Female patient aged 26 years having irregular menses with pn going hypothyroidism and USG shows both ovaries has increased volume
Reading File
Finding Sources
Finding Sources
Searching PubMed
polycystic ovary syndrome AND hypothyroidism
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have comprehensive information. Let me compile a thorough clinical answer.
Clinical Analysis: 26-Year-Old Female with Irregular Menses, Hypothyroidism, and Bilateral Enlarged Ovaries on USG
Likely Diagnosis
The presentation is consistent with Polycystic Ovary Syndrome (PCOS) - but with an important caveat: hypothyroidism must first be assessed as either the primary cause of the irregular menses and ovarian changes, or as a coexisting condition.
Critical point from Harrison's (22nd Ed.): "PCOS is a diagnosis of exclusion, and other etiologies for irregular menses and hyperandrogenism should be excluded - hypothyroidism, hyperprolactinemia, adrenal sources for hyperandrogenism."
Step 1: Is Hypothyroidism the Cause or a Co-condition?
Hypothyroidism by itself can cause:
- Irregular/absent menses (via disruption of GnRH pulsatility and elevated prolactin)
- Ovarian enlargement and polycystic-appearing ovaries on ultrasound
Before diagnosing PCOS, thyroid function must be optimized. Check TSH and free T4. If the patient's hypothyroidism is adequately treated (TSH in normal range) and menstrual irregularity + enlarged ovaries persist, then PCOS diagnosis can be pursued.
A 2025 systematic review and meta-analysis (PMID: 40102852) confirmed a significantly higher prevalence of subclinical hypothyroidism in PCOS patients and noted its impact on insulin resistance - highlighting the bidirectional relationship between these two conditions.
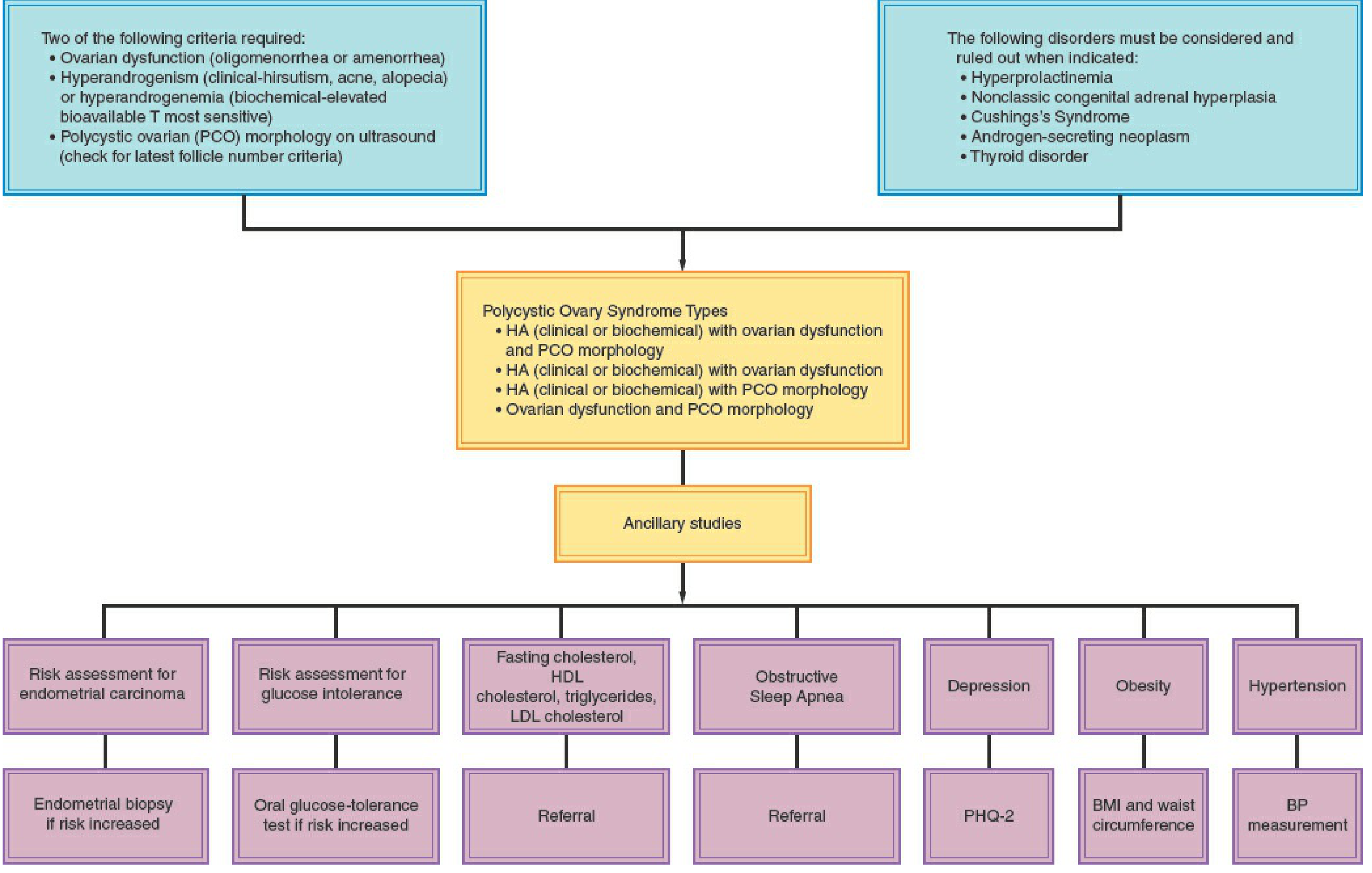
Step 2: Rotterdam Diagnostic Criteria for PCOS
Requires 2 out of 3 of the following (after excluding other causes):
| Criterion | This Patient |
|---|---|
| 1. Oligo/anovulation (irregular cycles) | ✅ Present |
| 2. Clinical/biochemical hyperandrogenism (hirsutism, acne, elevated androgens) | ? - not mentioned, needs assessment |
| 3. Polycystic ovary (PCO) morphology on USG | ✅ Present (bilateral enlarged ovaries) |
USG criteria for PCO morphology: ≥20 follicles (2-9 mm) in either ovary and/or ovarian volume >10 mL. A single ovary meeting these criteria is sufficient. - Berek & Novak's Gynecology
This patient already fulfills criteria 1 + 3 (ovarian dysfunction + PCO morphology), which is one of the four recognized Rotterdam phenotypes.
Diagnostic algorithm from Berek & Novak's Gynecology:
Step 3: Investigations to Order
To confirm PCOS and rule out mimics:
| Test | Reason |
|---|---|
| TSH + Free T4 | Assess thyroid control (already on treatment - ensure adequate) |
| Serum LH / FSH | LH:FSH ratio >2:1 suggests PCOS |
| Total + free testosterone, DHEAS | Assess hyperandrogenism |
| Serum prolactin | Rule out hyperprolactinemia |
| 17-OH progesterone (follicular phase) | Rule out non-classic congenital adrenal hyperplasia |
| Fasting glucose + 2-hr OGTT | Screen for insulin resistance / type 2 DM |
| Fasting lipid profile | Cardiovascular risk assessment |
| Anti-Mullerian Hormone (AMH) | Elevated in PCOS; correlates with antral follicle count |
| Pelvic USG | Already done - bilateral enlarged ovaries |
Step 4: Pathophysiology of PCOS
The four compartments contributing to PCOS - Berek & Novak's Gynecology:
- Ovaries - primary androgen source; dysregulation of CYP17 (androgen-forming enzyme)
- Adrenal glands - excess DHEAS in some patients
- Periphery (adipose tissue) - converts androgens to estrogens; worsened by obesity
- Hypothalamus-pituitary - elevated LH pulse frequency, elevated LH:FSH ratio
Macroscopic ovarian findings: Ovaries are 2-5x normal size, white thickened cortex, multiple small cysts (<1 cm). Microscopically: fibrotic cortex, increased follicles with luteinized theca interna.
Insulin resistance - present in most PCOS patients; hyperinsulinemia stimulates ovarian androgen production and suppresses hepatic SHBG synthesis, further increasing free androgens.
Step 5: Management
A. Optimize Thyroid Treatment First
- Ensure TSH is in target range (ideally 1-2.5 mIU/L for a woman of reproductive age)
- Reassess menstrual pattern and ovarian morphology after 3-6 months of euthyroid state
B. If PCOS diagnosis confirmed:
| Goal | Treatment |
|---|---|
| Regulate cycles (not trying to conceive) | Combined oral contraceptive pill (OCP) - lowest effective estrogen dose |
| Endometrial protection | OCP, or cyclic progestins (medroxyprogesterone 10 mg × 10-14 days every 3 months) |
| Hyperandrogenic symptoms (hirsutism/acne) | OCP ± spironolactone / flutamide if inadequate response at 6 months |
| Insulin resistance / metabolic risk | Metformin (especially if overweight/obese) + lifestyle changes |
| Fertility / ovulation induction | Letrozole (first-line) > Clomiphene citrate ± metformin; injectable gonadotropins as second-line |
C. Lifestyle - all PCOS patients:
- Weight loss (even 5-10% body weight improves hormonal profile and menstrual regularity)
- Regular aerobic exercise
- Low glycemic index diet
D. Monitoring:
- Screen for obesity, hypertension, glycemia, dyslipidemia, depression/anxiety at diagnosis and periodically
- Endometrial biopsy if at increased risk for endometrial carcinoma (prolonged unopposed estrogen)
- Oral GTT if impaired glucose tolerance suspected (~1/3 of obese PCOS patients have IGT; 7.5-10% develop T2DM)
Key Points Summary
- In this patient, hypothyroidism may be contributing to or mimicking PCOS - adequate thyroid control is the first step
- Once euthyroid state is confirmed, she likely has PCOS (phenotype 4: ovarian dysfunction + PCO morphology)
- Screen for hyperandrogenism clinically (hirsutism/acne/alopecia) and biochemically (testosterone)
- Long-term risks include insulin resistance, type 2 DM, dyslipidemia, cardiovascular disease, and endometrial carcinoma from chronic anovulation
- A 2025 meta-analysis (PMID: 40102852) confirms subclinical hypothyroidism is significantly more prevalent in PCOS and worsens insulin resistance - supporting the importance of tight thyroid control in this patient
Sources: Berek & Novak's Gynecology; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Goodman & Gilman's Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.