Intussusception
Reading File
Finding Sources
Searching PubMed
intussusception
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive, well-illustrated information from multiple authoritative textbooks. Here is the complete answer:
Intussusception
Definition
Intussusception is the telescoping of a proximal segment of bowel (the intussusceptum) into the lumen of an adjacent distal segment (the intussuscipiens). This causes bowel obstruction and, if prolonged, vascular compromise leading to ischaemia, gangrene, and perforation.
Epidemiology
- The second most common cause of acute abdomen in children after appendicitis (Rosen's Emergency Medicine)
- Peak incidence: 5-9 months of age; >50% occur under 1 year, <25% after age 2 years
- Most common type: Ileocolic (~77%) (see table below)
- In adults, intussusception is uncommon and almost always associated with a pathological lead point (neoplasm or malignancy)
Types of intussusception in children (Gross, n=702):
| Type | % of cases |
|---|---|
| Ileocolic | 77% |
| Ileoileocolic | 12% |
| Ileoileal | 5% |
| Colocolic | 2% |
| Multiple | 1% |
| Retrograde | 0.2% |
| Others | 2.8% |
Bailey and Love's Short Practice of Surgery, 28th ed.
Aetiology & Lead Points
In children (idiopathic majority):
- >90% have no focal lead point - caused by lymphoid hypertrophy (Peyer's patches), usually following a viral infection (viral gastroenteritis, URTI)
- Rotavirus vaccine administration has also been implicated in the pathogenesis
- A secondary lead point is found in 5-12% of cases, and is more common in:
- Older children (>6-7 years)
- Recurrences
Common pathological lead points:
- Meckel's diverticulum (most common)
- Intestinal polyp
- Duplication cyst
- Intestinal lymphoma
- Henoch-Schönlein purpura (submucosal haemorrhage)
- Inflamed appendix
- Ectopic pancreatic or gastric tissue
- Foreign body
- Nasojejunal tubes (in postoperative cases)
In adults:
- Nearly always secondary to a pathological lead point
- Neoplasm or malignancy are the leading causes
- Requires surgical management in most acute presentations
Sabiston Textbook of Surgery; Grainger & Allison's Diagnostic Radiology; Bailey and Love's Surgery
Pathophysiology
The telescoped bowel compresses the mesentery, leading to:
- Venous obstruction → oedema and congestion
- Arterial ischaemia → if not reduced promptly
- Gangrene and perforation → in delayed or untreated cases
The condition may deteriorate rapidly, particularly in infants, becoming life-threatening with hypovolaemia and shock.
Clinical Features
Classic triad (present in only ~20% of patients):
- Colicky abdominal pain - infant draws up knees during episodes, quiet between attacks
- Vomiting
- Bloody mucus per rectum ("currant jelly stools") - a late sign indicating mucosal ischaemia
Other features:
- Palpable right upper quadrant/abdominal mass (sausage-shaped) - present in <50%
- Dehydration and lethargy
- Signs of shock if delayed presentation
- A "Dance's sign" - emptiness in the right iliac fossa (caecum displaced)
Diagnosis
Ultrasound - Investigation of choice
Sensitivity and specificity of 100% in several reported studies. Key sonographic appearances:
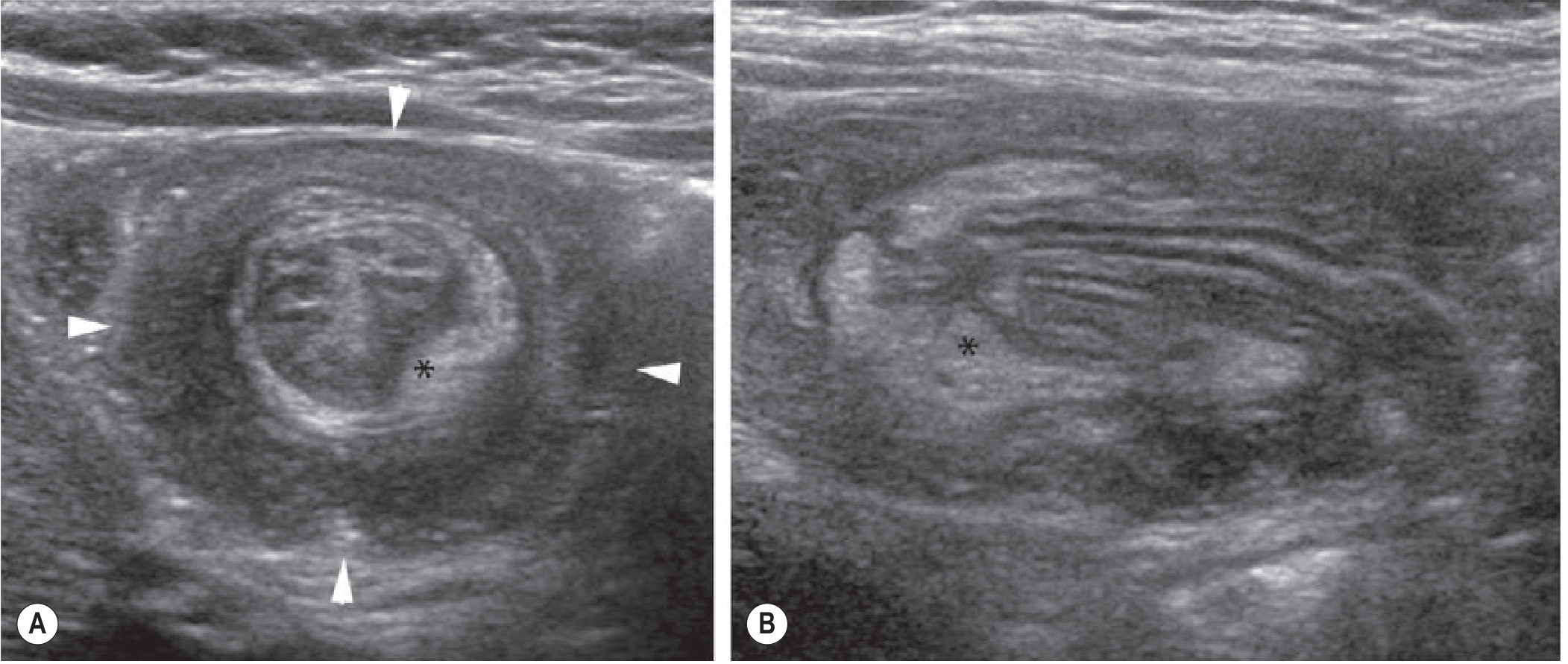
Fig: (A) Axial view - "doughnut/target sign" (arrowheads) with the pathognomonic hyperechoic semilunar appearance of mesenteric fat (asterisk). (B) Longitudinal view - "sandwich sign" showing multiple layers of bowel wall and mesenteric fat. (Grainger & Allison's Diagnostic Radiology)
| View | Sign |
|---|---|
| Transverse (axial) | "Target sign" / "Doughnut sign" |
| Longitudinal | "Sandwich sign" / "Pseudokidney sign" |
| Specific feature | "Crescent in doughnut" - hyperechoic semilunar mesenteric fat |
- US also evaluates for secondary lead points
- Free intraperitoneal fluid is common and alone does not indicate bowel necrosis
- Power Doppler is unreliable for assessing bowel necrosis
CT Scan
Shows the classic "target sign" on axial sections - layers of bowel wall creating a bullseye appearance:
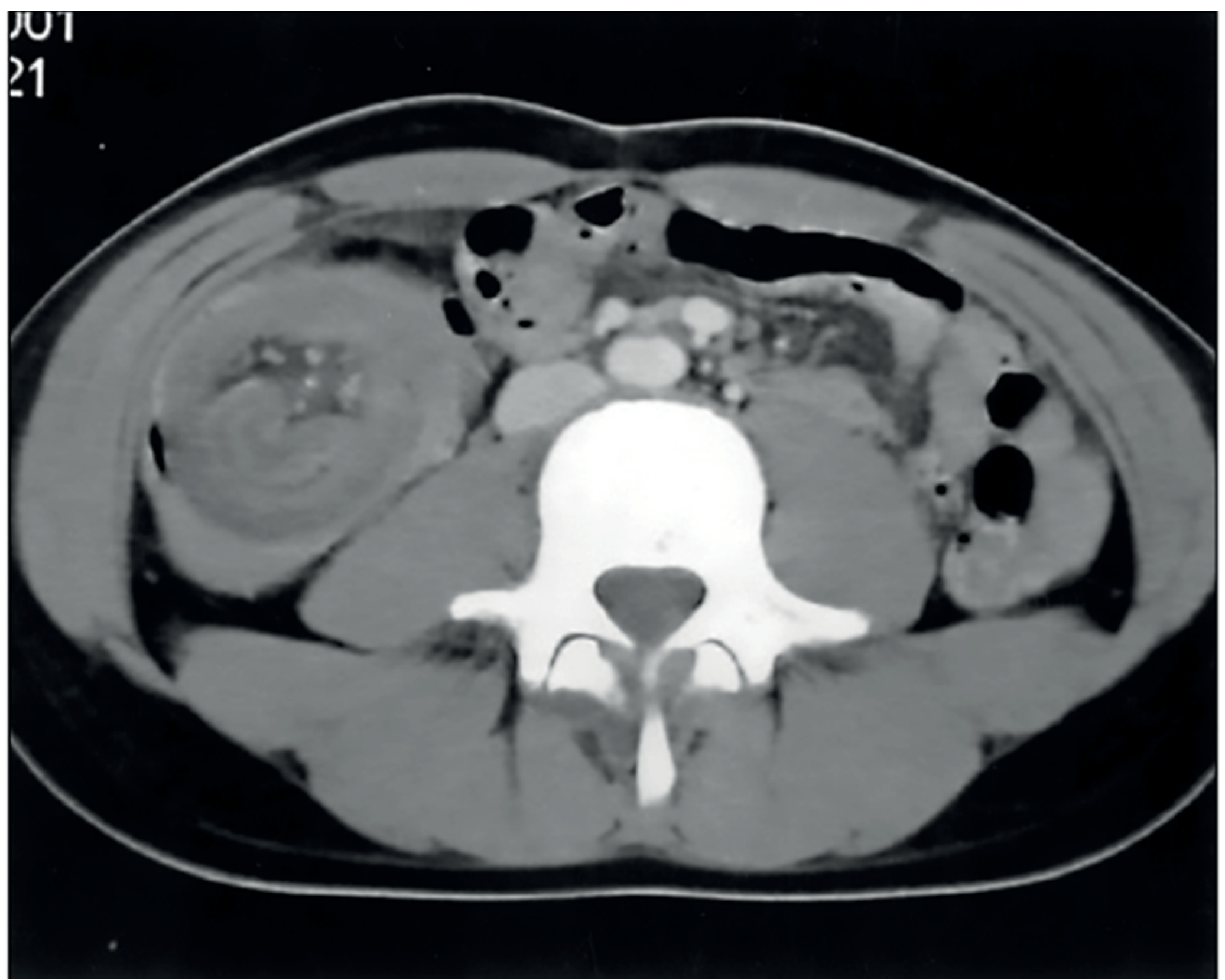
Fig: Axial CT showing the 'target sign' of ileocolic intussusception. (Bailey and Love's Surgery)
Plain Radiograph
- Role is controversial - should NOT be routinely used
- Features (when present): soft-tissue mass contrasting an air-filled bowel loop = "meniscus sign"; dilated proximal bowel loops; paucity of gas in the right iliac fossa
- ~50% of cases can be suspected on plain radiograph
- Free intraperitoneal gas on AXR = contraindication to enema reduction
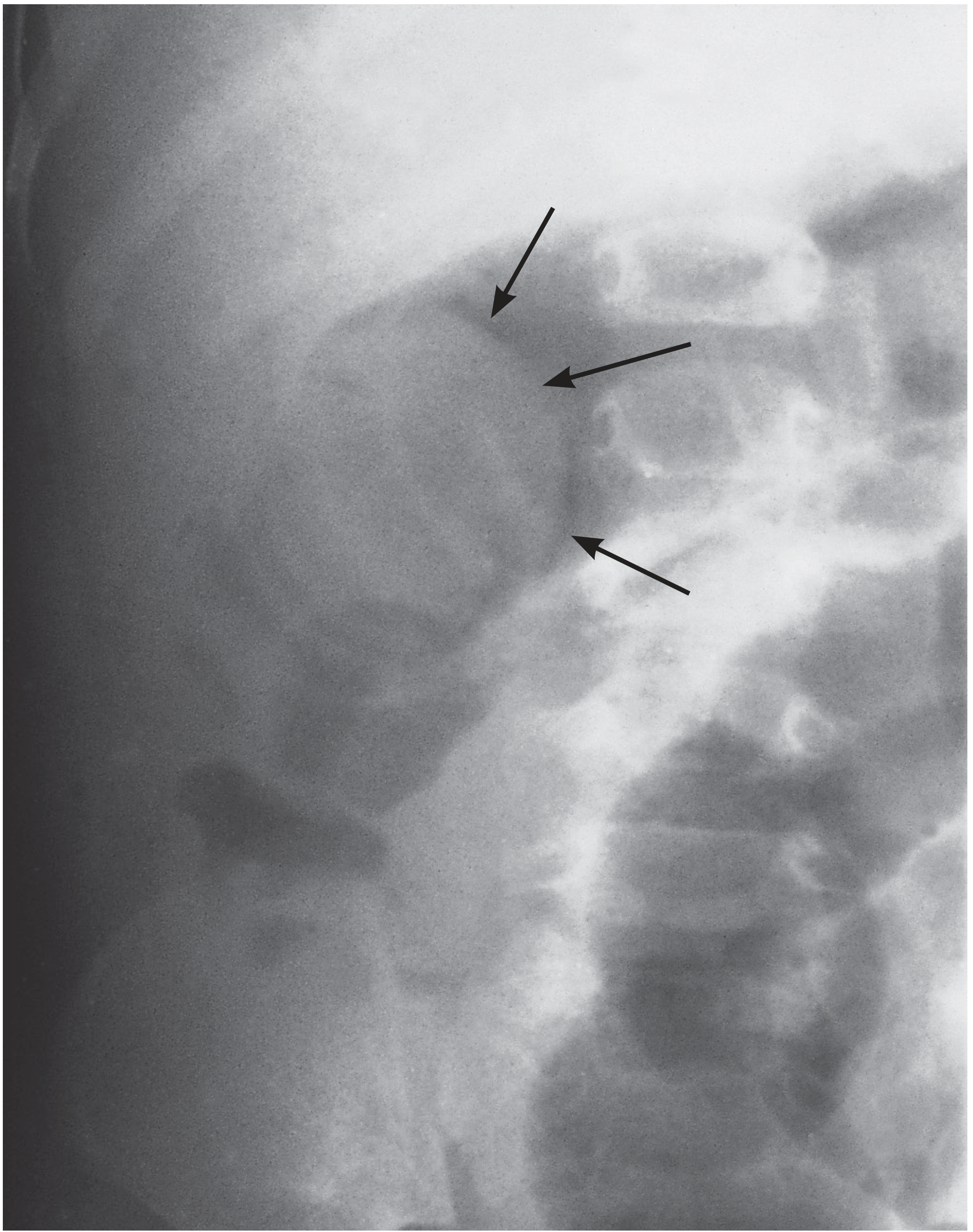
Fig: Air enema reduction - arrows mark the soft tissue shadow of the intussusceptum. (Bailey and Love's Surgery)
Management
Initial resuscitation (all patients)
- IV fluid resuscitation
- Broad-spectrum antibiotics
- Nasogastric drainage
Non-operative reduction (first-line in paediatric ileocolic intussusception)
Pneumatic (air) or hydrostatic (contrast) enema reduction
- Attempted after resuscitation in haemodynamically stable children
- >70% of cases are reducible non-operatively
- Success is confirmed when air flows into the small bowel and symptoms/signs resolve
- Repeat enema after a few hours is attempted in centres if initial attempt fails
Absolute contraindications to enema reduction:
- Free intraperitoneal air (perforation)
- Clinical peritonitis
- Haemodynamic instability/shock
No sonographic features alone (including lead point) should preclude a reduction attempt in a stable child.
Operative management
Indications:
- Peritonitis
- Bowel obstruction at initial presentation
- Failed enema reduction
- Multiple recurrences (third recurrence)
- Evidence of bowel necrosis or infarction
- Pathological lead point identified
Technique:
- Open or laparoscopic approach
- Retrograde "squeezing" of the intussusceptum proximally
- Assess bowel viability after reduction
- Bowel resection (ileocolectomy with primary anastomosis) if: irreducible, bowel non-viable, or lead point found
- Recurrence rates are extremely low after surgical reduction
Recurrence
- ~5-11% after non-operative reduction, usually within 24 hours
- Managed by repeat enema
- Third recurrence → surgical management
Adult Intussusception
- Uncommon; nearly always has a pathological lead point (polyp, malignancy, lymphoma, Meckel's diverticulum)
- Presentation may be subacute or chronic with intermittent obstruction
- Surgery is typically required
- Small-bowel intussusceptions may be managed conservatively in select cases; colonic intussusceptions generally require resection
Recent systematic review (2024) and 2025 systematic review confirm that adult intussusception is predominantly secondary (>80-90% have a lead point), and surgical resection - often without prior attempt at reduction - is the standard approach for colonic disease to avoid seeding of potentially malignant lead points.
Summary - Key Points
| Feature | Paediatric | Adult |
|---|---|---|
| Aetiology | Idiopathic (lymphoid hyperplasia) >90% | Pathological lead point (neoplasm, etc.) |
| Most common type | Ileocolic (77%) | Entero-enteric or colocolic |
| Lead point | Rare (5-12%); Meckel's diverticulum | Near universal |
| First-line treatment | Pneumatic/hydrostatic enema | Surgery |
| Surgery indication | Failed reduction, peritonitis, recurrence | Usually primary treatment |
| Recurrence after non-op | ~5-11% | N/A |
Sources: Bailey and Love's Short Practice of Surgery 28th ed.; Sabiston Textbook of Surgery; Grainger & Allison's Diagnostic Radiology; Rosen's Emergency Medicine; Sleisenger & Fordtran's GI & Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.