Carcinoma of prostate
Reading File
Finding Sources
Finding Sources
Searching PubMed
"prostate cancer"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the key information needed for a comprehensive answer. Let me compile it.
Carcinoma of the Prostate
Epidemiology
Adenocarcinoma of the prostate is the most common malignancy in men in the United States, accounting for approximately 21% of all male cancers. It is the second leading cause of cancer-related death in men, after lung cancer. It is overwhelmingly a disease of aging - the incidence rises from ~20% in men in their 50s to ~70% in men aged 70-80 years on autopsy studies. In the UK alone, over 48,000 men were diagnosed and 11,800 died from it in 2017. African American men die from prostate cancer at more than double the rate of European American men, partly due to unequal access to screening and treatment.
- Robbins & Kumar Basic Pathology, p. 660
Pathogenesis
Several factors converge in prostate carcinogenesis:
- Androgens - of central importance. Cancers depend on androgen receptor signaling for growth. Most tumors eventually become resistant to castration by acquiring androgen receptor gene amplifications or mutations enabling ligand-independent activation.
- Heredity - 10-15% of younger men with prostate cancer have a positive family history.
- Molecular mutations - The most common driver mutations are gene rearrangements creating TMPRSS2-ETS fusion genes (most often ERG or ETV1 overexpression) and mutations enhancing PI3K/AKT signaling, promoting tumor cell survival and growth.
- Environmental factors - Rates of clinically evident prostate cancer are low in Japan, China, and India despite similar rates of microscopic foci worldwide, pointing to environmental/dietary contributions.
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
Site of Origin
Approximately 70% of prostate carcinomas arise in the peripheral zone of the gland, often posteriorly where they may be palpable on digital rectal examination (DRE). Importantly, benign prostatic hyperplasia (BPH) arises in the transition zone - TURP for BPH therefore confers no protection against subsequent carcinoma.
Pathology / Morphology
The vast majority are adenocarcinomas (acinar type). On gross section, the neoplastic tissue is gritty and firm, and may be difficult to visualize macroscopically.
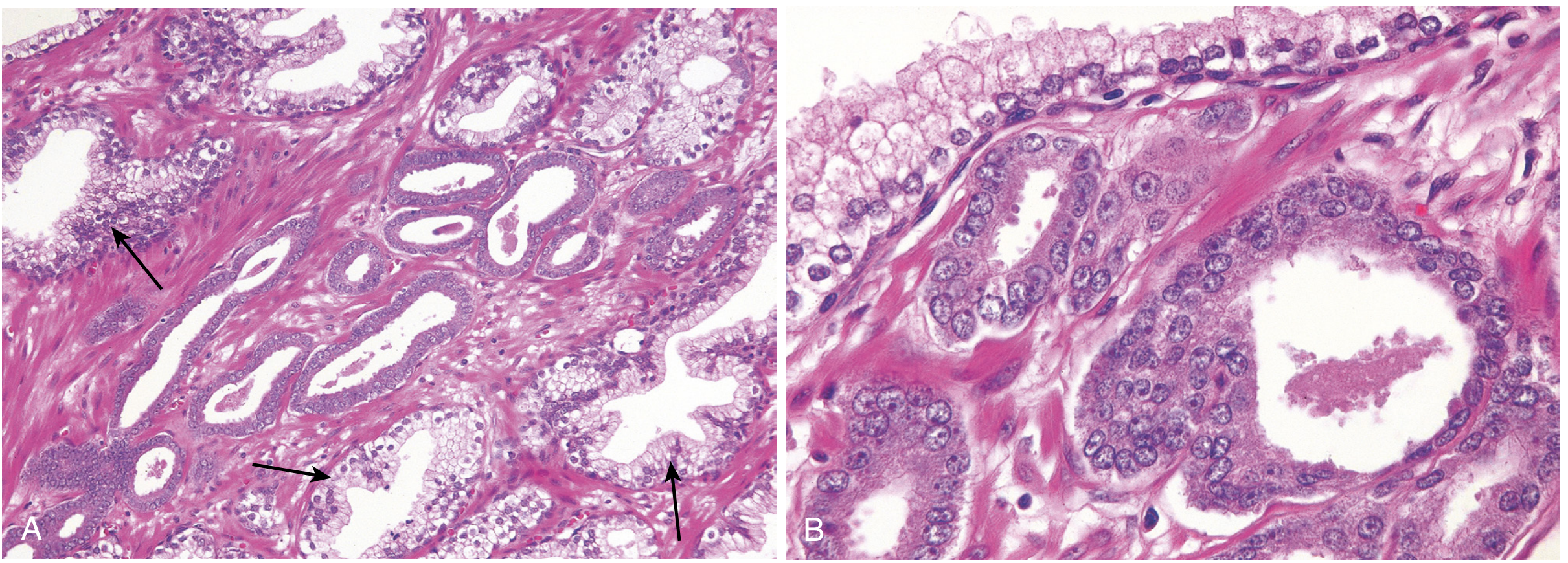
Histological features of malignant glands (vs. benign):
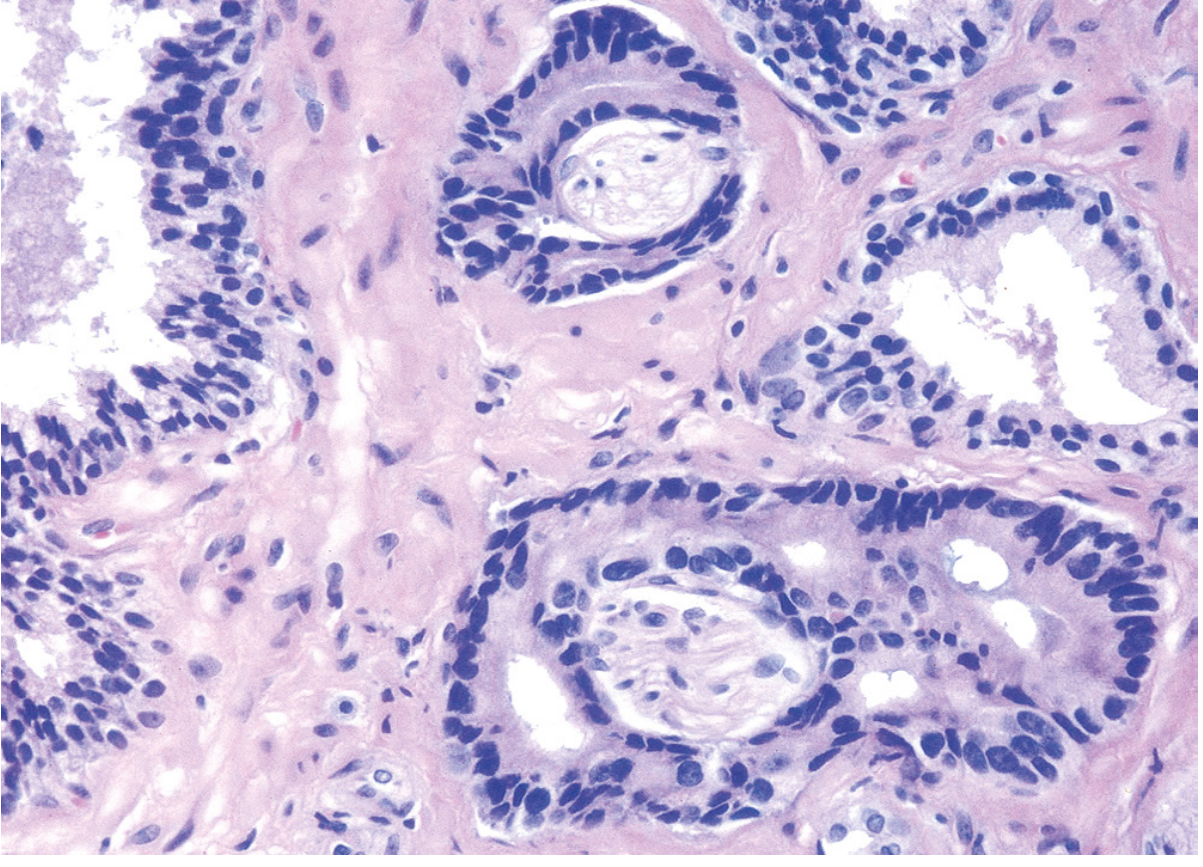
- Smaller glands lined by a single uniform layer of cuboidal or low columnar epithelium
- Absent basal cell layer (present in benign glands) - key distinguishing feature
- Tightly packed cells with no branching or papillary infoldings
- Enlarged nuclei with prominent nucleoli
- Amphophilic cytoplasm
- Perineural invasion is a specific finding for malignancy
Useful immunohistochemical markers:
- AMACR (alpha-methylacyl-CoA racemase) - upregulated in prostate cancer (sensitivity 82-100%)
- Basal cell markers (p63, CK5/6) - positive in benign glands, absent in cancer
High-grade prostatic intraepithelial neoplasia (HGPIN) is found in ~80% of prostatectomy specimens for carcinoma. It features architecturally benign acini lined by atypical cells with prominent nucleoli, but retains basal cells and an intact basement membrane.
Gleason Grading System
Gleason grading is the cornerstone of prostate cancer grading and correlates with both pathologic stage and prognosis.
- Five grades (1-5) based on degree of glandular differentiation and relation to stroma:
- Grade 1: Well-differentiated uniform round glands in well-circumscribed nodules
- Grade 5: Tumor cells infiltrating stroma in cords, sheets, and solid nests
- A primary grade is assigned to the dominant pattern and a secondary grade to the second most frequent pattern; these are summed to give the Gleason score (range 2-10)
- Grades 1 and 2 are no longer routinely reported (outcome similar to grade 3); Grade 3 cancers almost never metastasize
Gleason score interpretation:
| Gleason Score | Grade Group | Clinical Significance |
|---|---|---|
| 6 (3+3) | Grade Group 1 | Low risk; screen-detected |
| 3+4=7 | Grade Group 2 | Intermediate |
| 4+3=7 | Grade Group 3 | Intermediate-high |
| 8 (4+4) | Grade Group 4 | High risk |
| 9-10 | Grade Group 5 | Very high risk; advanced |
Most potentially treatable screen-detected cancers have Gleason scores of 6 or 7. Scores of 8-10 are typically advanced cancers less amenable to cure.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 908
Staging (pTNM - AJCC 8th Edition)
| Stage | Findings |
|---|---|
| pT2 | Organ confined |
| pT3a | Extraprostatic extension (unilateral or bilateral) or microscopic bladder neck invasion |
| pT3b | Seminal vesicle invasion |
| pT4 | Fixed or invades adjacent structures (rectum, bladder, levator muscles, pelvic wall, external sphincter) |
| N1 | Regional (obturator/paraaortic) lymph node metastasis |
| M1a | Distant lymph node metastases |
| M1b | Bone metastases |
| M1c | Other distant sites |
Clinical T-stage categories:
- T1a/T1b - found incidentally on TURP (<5% or >5% of tissue involved)
- T1c - found via PSA screening biopsy
- T2 - palpable, confined to prostate
- T3/T4 - locally advanced
Only T1 and T2 (early disease) are potentially curable. Symptomatic cancers are T3/T4 or metastatic and are not curable.
Local Spread and Metastasis
Local invasion most commonly involves:
- Periprostatic soft tissue
- Seminal vesicles
- Base of the urinary bladder (causing ureteral obstruction)
Lymphatic spread: obturator nodes → paraaortic nodes
Hematogenous spread (chiefly to bone - osteoblastic metastases):
- Lumbar spine (most common)
- Proximal femur
- Pelvis
- Thoracic spine
- Ribs
Osteoblastic bone metastases in a male strongly point to prostatic origin.

Clinical Features
Many patients are asymptomatic at diagnosis (screen-detected). When symptomatic, features include:
Local disease:
- Lower urinary tract symptoms (LUTS): frequency, nocturia, hesitancy, poor stream
- Haematuria or haematospermia (less common)
- Hard, irregular nodule on DRE
Advanced/metastatic disease:
- Bone pain (particularly low back pain, pelvic pain)
- Weight loss, anaemia
- Pathological fractures
- Ureteral obstruction and hydronephrosis
- Spinal cord compression (from vertebral metastases)
Diagnosis and Investigations
PSA (Prostate-Specific Antigen)
- Organ-specific (not cancer-specific) glycoprotein produced by prostatic epithelium
- Normal: <4 ng/mL (though age-adjusted norms are used)
- Elevated PSA may be seen in BPH, prostatitis, and prostate cancer
- PSA is controversial as a screening test (does not fulfil WHO screening criteria) but has clear value in monitoring treatment response and recurrence
- PSA >10 ng/mL warrants bone scan to assess for metastases
Digital Rectal Examination (DRE)
- Hard, irregular nodule in the peripheral zone suggests malignancy
- Measurement of PSA detects only 30-50% of cancers detected at autopsy (larger, more significant tumors)
Multiparametric MRI (mpMRI)
- Incorporates T2-weighted, diffusion-weighted, and dynamic contrast-enhanced imaging
- Reported using PI-RADS v2 scoring: score ≥3 indicates possible malignancy
- Used to localize and stage disease, and to guide targeted biopsy
Prostate Biopsy
- Transrectal ultrasound (TRUS)-guided biopsy is standard; transperineal approach increasingly preferred (lower sepsis risk)
- Antibiotic cover given to all
- Fusion biopsy (mpMRI + TRUS image fusion) allows targeting of suspicious index lesions for higher diagnostic yield
- Sampling: typically 10-12 systematic cores
Bone Scan
- Technetium-99m scintigraphy
- Indicated if PSA >10 ng/mL, Gleason ≥7, or locally advanced disease
- More sensitive than skeletal survey; false positives from arthritis, fractures
PSMA-PET Scan
- Gallium-labelled prostate-specific membrane antigen PET
- Sensitive for lymph node metastases and restaging after treatment relapse
- May detect disease not visible on conventional imaging
Treatment
Treatment is guided by three key parameters: PSA level, Gleason grade, and clinical stage, often combined in nomograms.
Early Disease (T1/T2) - Potentially Curative
| Risk Category | Management |
|---|---|
| Low-risk (low PSA, Gleason 6, small foci) | Active surveillance - DRE + PSA every 3-6 months, mpMRI yearly, repeat biopsy; radical treatment deferred until progression |
| Intermediate-risk | Radical prostatectomy OR radical radiotherapy (external beam or brachytherapy) in younger fitter patients; active surveillance still an option in elderly/lower-risk end |
| High-risk (T3) | Multimodal therapy: androgen ablation + radiotherapy ± radical prostatectomy with salvage radiotherapy |
Radical prostatectomy (open or robotic) - includes pelvic lymph node dissection; complications include impotence (up to 80%) and urinary incontinence.
Radiotherapy:
- External beam radiotherapy (EBRT) with or without androgen deprivation
- Brachytherapy (radioactive seed implantation) for low-intermediate risk
- Good local control, equivalent outcomes to surgery in many settings
Metastatic Disease
Androgen Deprivation Therapy (ADT) is the mainstay:
- Surgical castration (bilateral orchidectomy) - immediate, permanent
- Medical castration - LHRH (GnRH) agonists (e.g., leuprolide, goserelin): chronic administration desensitizes pituitary LHRH receptors → suppresses LH → reduces testosterone
- Anti-androgens (e.g., bicalutamide, enzalutamide) can be added
Most patients respond initially, but castration-resistant prostate cancer (CRPC) inevitably develops as tumors acquire androgen receptor amplifications or bypass androgen signaling.
Chemotherapy:
- Docetaxel - first-line for fit patients with symptomatic or high-volume metastatic disease
- Cabazitaxel - second-line after docetaxel failure
Newer agents for CRPC:
- Abiraterone (CYP17 inhibitor - blocks androgen synthesis)
- Enzalutamide (next-generation anti-androgen)
- PSMA-targeted radioligand therapy (Lu-177-PSMA)
Prognosis
| Stage | 5-year Survival |
|---|---|
| Localised (T1/T2) | ~99% |
| Regional (T3/N1) | ~85% |
| Distant metastases (M1) | ~31% |
The Gleason score remains the most powerful pathological predictor of outcome. Most men diagnosed with early prostate cancer die with the disease rather than because of it - reflecting the indolent biology of many tumors. This is the central challenge: distinguishing clinically significant from insignificant disease to avoid overtreatment.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.); Robbins & Kumar Basic Pathology; Bailey and Love's Short Practice of Surgery (28th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.