Defibrillator principles, types, application
Reading File
Finding Sources
Searching the Web
defibrillator principles types waveforms AED ICD clinical application 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have excellent content now. Let me compile the full response.
Defibrillator: Principles, Types, and Application
1. Basic Principle
Defibrillation works by passing a controlled electrical current through a critical mass of myocardium, causing simultaneous depolarization of myofibrils. This momentarily "resets" the chaotic electrical activity of ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT), allowing the heart's natural pacemaker (the SA node) to re-establish an organized rhythm.
Key distinction: Defibrillation is NOT "jumpstarting" the heart. It is not indicated for asystole or pulseless electrical activity (PEA), which have no chaotic electrical activity to terminate.
2. Electrical Physics
Defibrillators derive power from AC mains or an internal battery, store charge in a capacitor, and discharge it through electrodes. The critical relationships are:
| Quantity | Formula |
|---|---|
| Energy (J) | Power (W) × Duration (s) |
| Current (A) | Voltage (V) / Resistance (Ω) |
| Delivered current | = √[Energy / (Resistance × Duration)] |
Key implication: The actual determinant of successful defibrillation is current (amperes), not energy (joules). However, because current cannot be directly set, defibrillators are calibrated in joules. Higher transthoracic impedance reduces delivered current even at the same energy setting.
Transthoracic impedance averages 70-80 ohms in adults (range 15-143 Ω). It is reduced by:
-
Larger electrode surface area (optimal paddle diameter ~13 cm)
-
Firm paddle pressure (~25 lb/11 kg)
-
Conductive gel or saline pads
-
Shocking at end-expiration (air is a poor conductor)
-
Repeated shocks (impedance falls with each successive shock)
-
Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
3. Waveform Types
All modern defibrillators deliver one of three waveforms:
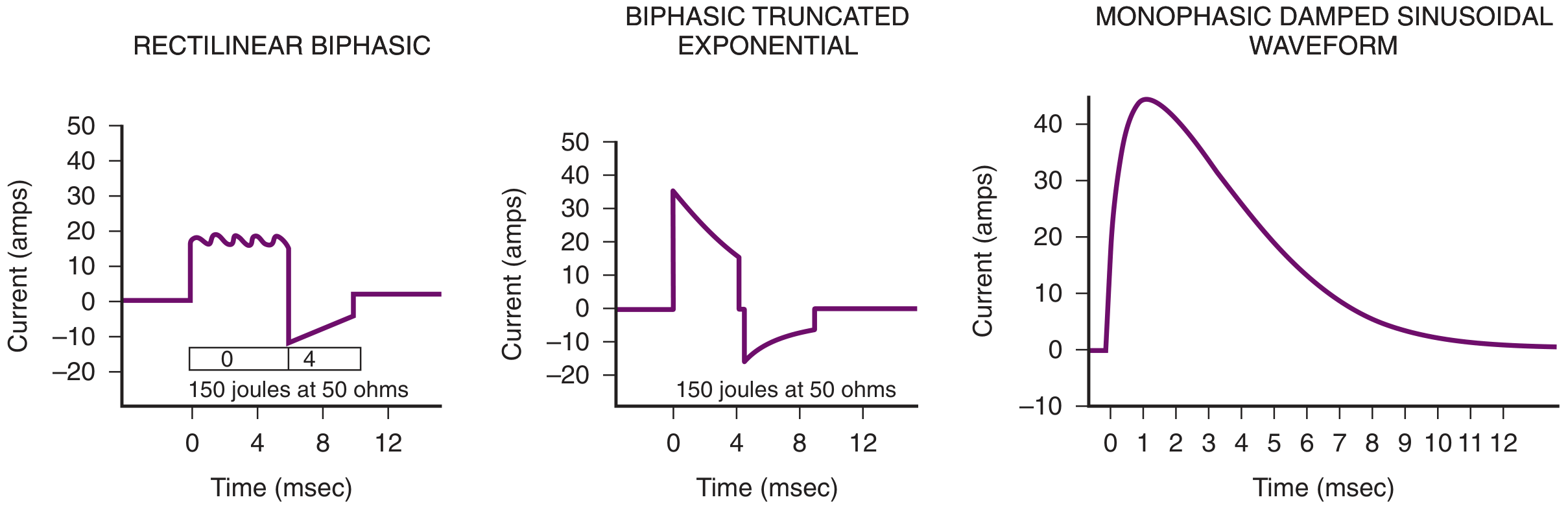
Monophasic (legacy)
- Current flows in one direction only between electrodes
- Subtypes: Monophasic Damped Sinusoidal (MDS) and Monophasic Truncated Exponential
- Requires higher energy: 360 J recommended for all shocks (MDS)
- Historical use: stacked shocks at 200 J → 200-300 J → 300-360 J (pre-2005 AHA)
- Still found in some older equipment
Biphasic (current standard)
- Current flows forward then reverses between electrodes within the same shock
- Two subtypes in clinical use:
- Biphasic Truncated Exponential (BTE): 150-200 J for first shock
- Rectilinear Biphasic (RLB): 120 J for first shock
- If waveform type unknown: default 200 J
- Lower energy requirements = less myocardial damage
- Higher first-shock success rate than monophasic
- All current AEDs and most hospital defibrillators use biphasic waveforms
"Current data do not support one waveform over another, but biphasic defibrillators appear to be more efficient in achieving defibrillation with the first shock." - Roberts and Hedges' Clinical Procedures in Emergency Medicine
4. Types of Defibrillators
A. Manual External Defibrillator
- Requires trained operator to interpret the rhythm and manually deliver the shock
- Delivers shock via handheld paddles or self-adhesive pads
- Used in hospitals, ICUs, and by advanced paramedics
- Allows fine energy titration and cardioversion in synchronized mode
B. Automated External Defibrillator (AED)
- Monitors ECG, automatically recognizes VF, charges, and (in fully automatic models) delivers shock - or prompts the operator to press a button (semi-automatic)
- Designed for minimally trained lay rescuers
- VF-detection algorithms have near-perfect specificity (will not shock a non-shockable rhythm) but somewhat lower sensitivity for low-amplitude VF
- Rhythm analysis can take up to 90 seconds, during which CPR is interrupted - a recognized limitation
- Can misinterpret pacemaker spikes as QRS complexes
- Delivers biphasic waveform at a pre-set impedance-compensated energy level
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
C. Implantable Cardioverter-Defibrillator (ICD)
- Surgically implanted device (subclavicular pocket, transvenous lead to RV) that continuously monitors rhythm
- Delivers tiered therapy:
- Anti-tachycardia pacing (ATP): overdrive pacing to terminate VT without a shock (patient often unaware)
- Low-energy cardioversion: synchronized shock for VT
- High-energy defibrillation: for VF
- Stores electrograms for later interrogation
- Appropriate shock occurs in ~50% of patients within 2 years of implantation
- Subcutaneous ICD (S-ICD) is available, requiring no transvenous leads
ICD indications (primary/secondary prevention):
- Survived cardiac arrest due to VF/pVT (secondary prevention)
- EF ≤35% with symptomatic heart failure (NYHA II-III) on optimal therapy
- Hypertrophic cardiomyopathy with risk factors
- Channelopathies (Long QT, Brugada, catecholaminergic VT)
D. Wearable Cardioverter-Defibrillator (WCD)
- External vest worn by patients at temporary high risk (e.g., post-MI before reassessment of EF, new cardiomyopathy)
- Bridges to ICD implantation or recovery
E. Combined CRT-D (Cardiac Resynchronization Therapy with Defibrillator)
- Biventricular pacing device that also has ICD capability
- For patients with EF ≤35%, wide QRS/LBBB, and NYHA class II-IV symptoms
- Improves symptoms, exercise capacity, and reduces mortality
5. Indications and Contraindications
Defibrillation (unsynchronized)
| Indication | Notes |
|---|---|
| Ventricular fibrillation (VF) | Primary indication |
| Pulseless ventricular tachycardia (pVT) | Treated same as VF |
Contraindications: Asystole, PEA, conscious patient with a pulse, wet patient/wet environment (safety risk)
Cardioversion (synchronized)
- Timed to QRS complex to avoid R-on-T phenomenon (which would induce VF)
- Indications: Hemodynamically unstable VT with pulse, SVT, atrial flutter, atrial fibrillation
- Also used electively after failed pharmacologic cardioversion
IMPORTANT: Always confirm "SYNC" mode is OFF for defibrillation, and ON for cardioversion. If SYNC is accidentally left on during VF, the device searches for a QRS and will not fire.
6. Electrode Placement
Two standard positions:
Sternum-Apical (most common)
- Sternal pad: below right clavicle, right of sternum
- Apical pad: midaxillary line, 5th-6th intercostal space (left)
Anterior-Posterior
- Anterior pad: left of sternum
- Posterior pad: directly behind, at the same level
- Preferred when pacemaker/ICD is present (avoids over the device) or in certain body habitus
Avoid pad-to-pad conductive gel smearing across the chest, which can cause arcing and burns.
7. Step-by-Step Defibrillation Procedure
- Confirm unresponsiveness, absent pulse (<10 sec check), call for help, start CPR
- Apply pads/electrodes in sternum-apical position
- Select energy: 200 J (biphasic default) or 360 J (monophasic)
- Confirm SYNC mode is OFF
- Press CHARGE, announce "I'm clear, you're clear, everybody's clear!"
- Visually confirm all contacts broken, press SHOCK
- Resume CPR immediately after shock - do not pause to check pulse first
- Continue 5 cycles (2 minutes) of CPR, then reassess rhythm
- If shockable rhythm persists: repeat shock (same or escalating energy), continue CPR, administer epinephrine, consider amiodarone
8. Complications
| Complication | Notes |
|---|---|
| Skin burns | Reduced by conductive gel/pads; self-adhesive pads preferred |
| Myocardial injury | Higher with high-energy/repeated shocks; minimal at recommended doses |
| Post-shock arrhythmias | AV block more common with high-energy shocks |
| Induced VF | Risk with unsynchronized cardioversion if R-on-T; prevented by synchronization |
Biphasic waveforms substantially reduced complications versus monophasic by achieving defibrillation at lower energies with fewer shocks. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
9. Special Considerations
- Pacemakers/ICDs: Place pads at least 8 cm from implanted device. Consider anterior-posterior placement. Interrogate device post-shock.
- Pregnancy: Standard defibrillation is safe; fetal monitors should be removed before shock.
- Children: Recommended dose 2-4 J/kg for biphasic; AEDs with pediatric attenuator pads preferred
- Low-amplitude VF: More likely to convert to asystole, associated with poor prognosis; epinephrine does NOT improve defibrillation threshold despite theoretical rationale
- ICD storm (≥3 appropriate shocks in 24 h): Indicates recurrent VT/VF; requires hospital admission, antiarrhythmics or ablation
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Barash, Cullen & Stoelting's Clinical Anesthesia 9e; Tintinalli's Emergency Medicine; Morgan & Mikhail's Clinical Anesthesiology 7e; Braunwald's Heart Disease
APPLICATION OF ULTRASOUND IN ANESTHESIA
Finding Sources
Searching the Web
ultrasound applications anesthesia regional blocks vascular access POCUS 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive response. Let me compile it.
Application of Ultrasound in Anesthesia
Overview
Echocardiography and point-of-care ultrasound (POCUS) have become essential tools in modern anesthesia practice. After early adoption in cardiac surgery, the last four decades have seen ultrasound spread across perioperative assessment, non-cardiac surgery, critical care, vascular access, and regional anesthesia. It is now considered an integral component of the anesthesiologist's skill set.
"Echocardiography and point-of-care ultrasound (POCUS) have become essential parts of perioperative and peri-interventional anesthesia practice." - Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
1. Physics of Ultrasound Relevant to Anesthesia
Basic Principles
- Ultrasound is sound with frequency above 20 kHz; diagnostic ultrasound uses 2-10 MHz for cardiac/general imaging and >10 MHz for peripheral nerve imaging
- Transducers use piezoelectric elements (PZEs) - crystals that expand/contract with alternating current, generating sound pulses
- The machine measures time of return of reflected signals to calculate depth, assuming a fixed tissue sound velocity of 1,540 m/s
- The fundamental relationship: v = f × λ (velocity = frequency × wavelength)
Key Image Properties
| Property | Determinant | Trade-off |
|---|---|---|
| Axial (depth) resolution | Frequency (wavelength) | Higher frequency = better resolution but less penetration |
| Lateral resolution | Beam width / scan-line density | Linear arrays > curved arrays |
| Temporal resolution | Frame rate | Narrow sector + shallow depth = faster refresh |
Echogenicity
| Structure | Appearance | Reason |
|---|---|---|
| Bone, calcium, metal | Bright (hyperechoic) + posterior shadow | High acoustic impedance, reflects most sound |
| Blood, fluid, urine | Black (anechoic) | Homogeneous, no impedance interface |
| Fat | Intermediate gray | Moderate impedance |
| Peripheral nerve | Honeycomb pattern | Internal fascicular structure + epineurium |
| Needle shaft | Variable; brighter at steep angles | Specular reflection |
Artifacts in Anesthesia Practice
- Acoustic shadow: behind bone or calcified structures - limits imaging
- Acoustic enhancement: bright area deep to fluid (vessels) - can mimic nerve
- Reverberation / comet-tail: sound bouncing between parallel reflectors (common with needle shafts, pleural line, air)
- Mirror-image artifact: most relevant in TEE during aortic imaging - can mimic aortic dissection
- Bayonet artifact: apparent bending of needle due to local speed-of-sound heterogeneity
Imaging Modes
| Mode | Use |
|---|---|
| 2D (B-mode) | Standard real-time anatomic imaging |
| M-mode | Motion of single scan line vs. time; valve leaflet motion, IVC collapsibility |
| Color Doppler | Direction and mean velocity of blood flow (color-encoded) |
| Power Doppler | Sensitive flow detection regardless of direction; nerve vascularity |
| Pulsed Wave (PW) Doppler | Velocity at a specific point; LVOT VTI, valve gradients |
| Continuous Wave (CW) Doppler | High-velocity flow (aortic stenosis); aliasing-free |
| Tissue Doppler (TDI) | Myocardial velocities; diastolic function (e'/a') |
Barash, Cullen & Stoelting's Clinical Anesthesia, 9e; Miller's Anesthesia, 10e
2. Transducer Selection
| Probe Type | Frequency | Use |
|---|---|---|
| High-frequency linear (15-6 MHz) | High | Peripheral nerves, superficial vessels, vascular access |
| Compact linear ("hockey stick") | High | Confined spaces (axilla, popliteal fossa) |
| Curved array (curvilinear) | Low-mid | Abdominal organs, deep structures, lung |
| Phased array (sector) | Low | Cardiac (TEE/TTE), deep thoracic structures |
| Micro-convex | Mid | Neonatal/pediatric cardiac, limited windows |
Rule: Select the highest frequency that still provides adequate penetration for the target depth. A "keyhole view" (depth > footprint) limits guidance quality.
3. Regional Anesthesia
This is the most widely practiced ultrasound application in anesthesia. Ultrasound replaced the older paresthesia-seeking and nerve stimulator approaches for most blocks.
Why Ultrasound for Regional Blocks?
- Direct visualization of the peripheral nerve, needle tip, and local anesthetic spread in real time
- Identifies anatomic variations in nerve position - a major source of block failure with landmark technique
- Allows visualization of fascial planes for interfascial blocks
- Reduces procedure time and increases first-attempt success
- Detects intravascular injection (local anesthetic should not enter vessel lumen)
"Anatomic variation in nerve position and course, which is a potential source of block failure, can be directly visualized." - Miller's Anesthesia, 10e
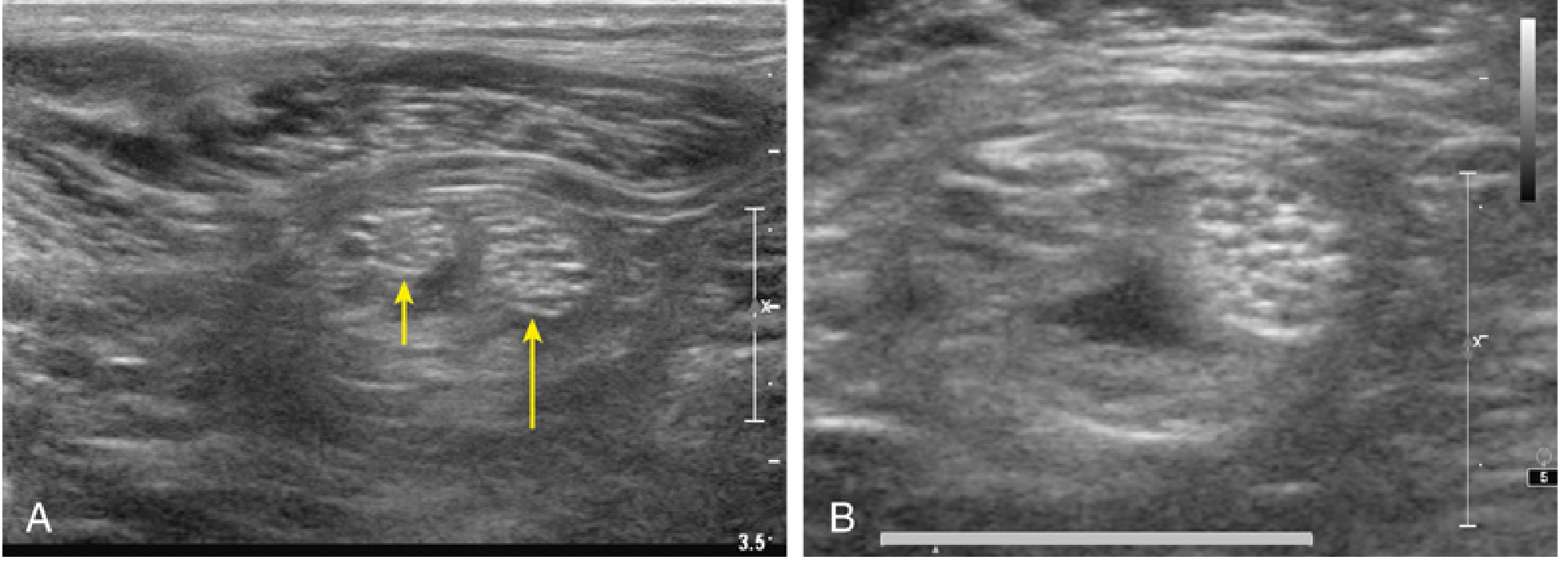
Nerve Appearance on Ultrasound
Peripheral nerves have a honeycomb echotexture formed by hypoechoic nerve fascicles surrounded by hyperechoic epineurium. This is best seen in short-axis (cross-sectional) view.
- Frequencies ≥10 MHz can distinguish nerves from tendons based on echotexture alone
- Ultrahigh frequency (>20 MHz) can resolve 50-60% of individual fascicles
- Nerves are not easily compressed (unlike veins) and are mobile with extremity movement
- Doppler can detect the nerve's vascular supply (useful for proximal sciatic nerve)
Signs of Nerve Pathology (Caution Before Blocking)
- Fusiform enlargement with unclear nerve borders
- Fascicular crowding from edema
- Hyperemia on Doppler (seen in entrapment neuropathy, Charcot-Marie-Tooth, diabetic neuropathy)
Needle Approaches
| Technique | Description | Advantages |
|---|---|---|
| In-plane (IP) | Needle travels within the ultrasound image plane; entire shaft visible | Full needle visibility; preferred for most blocks |
| Out-of-plane (OOP) | Needle crosses the image plane; appears as a bright dot | Useful in constrained spaces |
| Offline marking | Skin marked before needle insertion | Faster but relies on correct identification |
Echogenic needles with textured surfaces (retroreflective design) are commercially available and improve tip detection, especially at steep angles.
Confirming correct injection: Successful local anesthetic injection should:
- Surround and clarify the nerve border ("doughnut sign")
- Track along the nerve path and branches
- Separate the nerve from adjacent structures (e.g., adjacent artery)
Common Ultrasound-Guided Blocks in Anesthesia
Upper Extremity
| Block | Target | Indication |
|---|---|---|
| Interscalene | C5-C6-C7 nerve roots | Shoulder surgery |
| Supraclavicular | Brachial plexus trunk/division level | Hand, forearm, elbow surgery |
| Infraclavicular | Brachial plexus cords around axillary artery | Elbow, forearm, hand |
| Axillary | Terminal branches of brachial plexus | Hand and forearm surgery |
| WALANT variants | Median, ulnar, radial nerves | Hand surgery without tourniquet |
Lower Extremity
| Block | Target | Indication |
|---|---|---|
| Femoral / FNB | Femoral nerve lateral to femoral artery | Hip, knee surgery |
| Adductor canal | Saphenous nerve in adductor canal | Knee surgery (motor-sparing) |
| Popliteal sciatic | Sciatic bifurcation in popliteal fossa | Foot and ankle surgery |
| Ankle block | 5 terminal nerves around ankle | Foot surgery |
Trunk / Neuraxial
| Block | Target | Indication |
|---|---|---|
| TAP (Transversus Abdominis Plane) | Between internal oblique and transversus layers | Abdominal surgery analgesia |
| PECS I & II | Medial/lateral pectoral nerves; intercostals | Breast surgery |
| Serratus anterior plane | Long thoracic nerve; intercostals T2-T9 | Thoracic/rib pain |
| Erector Spinae Plane (ESP) | Dorsal rami + medial branches | Thoracic and lumbar analgesia |
| Quadratus Lumborum (QL) | QL fascial plane | Abdominal/hip surgery |
| Paravertebral | Spinal nerve roots unilaterally | Thoracotomy, mastectomy |
Neuraxial (Ultrasound-Assisted)
- Pre-procedure scanning of the lumbar spine to identify midline, intervertebral level, and depth to ligamentum flavum - especially in obese patients and those with scoliosis
- Does NOT eliminate fluoroscopy for epidurals but reduces attempts and improves success
Local Anesthetic Considerations
- Bupivacaine / Ropivacaine: long-acting (up to 24 hours); standard for most peripheral blocks
- Epinephrine (1:200,000-1:400,000): prolongs block, reduces systemic absorption; contraindicated for ring blocks, ankle blocks, penile blocks (vasoconstriction risk)
- Additives (dexamethasone, clonidine, dexmedetomidine): can prolong block by 4-8 hours
4. Vascular Access
Ultrasound-guided vascular access is now considered standard of care for central venous catheter (CVC) placement in many institutions.
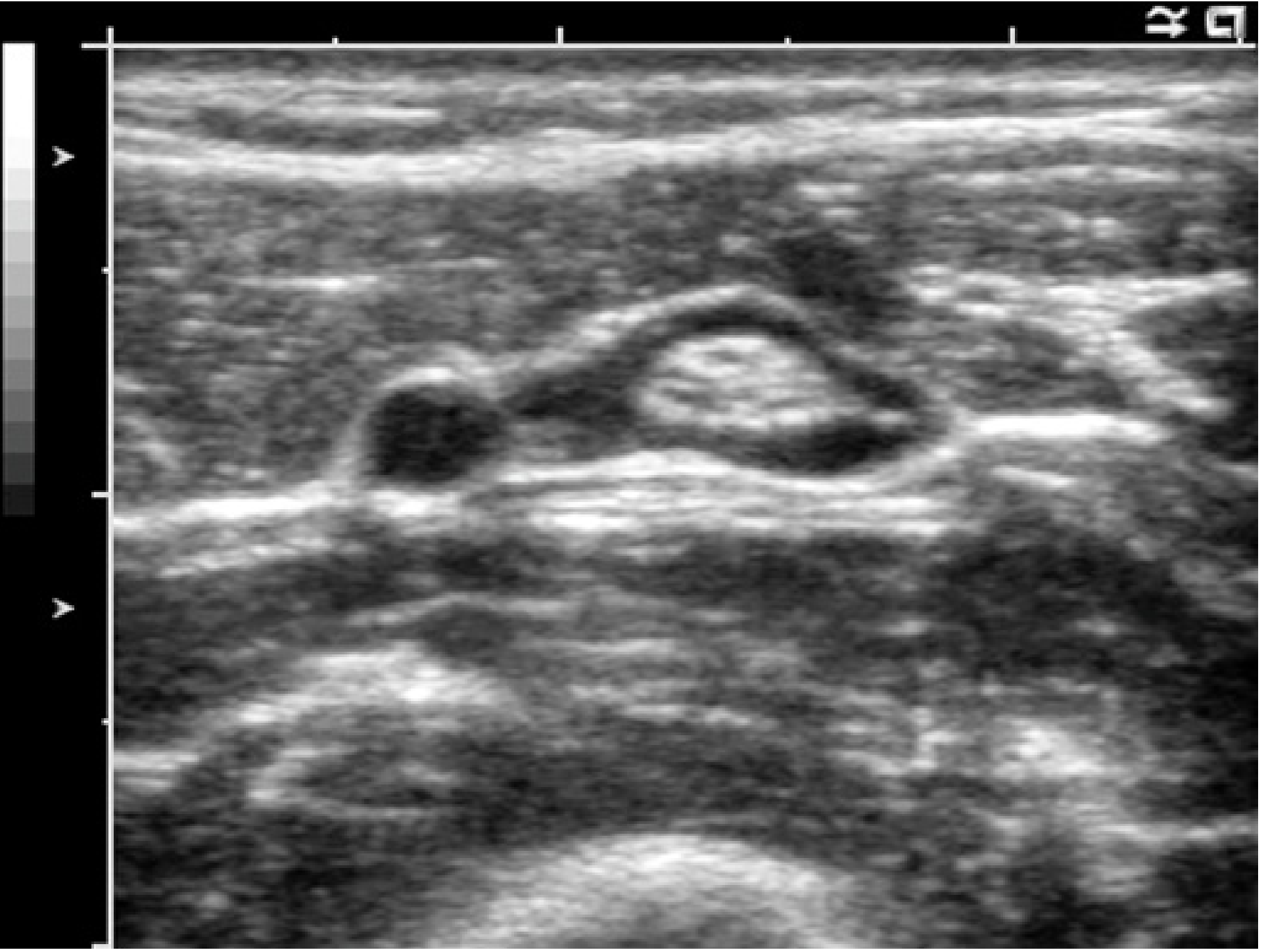
Central Venous Access
- Internal jugular vein (IJV): most studied; short-axis approach allows visualization of IJV collapsibility and differentiation from carotid artery
- Subclavian/infraclavicular axillary: reduces pneumothorax risk vs. landmark technique
- Femoral: useful in cardiac arrest; less affected by body habitus
Benefits over landmark technique:
- Reduced number of attempts
- Lower rate of arterial puncture
- Lower pneumothorax rate (for subclavian)
- Fewer overall mechanical complications
Arterial Line Placement
- Radial, femoral, and brachial arteries visualized directly
- Reduces hematoma formation and multiple attempts, especially in hypotensive/vasoconstricted patients
Peripheral IV Access
- Valuable in patients with difficult venous access
- Basilic and cephalic veins in the upper arm can be cannulated under direct vision
5. Perioperative Echocardiography
Transesophageal Echocardiography (TEE)
TEE is the primary intraoperative echocardiographic modality because the esophagus lies posterior to the heart, providing excellent image quality without the interference of ribs, lungs, or chest wall.
Indications:
- Cardiac surgery (valve repair/replacement, CABG, aortic surgery, LVAD, ECMO)
- Hemodynamically unstable patients of unknown cause
- Diagnosis of suspected intraoperative air embolism
- Guide to intracardiac procedures (ASD closure, TAVR, MitraClip)
- Assess adequacy of valve repair immediately after surgery
Key assessments:
- LV systolic function (qualitative EF assessment, wall motion abnormalities)
- RV function and size
- Valve morphology and regurgitation/stenosis severity
- Fluid responsiveness (IVC collapsibility index, LVOT VTI changes with passive leg raise)
- Detection of aortic pathology (dissection, atheroma)
Transthoracic Echocardiography (TTE) / POCUS
POCUS for perioperative cardiac assessment covers:
- Qualitative LV systolic function (visual EF)
- Detection of severe LV/RV dysfunction, tamponade, massive PE
- IVC assessment for volume status
- Gross valvular pathology
- Rule out intracardiac thrombus or masses
Five core POCUS cardiac windows:
- Parasternal long axis (PLAX)
- Parasternal short axis (PSAX)
- Apical four-chamber (A4C)
- Subcostal four-chamber
- Subcostal IVC view
Doppler in Perioperative Echo
| Doppler Mode | Measurement | Clinical Use |
|---|---|---|
| CW across aortic valve | Peak velocity, mean gradient | Severity of aortic stenosis |
| PW at LVOT | VTI (stroke volume index) | Fluid responsiveness, cardiac output |
| PW at mitral inflow | E/A ratio | Diastolic function grade |
| Tissue Doppler (mitral annulus) | e' velocity | Diastolic function (E/e' ratio = filling pressure) |
| Color Doppler | Regurgitant jets | Valve lesion severity |
6. Pulmonary / Lung Ultrasound
Lung ultrasound is increasingly used perioperatively and in the ICU.
| Finding | Pattern | Interpretation |
|---|---|---|
| Lung sliding + A-lines | Normal | Air-filled lung, no pneumothorax |
| No lung sliding + barcode sign (M-mode) | Absent sliding | Pneumothorax (or mainstem intubation on one side) |
| B-lines (comet tails, ≥3 per field) | Interstitial pattern | Pulmonary edema, interstitial lung disease |
| Consolidation | Tissue-like | Pneumonia, atelectasis |
| Pleural effusion | Anechoic space above diaphragm | Free fluid - quantifiable |
Perioperative use:
- Confirm bilateral lung sliding after intubation (rules out right mainstem intubation and pneumothorax)
- Diagnose cause of intraoperative desaturation (atelectasis vs. pneumothorax vs. pulmonary edema)
- Guide thoracentesis and chest drain placement
7. Airway Assessment
Ultrasound can contribute to pre-anesthetic airway assessment:
- Measure soft tissue thickness from skin to anterior trachea at vocal cord level (predicts difficult laryngoscopy in obese patients)
- Identify cricothyroid membrane for emergency front-of-neck access (FONA)
- Confirm tracheal intubation vs. esophageal intubation by visualizing tracheal ring movement and absence of "double-tract" sign (two air columns = esophageal intubation)
- Assess for subglottic stenosis and neck masses displacing the trachea
- Confirm ETT tip position (bilateral lung sliding confirms bilateral ventilation)
8. Gastric Ultrasound
Preoperative gastric ultrasound assesses aspiration risk:
- Performed with a curvilinear probe in the right lateral decubitus position, viewing the antrum
- Empty stomach: flat collapsed antrum (Grade 0)
- Clear fluid only: single layer (Grade 1)
- Solid content or thick fluid: complex content (Grade 2) = high aspiration risk; requires RSI or delay
This is particularly useful when fasting history is uncertain (emergency cases, delayed gastric emptying in diabetics, opioid use, obesity).
9. Limitations and Safety
| Limitation | Notes |
|---|---|
| Operator dependency | Image quality and interpretation require training; learning curve is substantial |
| Air and bone | Block ultrasound propagation; cannot image behind ribs or through lungs (unless B-lines/consolidation) |
| Deep structures | Limited by attenuation; lower frequencies needed sacrifice resolution |
| Needle tip visualization | Difficult at steep insertion angles; mitigated by echogenic needles |
| No evidence of superiority for nerve injury prevention | No technique (paresthesia, nerve stimulator, US) has proven superiority in preventing nerve damage |
Safety: Diagnostic ultrasound uses non-ionizing sound energy. At frequencies and powers used clinically, there are no documented harmful thermal or mechanical effects on tissue.
10. Training and Competency
Major societies (ASRA, ESA, ESAIC) recommend structured training for ultrasound-guided regional anesthesia and perioperative POCUS. Competency typically requires:
- Didactic physics and anatomy education
- Supervised clinical procedures (minimum case numbers vary by block)
- Image acquisition and interpretation assessment
- The PERSEUS Guidelines (ESAIC, 2024) provide current evidence-based recommendations for ultrasound in vascular access and regional anesthesia
Sources: Miller's Anesthesia, 10e (Chapters 42, 33); Barash, Cullen & Stoelting's Clinical Anesthesia, 9e (Chapter 27); Morgan & Mikhail's Clinical Anesthesiology, 7e; Campbell's Operative Orthopaedics, 15e
This is a shared conversation. Sign in to Orris to start your own chat.