Shoulder joint kinetics and kinematics
Reading File
Finding Sources
Finding Sources
Searching PubMed
shoulder joint kinematics kinetics biomechanics
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive breakdown of shoulder joint kinetics and kinematics, drawn from multiple authoritative textbooks.
Shoulder Joint: Kinetics and Kinematics
1. Overview of the Shoulder Complex
The shoulder is not a single joint but a complex of four articulations that work in concert:
- Glenohumeral (GH) joint - the primary ball-and-socket articulation
- Acromioclavicular (AC) joint
- Sternoclavicular (SC) joint
- Scapulothoracic (ST) "joint" - a functional articulation
Each of the three true synovial joints (GH, AC, SC) has 3 degrees of freedom of rotation and 3 degrees of translation, giving the shoulder girdle as a whole an exceptionally large workspace for the hand. - Imaging Anatomy: Bones, Joints, Vessels and Nerves, p. 493
2. Kinematics
Glenohumeral Joint
The GH joint is a multiaxial spheroidal joint - the joint with the greatest freedom of movement in the body, but at the expense of stability. Its three cardinal axes allow six principal movement directions:
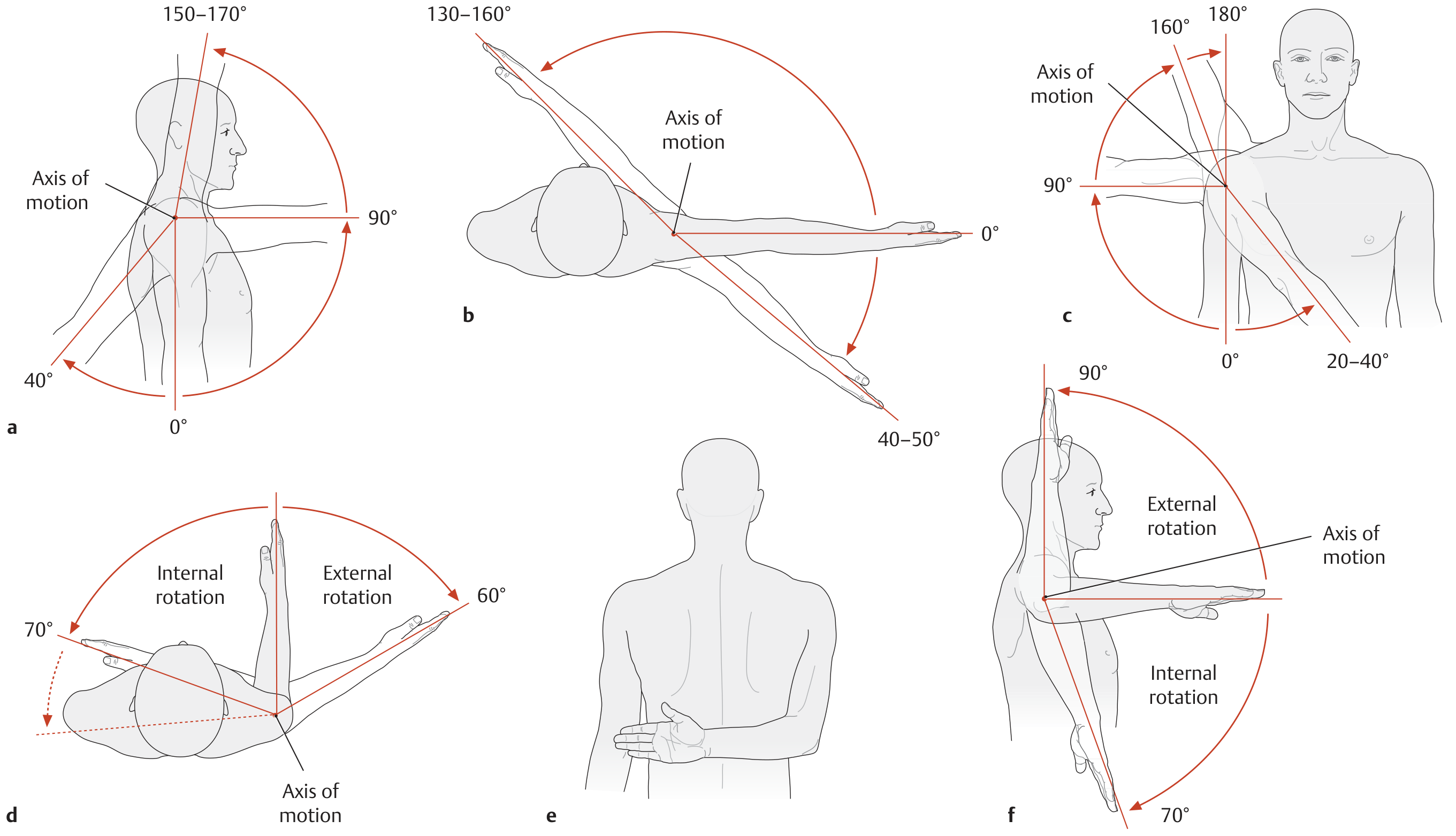
| Movement | Range | Key Muscles | Innervation |
|---|---|---|---|
| Flexion | 90° (>90° = elevation) | Deltoid (clavicular), Biceps brachii, Pectoralis major | Axillary n. (C5-C6), Musculocutaneous n. (C5-C7) |
| Extension | 40° | Latissimus dorsi, Teres major, Triceps (long head), Deltoid (spinal) | Thoracodorsal, Subscapular, Radial, Axillary nn. |
| Abduction | 90° (>90° = elevation) | Deltoid (acromial, above 60°), Supraspinatus, Biceps brachii | Axillary n. (C5-C6), Suprascapular n. |
| Adduction | 20-40° | Latissimus dorsi, Teres major, Pectoralis major, Coracobrachialis | Thoracodorsal, Pectoral, Subscapular nn. |
| Internal Rotation | 50-95° | Subscapularis, Pectoralis major, Deltoid (clavicular), Teres major | Subscapular, Pectoral, Axillary, Thoracodorsal nn. |
| External Rotation | 40-60° | Infraspinatus, Teres minor, Deltoid (spinal) | Suprascapular n. (C5-C6), Axillary n. |
Source: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System, p. 344
Important kinematic detail: Past 80-90° of abduction, automatic external rotation occurs, which rotates the greater tubercle posteriorly so it clears the coracoacromial arch and does not impinge. - THIEME Atlas, p. 296
Humeroscapular (Scapulohumeral) Rhythm
This is one of the most clinically important kinematic concepts:
The arm and scapula move in a 2:1 ratio during abduction. When the arm is abducted 90°, 60° occurs at the GH joint and 30° occurs through scapulothoracic motion (upward rotation of the scapula). - THIEME Atlas, p. 296
- As elevation increases above 90°, the proportion of scapulothoracic motion increases relative to GH motion.
- Disturbance of this normal rhythm can result in secondary impingement.
- Even in complete GH ankylosis/arthrodesis, scapulothoracic motion alone can permit 40-60° of abduction and 1/3 of normal flexion/extension.
- Rheumatology, 2-Volume Set (2022), p. 700
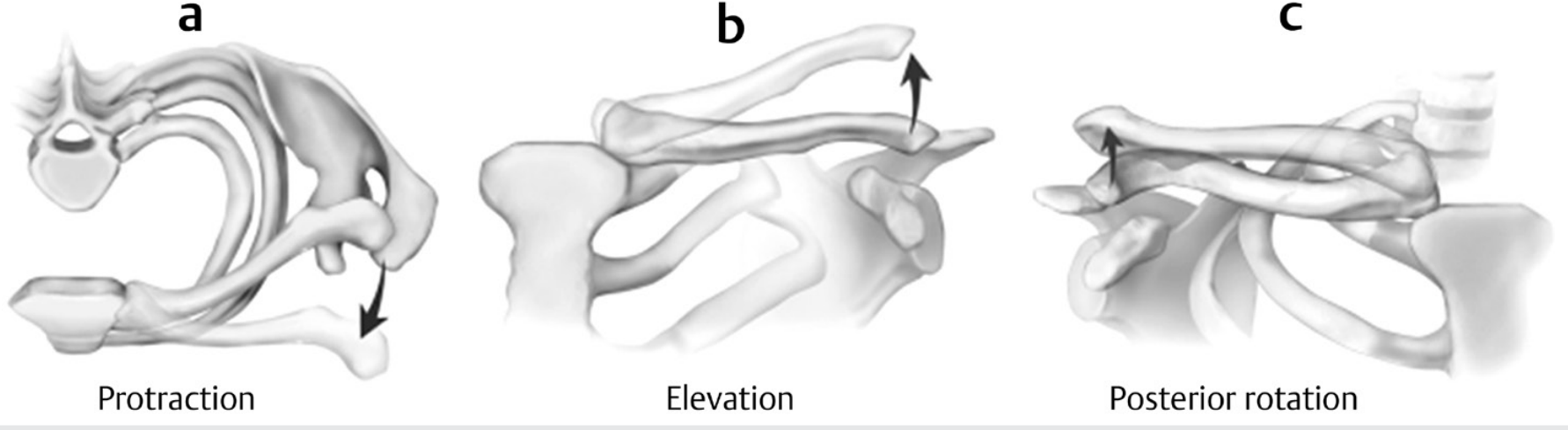
Sternoclavicular Joint Kinematics
The SC joint is a diarthrodial saddle joint with an intraarticular disk. Despite its incongruent surfaces, it functions effectively as a spheroidal joint because of a ~45° axial rotation of the clavicle about its own long axis - particularly during shoulder elevation. This rotation significantly increases the overall range of shoulder elevation.
Clavicular motions at the SC joint:
- Elevation and depression (lateral end moves superiorly/inferiorly)
- Protraction and retraction (lateral end moves anteriorly/posteriorly)
- Posterior/anterior rotation about the clavicular long axis (~45°)
The clavicle moves within a conical shell whose apex points at the sternum, with an oval base ~10-13 cm in diameter. - THIEME Atlas, p. 295
Acromioclavicular Joint Kinematics
The AC joint contains a fibrous disk and allows:
- Anterior/posterior tilting (tipping)
- Internal/external rotation
- Upward/downward rotation of the scapula
During abduction and elevation, the clavicle rotates 30-40°, mostly at the SC joint. The coracoclavicular ligaments (conoid and trapezoid) couple posterior rotation of the clavicle with scapular upward rotation during arm elevation. - Imaging Anatomy, p. 493 and Rheumatology, p. 700
Scapulothoracic "Joint" Kinematics
The scapula slides and rotates against the posterolateral thoracic wall. Its principal motion during arm elevation is upward rotation (lateral rotation of the inferior angle), with coupled:
- Posterior tilting
- External rotation
The inferior angle moves ~10 cm laterally and the superior angle moves ~2-3 cm inferomedially during a 60° upward rotation arc. - THIEME Atlas, p. 295
3. Kinetics
Joint Reaction Forces and the Force Couple
The glenohumeral joint is subjected to large compressive joint reaction forces during overhead activities. The key kinetic concept is the force couple mechanism:
- The deltoid generates a large superiorly directed force vector during abduction.
- Acting alone, this would shear the humeral head superiorly out of the glenoid.
- The rotator cuff muscles (and long head of biceps) act as humeral head depressors, redirecting the vertical deltoid force vector into a rotational (torque-generating) force.
- This transforms what would be a destabilizing shear into a compressive force directed into the glenoid concavity. - Rheumatology, p. 699
"The rotator cuff muscles and the biceps tendon act as humeral head depressors and work to alter the vertically oriented vector from the deltoid muscle into a rotational force." - Rheumatology (2022)
Dysfunction of the rotator cuff (weakness or tear) removes this depression force, resulting in superior migration of the humeral head, increasing subacromial impingement risk.
Glenoid Concavity Compression (Stability via Joint Reaction Force)
A key kinetic stability mechanism: normal synchronous scapular stabilizer function positions the glenoid so the joint reaction force is compressive rather than shear. This "compressive stabilization" is the main dynamic stability mechanism at the GH joint.
- The labrum increases glenoid depth and concavity; loss of labrum reduces this stabilizing effect by ~20%.
- Rotator cuff and biceps must perform synchronous eccentric deceleration and concentric contraction for humeral stability during midranges of motion.
- Scapular dyskinesis (e.g., SICK scapula syndrome: Scapular malposition, Inferior medial border prominence, Coracoid pain, Dyskinesis) tilts the glenoid, converting compressive forces to shear forces and predisposing to instability. - Campbell's Operative Orthopaedics 15th ed. (2026)
Static vs. Dynamic Stabilizers
| Category | Structures | Kinetic Role |
|---|---|---|
| Static | Glenoid labrum, GH ligaments (SGHL, MGHL, IGHL), joint capsule, negative intraarticular pressure, humeral head retroversion | Passive resistance to translation; position-dependent |
| Dynamic | Rotator cuff (subscapularis, supraspinatus, infraspinatus, teres minor), long head of biceps, scapular stabilizers (serratus anterior, trapezii, rhomboids) | Active compressive force generation; force couple; proprioceptive feedback via Ruffini and Pacinian corpuscles |
The IGHL is the primary restraint to external rotation in abduction and is the main check against anteroinferior instability (the classic dislocation position: abduction + external rotation). - Rheumatology (2022), p. 699
Proprioception and Neuromuscular Kinetics
Ruffini end organs and Pacinian corpuscles in the shoulder capsule provide proprioceptive feedback that drives neuromuscular stabilization. This supports the concept of proprioceptive training as a cornerstone of shoulder rehabilitation after injury or instability. - Campbell's Operative Orthopaedics 15th ed. (2026)
Summary
| Concept | Key Value/Principle |
|---|---|
| Scapulohumeral rhythm | 2:1 ratio (GH : ST) |
| Full abduction | ~60° GH + ~30° ST upward rotation = 90° |
| Clavicular rotation at SC | ~45° posterior rotation during full elevation |
| AC joint clavicular rotation | 30-40° during elevation |
| Force couple | Deltoid (elevator) + Rotator cuff (depressor) = net rotation |
| Labral loss impact | Reduces concavity-compression stability by ~20% |
| GH joint DOF | 3 rotational + 3 translational |
The shoulder's extraordinary mobility is the product of tightly choreographed multi-joint kinematics, while its kinetic stability depends on the dynamic force couple and the ability to direct joint reaction forces compressively into the glenoid.
Sources: Rheumatology 2-Volume Set (Elsevier, 2022) | THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System | Imaging Anatomy: Bones, Joints, Vessels and Nerves (THIEME) | Campbell's Operative Orthopaedics 15th ed. (2026)
This is a shared conversation. Sign in to Orris to start your own chat.