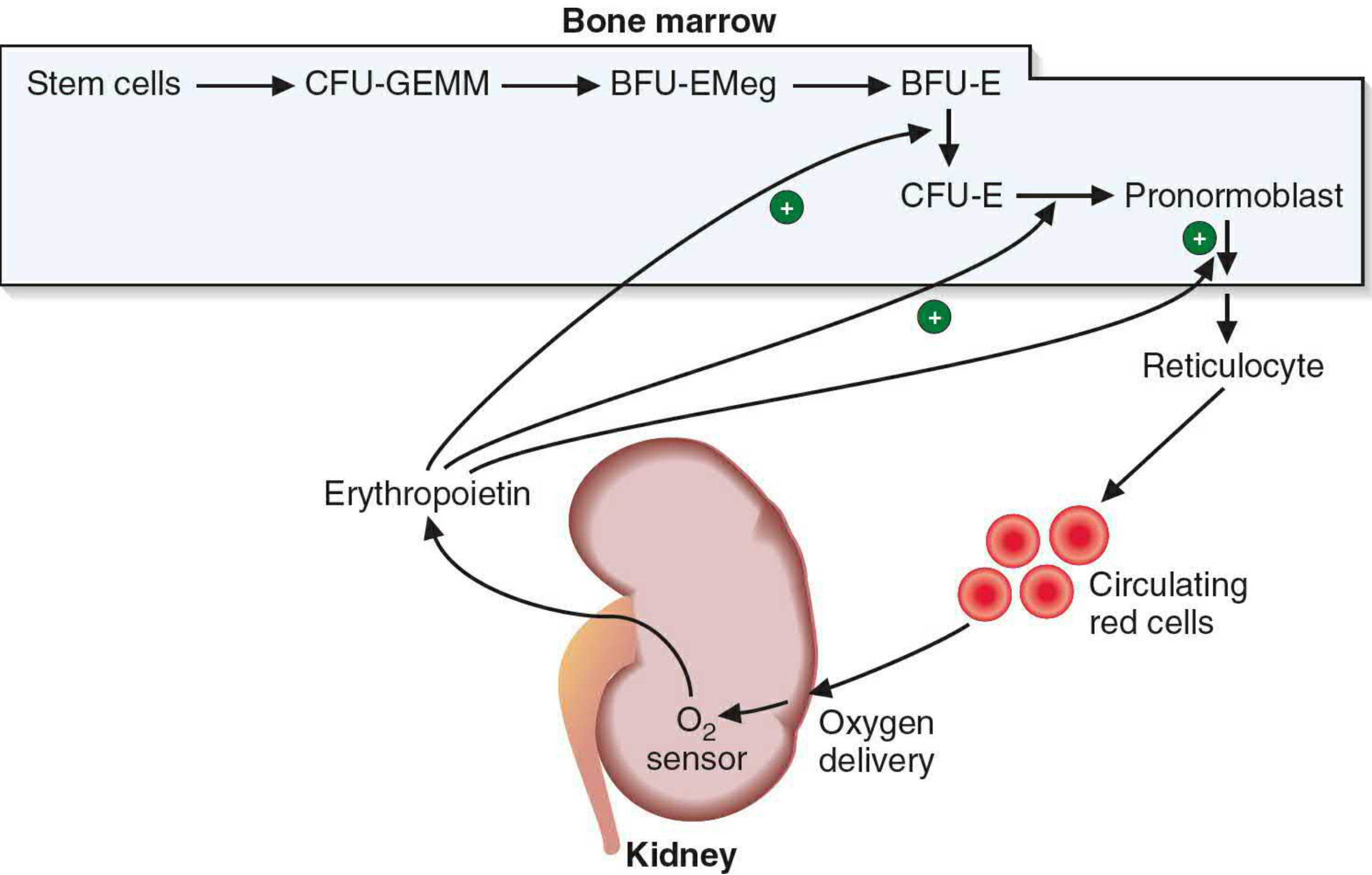
Figure: EPO stimulation pathway - Kidney senses reduced O₂ delivery → releases EPO → stimulates BFU-E, CFU-E, and pronormoblasts → more circulating red cells
- Hypoxia (from anemia, altitude, cardiopulmonary disease) stimulates HIF-2α in renal interstitial cells
- HIF-2α drives EPO gene transcription
- EPO binds EPO receptors (EPO-R) on erythroid progenitors and promotes their survival, proliferation, and differentiation via the JAK2/STAT5 signaling pathway
- Rising red cell mass corrects tissue oxygenation, completing the negative feedback loop
Progenitor Hierarchy (Pre-Morphological Stages)
These stages are not visible by light microscopy but are defined functionally by colony assays:
HSC → CMP → MEP → BFU-E → CFU-E → Proerythroblast
| Cell | Key Feature |
|---|---|
| HSC (Hematopoietic Stem Cell) | Self-renewing, pluripotent |
| CMP (Common Myeloid Progenitor) | Gives rise to myeloid lines |
| MEP (Megakaryocyte/Erythrocyte Progenitor) | Bipotent; requires GATA-1 transcription factor for erythroid commitment |
| BFU-E (Burst-Forming Unit - Erythroid) | Large colony-former; EPO-independent initially |
| CFU-E (Colony-Forming Unit - Erythroid) | Small colony-former; highly EPO-dependent |
| Proerythroblast | First morphologically recognizable erythroid cell |
- The full progenitor chain from stem cells is: Stem cell → CFU-GEMM → BFU-EMeg → BFU-E → CFU-E → Pronormoblast
- GATA-1 is the master transcription factor required for terminal erythroid differentiation
Morphologically Recognizable Stages (Maturation Series)
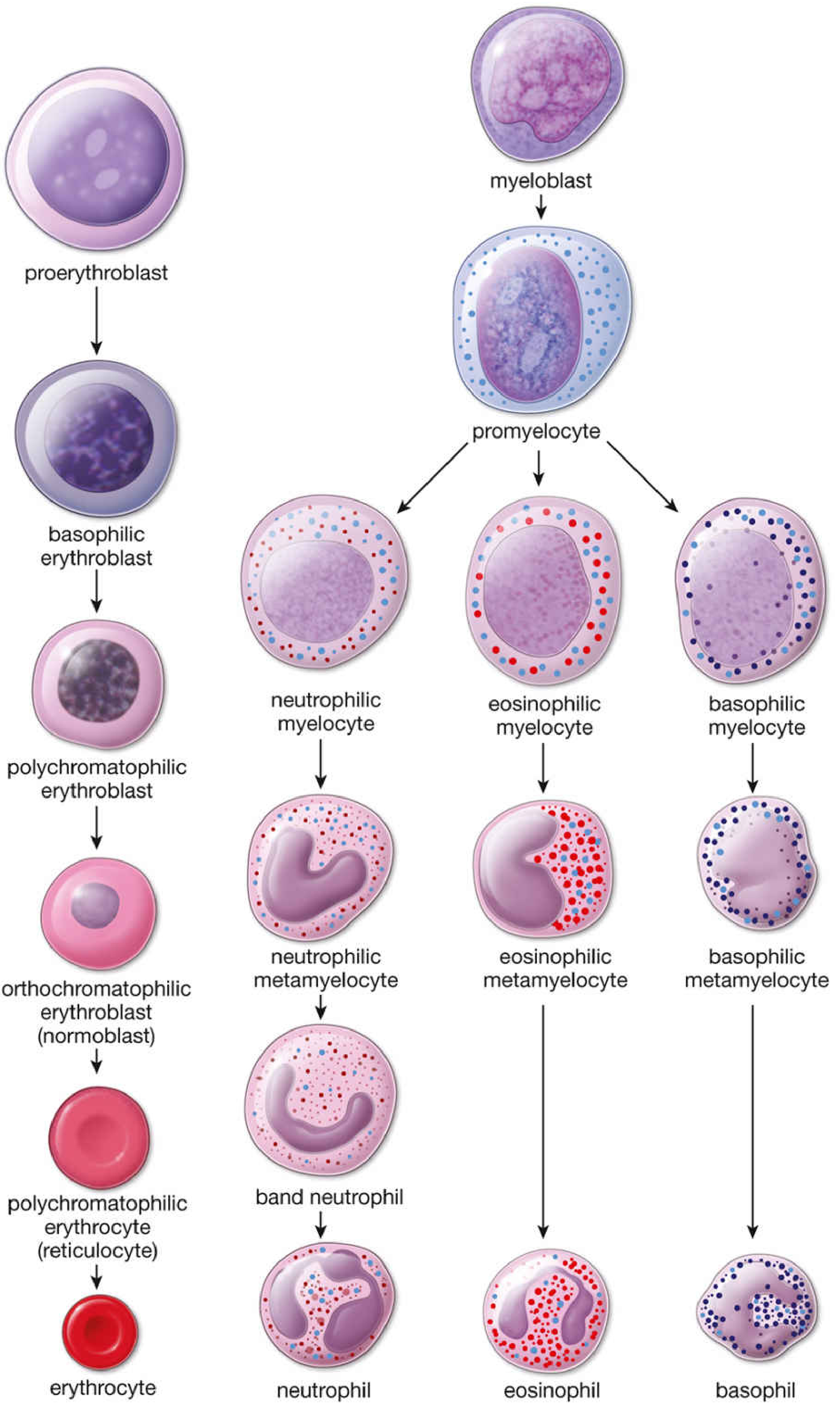
Figure: Normal bone marrow cell stages - erythroid series on the left
1. Proerythroblast (Pronormoblast)
- Size: 12-20 μm (largest erythroid precursor)
- Nucleus: large, spherical, with 1-2 nucleoli
- Cytoplasm: mild basophilia (free ribosomes beginning hemoglobin synthesis)
- Duration: ~24 hours
2. Basophilic Erythroblast
- Size: 10-16 μm (smaller than proerythroblast)
- Nucleus: smaller, progressively more heterochromatic
- Cytoplasm: strong basophilia due to abundant polyribosomes actively synthesizing hemoglobin
- Duration: ~24 hours; undergoes mitosis
3. Polychromatophilic Erythroblast
- Cytoplasm: mixed blue and pink (both ribosomes and accumulating hemoglobin present)
- Nucleus: checkerboard heterochromatin pattern; smaller than previous stage
- Duration: ~30 hours
- Last stage capable of mitosis
4. Orthochromatophilic Erythroblast (Normoblast)
- Cytoplasm: predominantly eosinophilic (large amount of hemoglobin)
- Nucleus: small, compact, pyknotic (dense, dark-staining)
- At this stage, the nucleus is extruded - this is the last nucleated stage
- Cannot undergo further division
5. Reticulocyte (Polychromatophilic Erythrocyte)
- Anucleate
- Still contains residual ribosomes and mRNA - capable of hemoglobin synthesis
- Stains with supravital dyes (e.g., new methylene blue) showing a reticulum of RNA
- Released from bone marrow into blood
- Circulates for 1-2 days; final maturation occurs in the spleen where ribosomes/mRNA are removed
- Normal reticulocyte count: ~0.5-2.5% of RBCs
6. Mature Erythrocyte
- 7.2 μm biconcave disc
- Anucleate, no organelles
- Packed with hemoglobin (~34 g/dL intracellular)
- Lifespan: ~120 days
- Removed by macrophages of spleen, bone marrow, and liver (the mononuclear phagocyte system)
RNA vs. Hemoglobin During Maturation
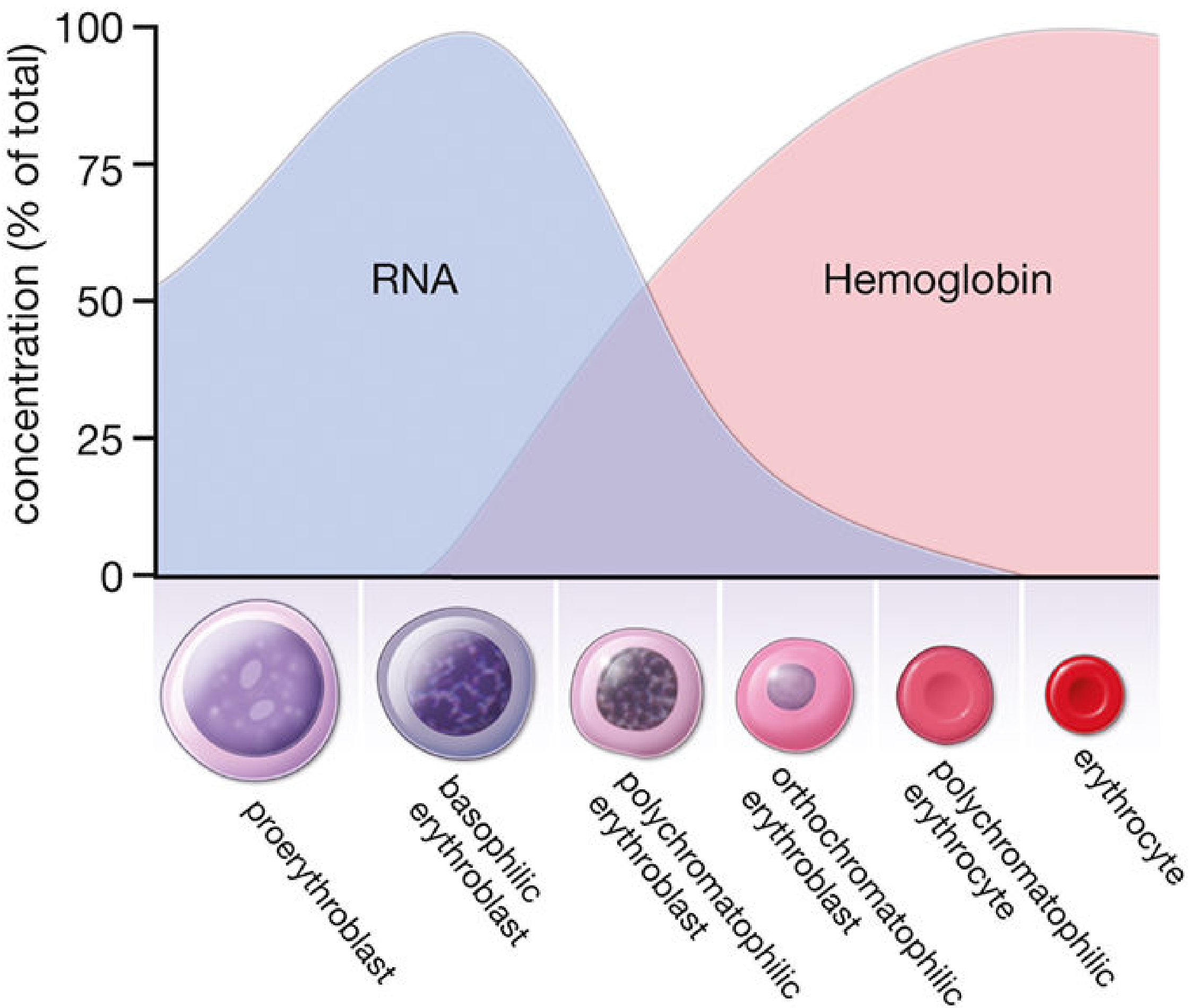
Figure: As cells mature, RNA (ribosomes) peaks at basophilic erythroblast stage and progressively falls; hemoglobin accumulates from polychromatophilic stage onward and plateaus at the mature erythrocyte
Kinetics Summary
- From basophilic erythroblast → circulation takes approximately 1 week
- Each proerythroblast undergoes 4 mitotic divisions (producing ~16 erythrocytes per progenitor cell)
- Mitosis occurs at: proerythroblast, basophilic erythroblast, and polychromatophilic erythroblast stages only
- Bone marrow is not a storage site for erythrocytes - cells are released as soon as formed
Nutritional Requirements
Three cofactors are essential for effective erythropoiesis:
| Nutrient | Role | Deficiency Effect |
|---|---|---|
| Iron | Hemoglobin synthesis (heme component); regulated by HRI kinase sensing heme availability | Microcytic, hypochromic anemia; iron-deficient erythropoiesis |
| Vitamin B12 | DNA synthesis (via methylcobalamin and adenosylcobalamin); thymidine and purine synthesis | Megaloblastic anemia; ineffective erythropoiesis; hypersegmented neutrophils |
| Folate | Single-carbon transfer reactions; pyrimidine and purine synthesis | Megaloblastic anemia; similar to B12 deficiency |
In megaloblastic anemia (B12 or folate deficiency), erythroid progenitors cannot progress through the cell cycle and undergo apoptosis (ineffective erythropoiesis), leading to:
- Reduced reticulocyte count despite erythroid hyperplasia in marrow
- Elevated serum bilirubin and LDH
- Accelerated iron turnover
In iron deficiency, the HRI kinase pathway suppresses globin synthesis and mTORC1 activity, producing microcytic (small) but morphologically normoblastic erythropoiesis.
Iron Recycling
- Each mL of blood contains ~0.5 mg of iron
- The gut absorbs only ~1 mg iron/day (~5-10% of dietary intake)
- The majority of iron for erythropoiesis comes from recycling of iron from aged RBCs via splenic and hepatic macrophages
- Intracellular iron, heme, and globin must be precisely matched - excess of any is toxic
Red Cell Destruction (End of Lifespan)
After ~120 days, senescent erythrocytes are phagocytosed by macrophages of the spleen, bone marrow, and liver:
- Globin → hydrolyzed to amino acids → recycled
- Iron from heme → stored as ferritin/hemosiderin in spleen → recycled to erythropoiesis
- Heme porphyrin ring → partially degraded to bilirubin → bound to albumin → transported to liver → conjugated to bilirubin glucuronide → excreted in bile
Clinical Relevance
| Condition | Mechanism |
|---|---|
| Anemia of CKD | EPO deficiency (damaged renal interstitium cannot produce EPO); treated with erythropoiesis-stimulating agents (ESAs) |
| Polycythemia vera | Autonomous EPO-independent erythroid proliferation (JAK2 V617F mutation) |
| Thalassemia | Imbalanced globin chain synthesis → precipitation of excess chains → RBC precursor damage → ineffective erythropoiesis → iron overload |
| High-altitude adaptation | Hypoxia → HIF-2α → EPO → increased RBC mass |
| Iron deficiency anemia | Microcytic, hypochromic RBCs; low serum ferritin, high TIBC |
| Megaloblastic anemia | Large oval erythrocytes (macro-ovalocytes), hypersegmented neutrophils |
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 737-746
- Basic Medical Biochemistry: A Clinical Approach 6e, pp. 1535-1536
- Brenner and Rector's The Kidney, pp. 2465-2470
Erythropoiesis physiology mbbs year 1
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive, MBBS Year 1-targeted answer from Guyton & Hall. Let me compile the full response.
Erythropoiesis - MBBS Year 1 Physiology
(Based on Guyton and Hall Textbook of Medical Physiology)
Definition
Erythropoiesis is the process of formation and maturation of red blood cells (erythrocytes) from hematopoietic stem cells in the bone marrow.
1. Sites of Erythropoiesis
| Period | Site |
|---|---|
| Early embryo (first weeks) | Yolk sac (primitive nucleated RBCs) |
| Middle trimester | Liver (main site), also spleen and lymph nodes |
| Last month of gestation onwards | Red bone marrow (exclusively) |
In adults: RBCs are produced in the red marrow of membranous bones - vertebrae, sternum, ribs, and ilia. After age 20, the long bones (except proximal humerus and tibia) become fatty and stop producing RBCs. Marrow productivity decreases further with increasing age.
2. Genesis of Blood Cells - Stem Cell Hierarchy
All blood cells originate from a single Multipotent Hematopoietic Stem Cell (MHSC) in the bone marrow.
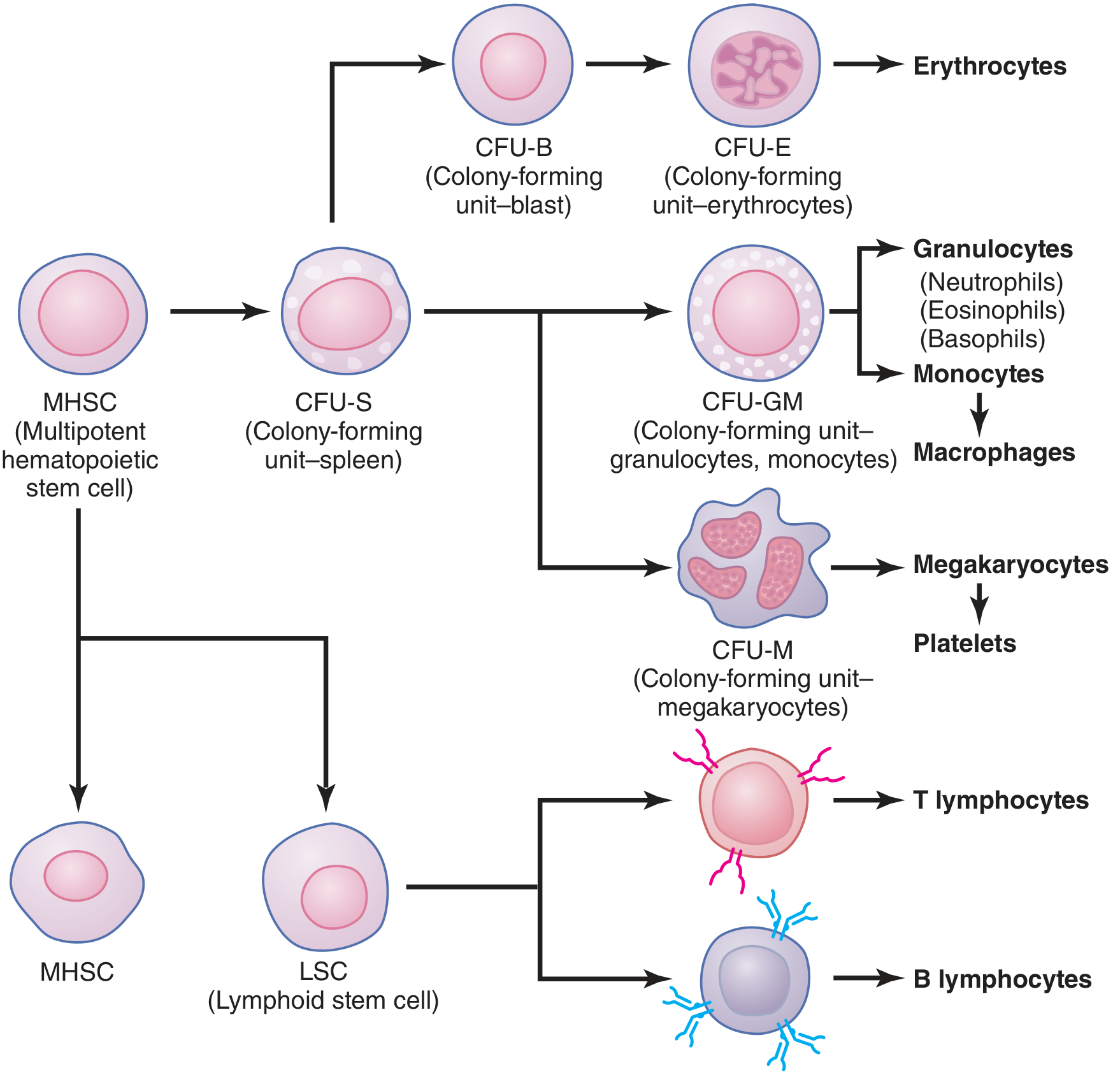
Key concept: Two types of proteins control stem cell fate:
- Growth inducers (e.g., IL-3) - promote proliferation, not differentiation
- Differentiation inducers - cause commitment to a specific cell lineage
The committed erythroid progenitor is the CFU-E (Colony-Forming Unit - Erythrocyte), which responds to erythropoietin.
3. Stages of Differentiation (Maturation Series)
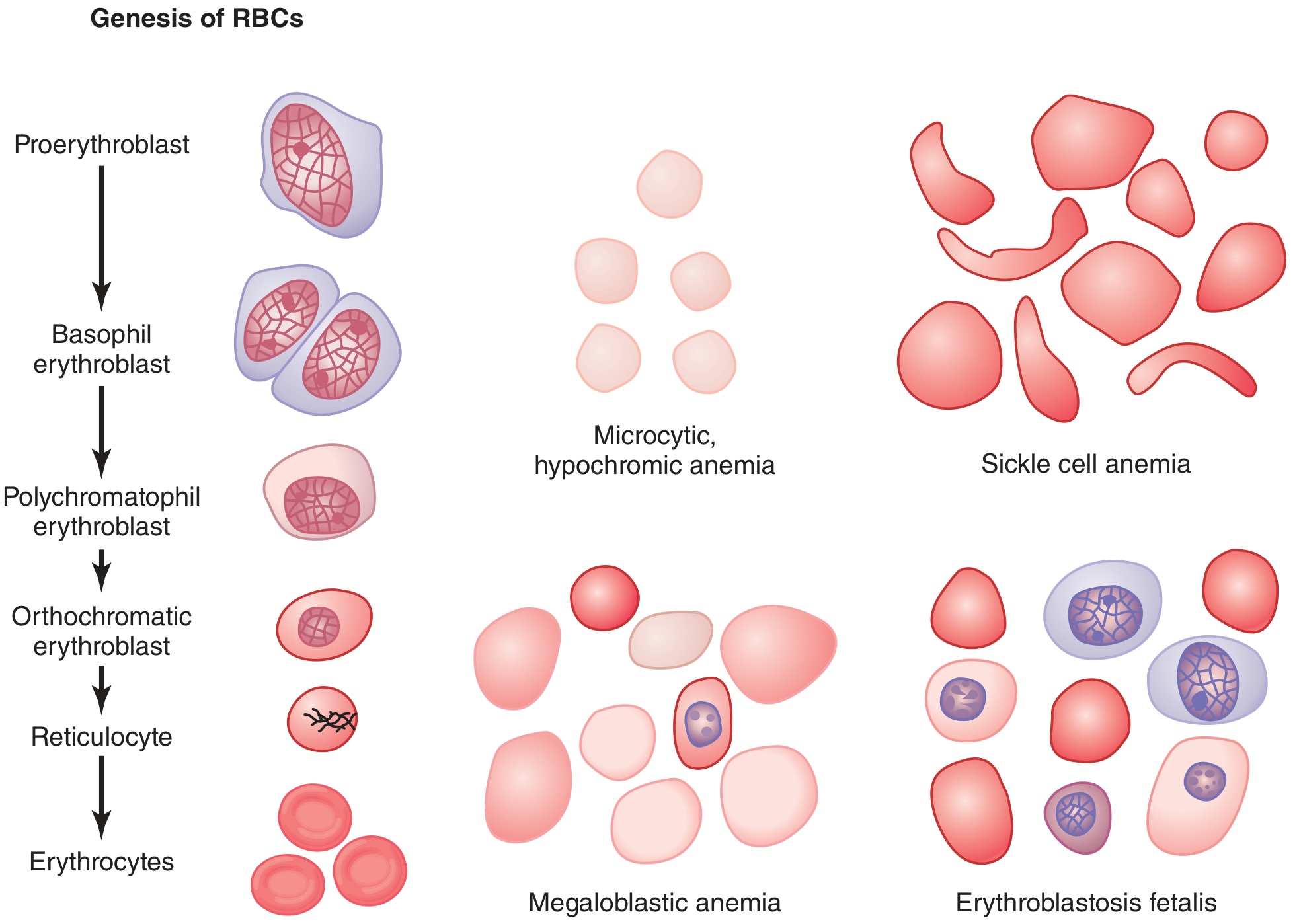
The sequence from committed progenitor to mature RBC:
CFU-E → Proerythroblast
- First morphologically recognizable stage
- Large cell with prominent nucleus
- Cytoplasm begins accumulating components for Hb synthesis
Proerythroblast → Basophil Erythroblast (1st generation)
- Stains strongly with basic dyes (deeply basophilic cytoplasm)
- Rich in ribosomes (polyribosomes) actively synthesizing hemoglobin
- Undergoes mitosis → divides several times
Basophil Erythroblast → Polychromatophil Erythroblast (2nd-3rd generation)
- Hemoglobin first appears in the cytoplasm at this stage
- Mixed staining: both basophilic (ribosomes) and acidophilic (hemoglobin)
- Nucleus becomes progressively smaller and denser
Polychromatophil → Orthochromatic Erythroblast (4th generation)
- Cytoplasm becomes predominantly eosinophilic (filled with Hb ~34%)
- Nucleus condenses to small pyknotic remnant
- Nuclear remnant is absorbed or extruded from cell
- Endoplasmic reticulum also reabsorbed at this stage
Orthochromatic Erythroblast → Reticulocyte
- Anucleate - no longer has a nucleus
- Still contains small amounts of basophilic material: remnants of Golgi apparatus, mitochondria, and cytoplasmic organelles
- Named "reticulocyte" because of this reticular (net-like) basophilic material seen with supravital stains
- Passes from bone marrow into blood capillaries by diapedesis (squeezing through capillary pores)
Reticulocyte → Mature Erythrocyte
- Basophilic material disappears within 1-2 days in circulation
- Normal reticulocyte count = slightly less than 1% of all RBCs
- Mature RBC: biconcave disc, ~7-8 μm diameter, no nucleus or organelles, packed with hemoglobin
Memory tip: Pro → Baso → Poly → Ortho → Retic → RBC ("Please Be Polite Or Remain Respectful")
4. Regulation of RBC Production - Erythropoietin
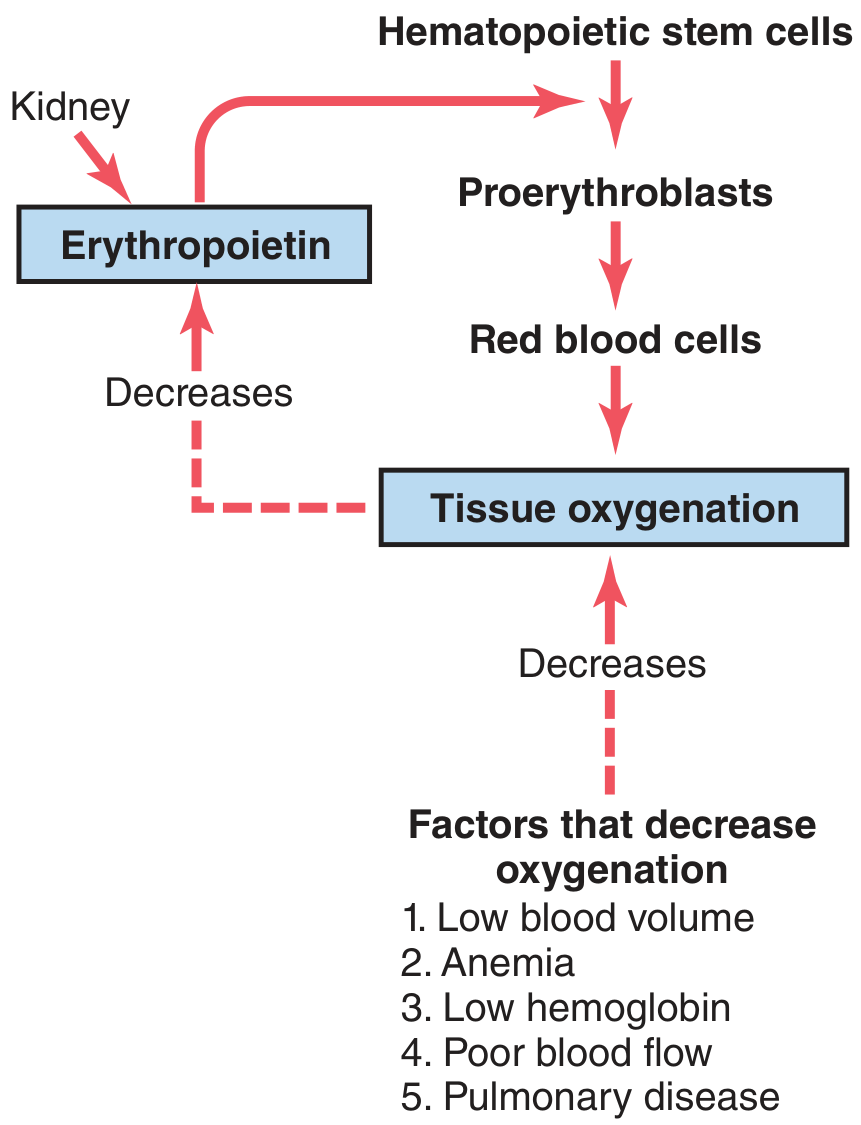
The Key Hormone: Erythropoietin (EPO)
- A glycoprotein, molecular weight ~34,000
- Produced: 90% kidneys (peritubular fibroblast-like interstitial cells in cortex and outer medulla), 10% liver
- EPO stimulates production of proerythroblasts from hematopoietic stem cells, and speeds up all subsequent maturation steps
The Feedback Loop:
Hypoxia / Low O₂ delivery
↓
Kidney senses ↓ O₂ → produces EPO
↓
EPO acts on bone marrow CFU-E
↓
↑ Proerythroblast formation
↓
↑ RBCs released into circulation
↓
Tissue oxygenation restored
↓
EPO production falls (negative feedback)
Molecular Mechanism:
- Hypoxia → ↑ HIF-1 (Hypoxia-Inducible Factor-1) in renal tissue
- HIF-1 binds to hypoxia response element in the EPO gene
- → Transcription of EPO mRNA → ↑ EPO synthesis
Timeline:
- EPO production begins within minutes to hours of hypoxia
- Reaches maximum within 24 hours
- New RBCs appear in blood only after ~5 days
Factors that DECREASE tissue oxygenation → INCREASE EPO → INCREASE RBC production:
| Factor | Example |
|---|---|
| Low blood volume | Hemorrhage |
| Anemia | Any cause |
| Low hemoglobin | Iron deficiency |
| Poor blood flow | Cardiac failure |
| Lung disease | Impaired O₂ absorption |
| High altitude | Low atmospheric O₂ |
5. Maturation Factors - Nutritional Requirements
Two vitamins are specifically required for nuclear maturation (DNA synthesis) of erythroid precursors:
A. Vitamin B12 (Cyanocobalamin)
- Essential for DNA synthesis
- Deficiency → cells cannot divide normally → abnormally large cells (megaloblasts)
- Absorbed in terminal ileum with the help of Intrinsic Factor (produced by gastric parietal cells)
- Deficiency causes: Megaloblastic (Pernicious) Anemia
B. Folic Acid
- Also essential for DNA synthesis (one-carbon transfer reactions)
- Deficiency produces identical blood picture to B12 deficiency
- Megaloblastic anemia - large oval macrocytes, hypersegmented neutrophils
C. Iron
- Essential for hemoglobin synthesis (incorporated into heme)
- Total body iron: 4-5 g
- ~65% in hemoglobin
- ~4% in myoglobin
- ~15-30% stored as ferritin/hemosiderin
- ~0.1% in plasma as transferrin-bound iron
Iron metabolism:
- Absorbed from small intestine as Fe²⁺ (ferrous form)
- Transported in plasma bound to transferrin (beta-globulin)
- Stored in cells as ferritin (soluble) or hemosiderin (insoluble)
- Transferrin delivers iron to erythroid precursors by binding to receptors on erythroblasts → endocytosis → iron delivered to mitochondria for heme synthesis
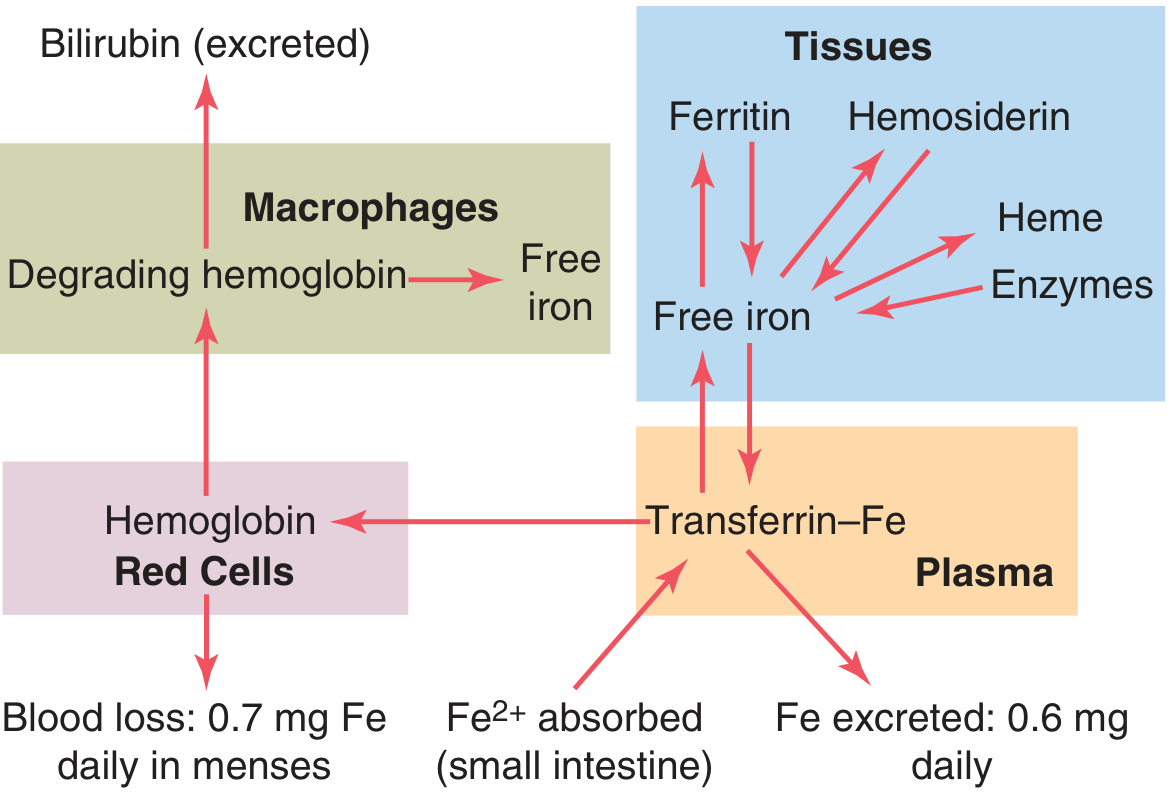
6. Life Span and Destruction of RBCs
- Life span: ~120 days
- Old RBCs become fragile because metabolic enzymes become progressively less active
- Self-destruct mainly in the spleen (red pulp spaces only 3 μm wide vs. 8 μm RBC diameter)
- Destroyed RBCs are phagocytized by macrophages (Kupffer cells of liver, splenic macrophages, bone marrow macrophages)
Fate of hemoglobin:
| Component | Fate |
|---|---|
| Iron (Fe) | Released → transferrin → back to bone marrow for new Hb synthesis, OR stored as ferritin/hemosiderin |
| Globin chains | Broken down into amino acids → recycled |
| Porphyrin ring (heme) | Converted to bilirubin → released into blood → liver → conjugated → excreted in bile |
7. Anemias - Applied Physiology
| Type | Cause | RBC Appearance |
|---|---|---|
| Blood loss anemia | Hemorrhage (acute or chronic) | Normal or microcytic hypochromic |
| Iron deficiency anemia | Insufficient iron for Hb synthesis | Microcytic, hypochromic (small, pale RBCs) |
| Megaloblastic anemia | B12 or folate deficiency | Large, oval macrocytes; hypersegmented neutrophils |
| Aplastic anemia | Bone marrow failure (radiation, chemicals, autoimmune) | Pancytopenia (all cell lines reduced) |
| Hemolytic anemia | Premature RBC destruction | Spherocytes, fragments |
| Polycythemia vera | Uncontrolled autonomous RBC production (JAK2 mutation) | ↑↑ RBCs, hematocrit 60-70% |
Quick Revision Summary
SITES: Yolk sac → Liver → Bone marrow (adult)
STAGES: CFU-E → Proerythroblast → Basophil → Polychromatophil
→ Orthochromatic → Reticulocyte (1-2 days) → RBC (120-day lifespan)
REGULATION: Hypoxia → HIF-1 → Kidney → EPO → Bone marrow → ↑ RBCs
MATURATION FACTORS: Iron (Hb synthesis) + B12 + Folate (DNA synthesis)
DESTRUCTION: Spleen (mainly) + Macrophages
→ Iron recycled; Heme → Bilirubin → Bile
Sources: Guyton and Hall Textbook of Medical Physiology (Chapter 33: Red Blood Cells, Anemia, and Polycythemia); Histology: A Text and Atlas (Eroschenko); Basic Medical Biochemistry - A Clinical Approach 6e
This is a shared conversation. Sign in to Orris to start your own chat.