Central pontine mylinolysis
Reading File
Finding Sources
Searching PubMed
"central pontine myelinolysis" OR "osmotic demyelination syndrome"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full synthesized answer.
Central Pontine Myelinolysis (CPM) / Osmotic Demyelination Syndrome (ODS)
Definition and Terminology
Central pontine myelinolysis is an acute demyelinating disorder affecting the center of the base of the pons, first described in 1959 by Adams and colleagues in 4 patients (2 alcoholics, 1 with scleroderma) who developed rapidly evolving quadriplegia and pseudobulbar palsy. The term reflects its anatomic location and essential pathology: dissolution of myelin sheaths with sparing of neurons and axons. Because identical lesions can occur outside the pons (extrapontine myelinolysis), the broader term osmotic demyelination syndrome (ODS) is now preferred in modern texts (Harrison's 22E, 2025).
Epidemiology and Risk Factors
CPM occurs equally in both sexes across all age groups, including children (especially those with severe burns). The reported incidence at autopsy was about 0.25% in one large series (3,548 consecutive autopsies). Most cases occur in the setting of serious systemic illness:
- Chronic alcoholism - the most common association (>50% of cases); often coexists with Wernicke's disease and polyneuropathy
- Rapid correction of hyponatremia - the most important triggering event (serum Na typically <130 mEq/L at baseline, often much lower)
- Chronic renal failure on dialysis
- Hepatic failure / liver transplantation (possibly cyclosporine-related)
- Advanced lymphoma, cancer, cachexia
- Severe burns (hyperosmolality is the key mechanism in this group)
- Severe bacterial infections, dehydration, electrolyte disturbances
- Acute hemorrhagic pancreatitis, pellagra
Pathology
The lesion is a single, confluent, symmetric zone of demyelination in the central base of the pons. Key features:
| Feature | Detail |
|---|---|
| Location | Central base of pons; may extend to medial lemnisci and tegmentum |
| Extent | A few mm to nearly the entire ventral pons |
| Sparing | Peripheral rim of myelin always spared; does NOT extend below pontomedullary junction |
| Extrapontine | Internal capsule, corpus callosum, deep cerebral white matter, thalamus, striatum, lateral geniculate body, cerebellar white matter |
| Micro | Destruction of myelinated sheaths; axons and nerve cells of pontine nuclei are spared; oligodendrocytes depleted; reactive phagocytes and glia present; inflammation absent |
| Stage | All lesions appear at the same stage (synchronous onset) |
The absence of inflammation clearly differentiates CPM from MS and postinfectious encephalomyelitis. The preservation of axons and neurons distinguishes it from infarction. It resembles Marchiafava-Bignami disease histologically.
Pathogenesis
A rapid rise in serum osmolality is the near-obligate antecedent. The leading mechanism:
- In chronic hyponatremia, brain cells adapt by extruding organic osmolytes (taurine, glutamate, myoinositol) to reduce cell volume
- When sodium is corrected too quickly, osmolality rises rapidly - the brain cannot re-accumulate these osmolytes fast enough
- This osmotic stress selectively damages oligodendrocytes through uncertain mechanisms, leading to demyelination
- The center of the pons is particularly vulnerable - possibly due to its unique microvasculature or the density of interspersed gray and white matter elements
Laureno's experimental model (1983) confirmed: dogs made severely hyponatremic and then rapidly corrected with 3% saline developed spastic quadriparesis and CPM lesions indistinguishable from the human disease. Slow correction did not produce the disease.
In burn patients, extreme hyperosmolality itself (not hyponatremia correction) is the driver.
Clinical Features
Symptoms typically appear 2-6 days after rapid sodium correction.
Classic (Severe) Presentation
- Flaccid quadriplegia progressing to spasticity and extensor posturing
- Pseudobulbar palsy: inability to chew, swallow, or speak
- "Locked-in" syndrome: fully conscious but nearly completely paralyzed; only vertical eye movements and blinking preserved - the majority of severely affected patients reach this state
- Roughly 25% have impaired consciousness (dorsal/rostral pontine extension)
Preserved Functions (Typically)
- Pupillary reflexes
- Facial sensation
- Consciousness (unless extensive)
- Vertical gaze (distinguishes from brainstem infarction)
Partial / Milder Forms (increasingly recognized with MRI)
- Confusion
- Dysarthria and cerebellar ataxia (may persist months before full recovery)
- Disturbances of conjugate gaze
- Behavioral changes
Extrapontine variants
- Large symmetric lesions in frontal cortex and white matter without pontine involvement (rare)
- Thalamic, striatal, or cerebellar involvement
MRI Findings
MRI is the diagnostic tool of choice. The characteristic appearance:
- T2/FLAIR: symmetric high-signal intensity lesion in the central pons, involving transverse pontine fibers
- Corticospinal tracts are characteristically spared (the descending tracts run at the periphery of the pons)
- Classic "trident" or "bat wing" shape on axial T2
- DWI (diffusion restriction) may appear within a day of motor signs - earlier than T2 changes
- MRI changes may lag clinical onset by several days
- Extrapontine lesions may be identified simultaneously
Here are two T2-weighted MRI images demonstrating the characteristic pontine lesion:
Harrison's (axial T2 - normal-appearing pons for comparison with text description):
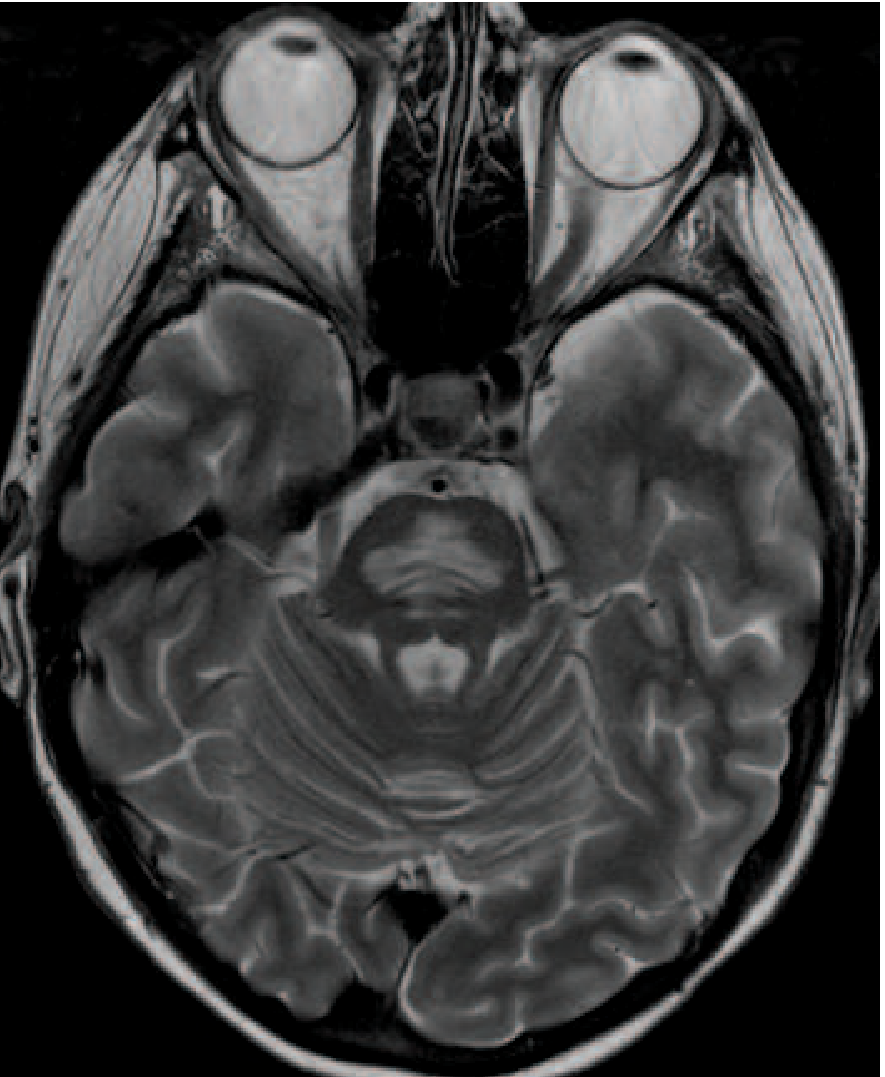
Axial T2-weighted MRI through the pons - the symmetric high-signal area characteristically involves transverse pontine fibers while sparing the descending corticospinal tracts. (Harrison's Principles of Internal Medicine 22E, Fig. 318-5)
Adams & Victor (T2 - CPM in an alcoholic patient):
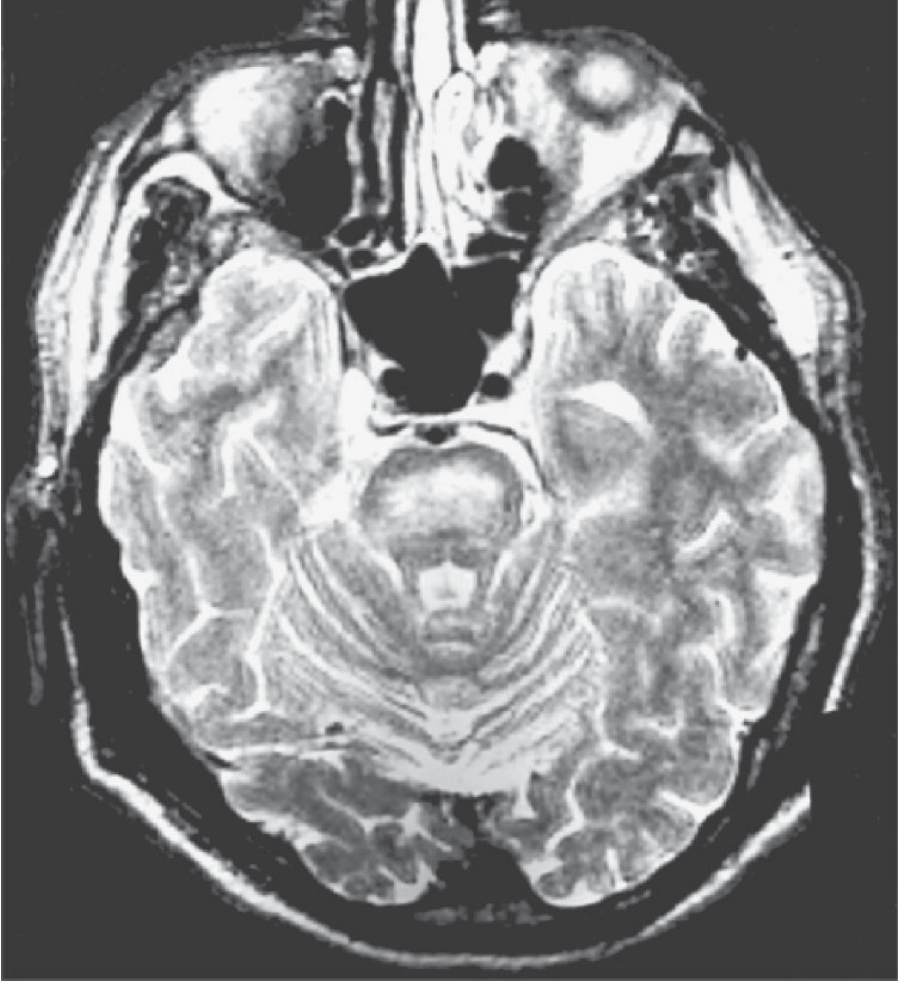
T2-weighted MRI showing the typical lesion of central pontine myelinolysis. (Adams & Victor's Principles of Neurology 12E, Fig. 39-6)
Other investigations: Brainstem auditory evoked potentials can detect lesions encroaching on the pontine tegmentum. CSF is usually normal or shows mildly elevated protein.
Differential Diagnosis
| Condition | Distinguishing features |
|---|---|
| Basilar artery occlusion | Sudden/stepwise onset, asymmetric signs, tegmental + midbrain + thalamic involvement on MRI, DWI follows vascular territory |
| Brainstem glioma | Gradual onset, expansile mass |
| Multiple sclerosis | Inflammatory; periventricular lesions; oligoclonal bands in CSF |
| Wernicke's disease | Periventricular lesions (around 3rd ventricle, aqueduct); responds to thiamine; no sparing of neurons |
Prevention and Treatment
Prevention (the cornerstone)
Safe correction rates for hyponatremia:
- No more than 6-8 mEq/L per 24 hours (current conservative standard; Adams & Victor)
- ≤8 mmol/L within 24 h and ≤15 mmol/L within 48 h (Harrison's 22E, 2025)
- Earlier literature suggested up to 10 mEq/day - current guidelines are stricter
Patients at highest risk (Na <115 mEq/L, alcoholism, malnutrition) require the most conservative correction rates.
Acute Treatment
- There is no specific therapy once CPM develops
- Supportive care: mechanical ventilation if needed, nutritional support, prevention of complications (DVT, aspiration, pressure ulcers)
- Treat the underlying cause (nutritional deficiency, hepatic disease, etc.)
- Desmopressin (DDAVP) can be used to slow or reverse inadvertent over-correction: by causing water retention, it reduces serum sodium back down (relowering). This is most effective if given within a few hours of over-correction
- Thiamine should always be given concomitantly in at-risk patients (alcoholics) to prevent Wernicke's disease
Prognosis
- Outcome is highly variable - ranges from death to complete recovery
- Milder cases (without locked-in syndrome) may recover over months
- The locked-in state may be permanent or show partial improvement
- Two of Adams & Victor's patients with dysarthria and cerebellar ataxia (but no quadriplegia) had near-complete recovery at 6 months
- Since adoption of current conservative correction rates, frequency of CPM has decreased dramatically
Recent Evidence (PubMed, 2023-2026)
A 2025 systematic review and meta-analysis in JAMA Internal Medicine (Ayus et al., PMID 39556338) examined correction rates and clinical outcomes in hospitalized adults with severe hyponatremia - this is the most current high-level evidence on this topic. Recent reviews also address optimal ICU management of severe hyponatremia (Rondon-Berrios, J Intensive Care Med 2024) and best clinical practice for correction (Sumi et al., Clin Exp Nephrol 2025).
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 318
- Adams and Victor's Principles of Neurology 12E, Ch. 39
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10E)
This is a shared conversation. Sign in to Orris to start your own chat.