Pseudogout
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
pseudogout calcium pyrophosphate crystals polarized light microscopy chondrocalcinosis
Searching PubMed
calcium pyrophosphate deposition disease treatment
Loading Image
Loading Image
Pseudogout (Calcium Pyrophosphate Deposition Disease)
Definition & Pathophysiology
Pseudogout is the acute inflammatory arthritis caused by calcium pyrophosphate dihydrate (CPPD) crystals deposited in articular cartilage, menisci, and intervertebral discs. When deposits enlarge and rupture into the joint space, they trigger inflammasome activation in macrophages — the same mechanism as in gout — producing an acute synovitis. Inflammation is generally milder than gout.
The condition is divided into three etiological types:
| Type | Mechanism |
|---|---|
| Sporadic (idiopathic) | Aging chondrocytes produce excess extracellular inorganic pyrophosphate; most common |
| Hereditary | Autosomal dominant mutations in pyrophosphate transport channels → early-onset disease |
| Secondary (metabolic) | See associated conditions below |
Associated Metabolic Conditions
Early or atypical CPPD should prompt screening for:
- Hyperparathyroidism (↑ PTH → ↑ extracellular Ca²⁺)
- Hemochromatosis (iron deposition alters pyrophosphatase activity)
- Hypomagnesemia (Gitelman syndrome) — Mg²⁺ is a pyrophosphatase cofactor
- Hypophosphatasia (↓ alkaline phosphatase → ↑ inorganic pyrophosphate)
- Hypothyroidism, diabetes, prior joint trauma/surgery
Clinical Presentations
CPPD is frequently asymptomatic (lanthanic), recognized incidentally on imaging. When symptomatic, it presents in four patterns:
| Pattern | Description |
|---|---|
| Acute pseudogout | Acute mono- or oligoarthritis; ~60% of symptomatic cases |
| Pseudo-OA | Chronic polyarticular degeneration mimicking osteoarthritis; knees, wrists, MCPs |
| Pseudo-RA | Chronic inflammatory polyarthritis; can mimic rheumatoid arthritis |
| Asymptomatic CPPD | Chondrocalcinosis on imaging only |
Acute Attack Features
- Most common joint: knee (followed by wrist, elbow, shoulder, ankle)
- Warm, swollen, acutely tender joint — similar to gout
- Patients tend to be older than typical gout patients
- Onset is less abrupt than gout; attacks can persist weeks to months
- ~50% of pseudo-OA patients experience superimposed acute attacks
Diagnosis
Synovial Fluid Analysis (Definitive)
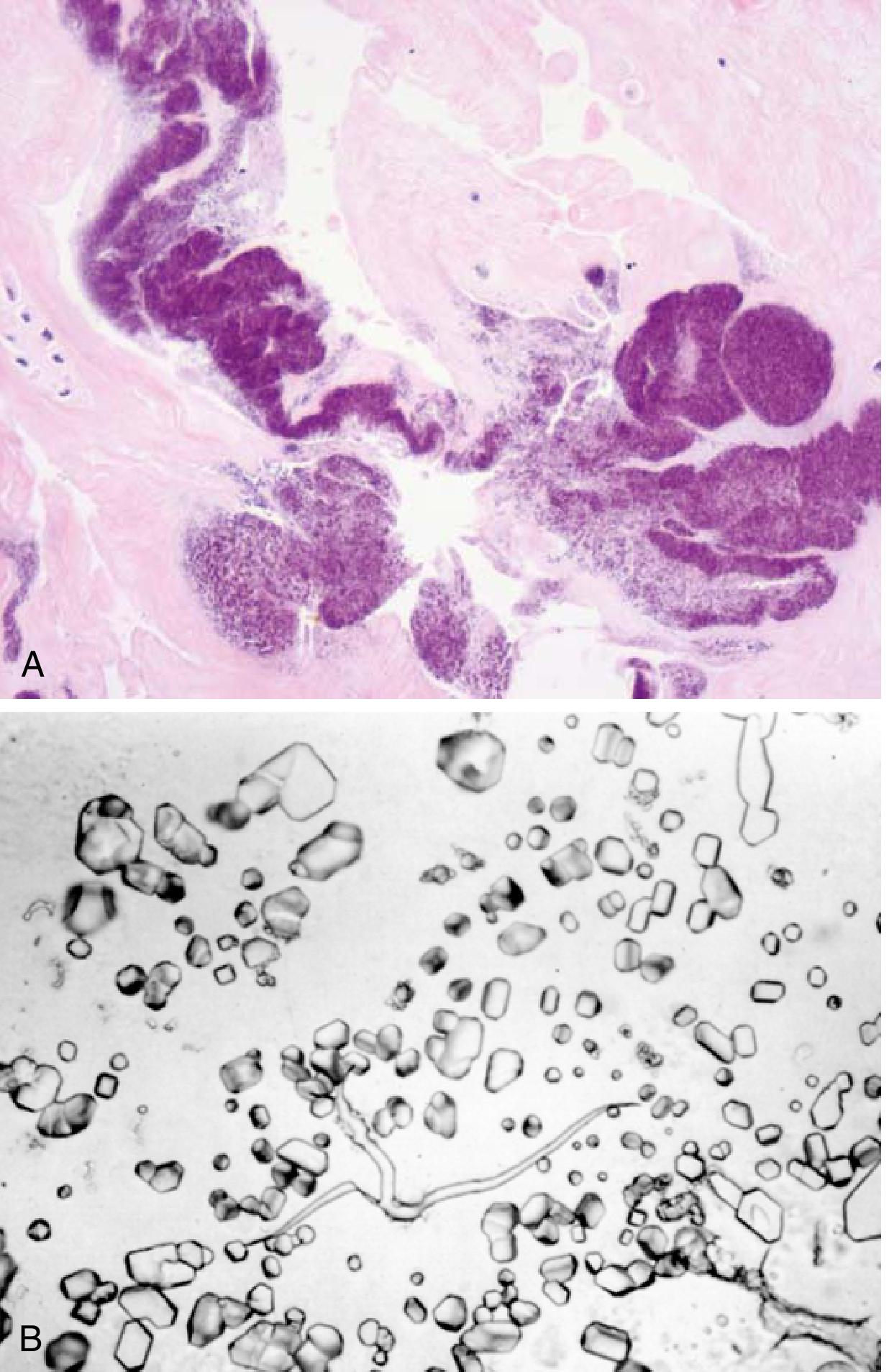
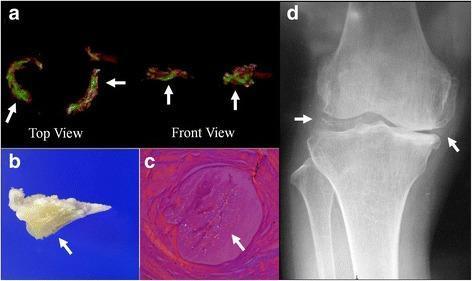
- Crystal morphology: rhomboid-shaped, 0.5–5 μm
- Birefringence: weakly positively birefringent under compensated polarized light (blue when parallel to slow axis — contrast with gout's needle-shaped, negatively birefringent urate crystals)
- Leukocyte count during acute attack: 15,000–30,000 cells/mm³, neutrophil predominance
- ⚠️ Crystals and concurrent infection can coexist — always consider septic arthritis
Imaging
- Chondrocalcinosis on plain radiograph: linear calcifications in articular cartilage — supportive but not diagnostic; absent in >50% of cases
- Best views: wrists, knees, pubic symphysis
- Hook-like osteophytes at MCPs (unlike the erosions of RA)
- DECT can identify CPPD deposits (distinct from urate on dual-energy CT)
Metabolic Workup (especially in young patients or severe disease)
Serum: calcium, phosphorus, PTH, iron/TIBC/ferritin, alkaline phosphatase, magnesium
Crystal Comparison: Pseudogout vs. Gout
| Feature | Pseudogout (CPPD) | Gout (MSU) |
|---|---|---|
| Crystal | Calcium pyrophosphate | Monosodium urate |
| Shape | Rhomboid | Needle-shaped |
| Birefringence | Weakly positive (blue ∥ slow axis) | Strongly negative (yellow ∥ slow axis) |
| Typical joint | Knee, wrist | 1st MTP, ankle |
| Chondrocalcinosis on X-ray | Present | Absent |
| Serum uric acid | Normal | Elevated |
| Onset pattern | Less abrupt, longer attacks | Abrupt, nocturnal |
Treatment
Acute Attack
There are no agents that prevent or reverse crystal formation; therapy targets inflammation:
- NSAIDs — first-line for most patients (short high-dose course); may be contraindicated in elderly or those with renal/GI comorbidities
- Colchicine — effective via inhibition of PMN activity; narrow therapeutic window limits use in elderly
- Corticosteroids — intra-articular injection (rapid relief after ruling out infection) or systemic oral course
- Joint aspiration — both diagnostic and provides symptomatic relief
Chronic/Prophylactic
- Low-dose colchicine 0.6 mg twice daily for prevention of recurrent attacks
- NSAIDs for chronic pseudo-OA
- Methotrexate, IL-1 inhibitors, anti-TNF-α — show promise in small studies for refractory or periarticular disease
- Treat underlying metabolic disease (e.g., hyperparathyroidism, hypomagnesemia) — may improve arthritis in those subtypes, though benefit on crystal burden in hemochromatosis is uncertain
Key Points
- CPPD is primarily a disease of the elderly; consider underlying metabolic disease in young patients
- Definitive diagnosis requires synovial fluid crystal identification under polarized light
- Chondrocalcinosis on X-ray is supportive but neither sensitive nor specific
- ~50% of affected individuals develop significant joint damage over time
- No disease-modifying therapy exists; treatment is entirely symptomatic
Sources: Robbins & Kumar Basic Pathology 10e; Goldman-Cecil Medicine; Washington Manual of Medical Therapeutics; Rosen's Emergency Medicine; Miller's Review of Orthopaedics 9e
Septic arthritis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"septic arthritis" diagnosis management
Reading File
Reading File
Searching Images
septic arthritis joint aspiration synovial fluid diagnosis
Loading Image
Loading Image
Septic Arthritis
Definition & Overview
Septic arthritis is invasion of a joint by an infectious agent — bacterial arthritis being the most common subset — resulting in organism proliferation and acute inflammation. It is an orthopedic emergency: even with prompt treatment, it leads to permanent loss of function in 25–50% of patients. Incidence in native joints is ~2–10/100,000; in patients with rheumatoid arthritis this rises to 30–70/100,000.
Pathogenesis & Routes of Infection
| Route | Notes |
|---|---|
| Hematogenous spread (~75%) | Most common; bacteremia seeds the highly vascular synovium |
| Direct inoculation | Trauma, bites, arthrocentesis (rare: <1/10,000), arthroscopy |
| Contiguous spread | Extension from adjacent osteomyelitis (especially knee, hip, shoulder — where synovium attaches to metaphysis) |
| Iatrogenic | Post-joint injection or surgery |
Bacteria trigger synovial hyperplasia, inflammatory cell infiltration, and release of proteases and cytokines that destroy cartilage and bone. Bacterial toxins and superantigens (e.g., staphylococcal toxic shock) compound this damage.
Microbiology
S. aureus is the single most common organism overall. Pathogen varies by clinical context:
| Patient Group | Likely Organisms |
|---|---|
| Healthy adults, sexually active | S. aureus, N. gonorrhoeae, Streptococci |
| Elderly / comorbid (RA, DM, cancer) | S. aureus, gram-negative bacilli |
| Injection drug users | S. aureus, gram-negatives; sternoclavicular involvement suggests IVDU |
| Children | S. aureus, Group A Strep; neonates add gram-negatives |
| Sickle cell disease | Salmonella (increasingly also S. aureus) |
| Immunocompromised / HIV | MRSA, gram-negatives, fungi, mycobacteria |
| Prosthetic joint | Coagulase-negative staphylococci, S. aureus |
Risk Factors
Penetrating trauma, RA, OA, DM, alcohol use disorder, injection drug use, cutaneous ulcers, indwelling IV catheters, cancer, immunosuppressive/biologic therapies, advanced age, low socioeconomic status.
Clinical Features
- Onset: Acute (faster than osteomyelitis); the joint becomes exquisitely painful over hours
- Monoarticular in >80% of cases
- Most common joint: Knee (>50%), hip (25%), shoulder (15%) in adults; lower extremity predominates in all age groups
- Fever in >80% of children, ~40% of adults; immunosuppressed patients may be afebrile
- Signs: Swelling, erythema, warmth, exquisite tenderness; joint held in flexion (position of comfort); pain markedly worsened with passive range of motion
- Children: May present with pseudoparalysis or refusal to bear weight
- Polyarticular (<10–20%): seen in RA, SLE, immunocompromised patients — these patients may appear deceptively well but can decompensate rapidly
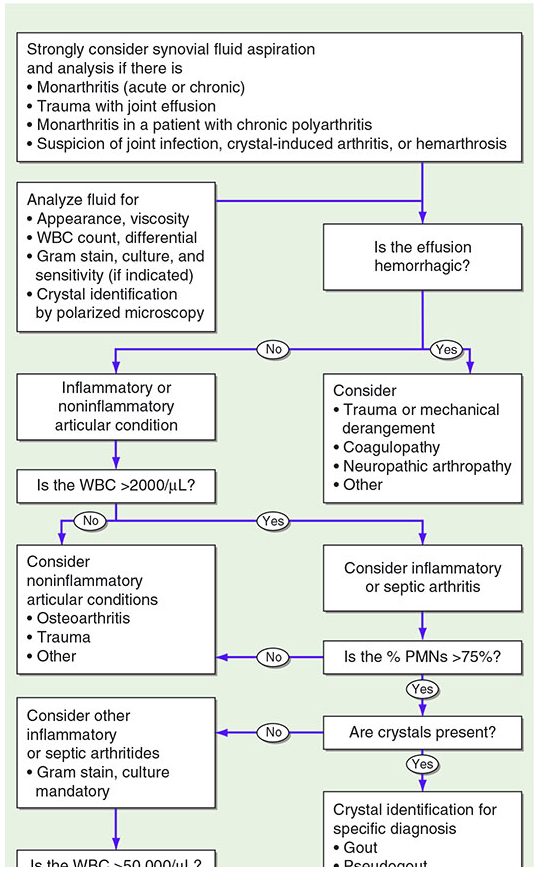
Synovial Fluid Analysis — Cornerstone of Diagnosis
Arthrocentesis is mandatory whenever septic arthritis is suspected. Anticoagulation is generally NOT a contraindication given the emergent nature.
| Parameter | Septic | Inflammatory (gout, RA) | Non-inflammatory (OA) | Normal |
|---|---|---|---|---|
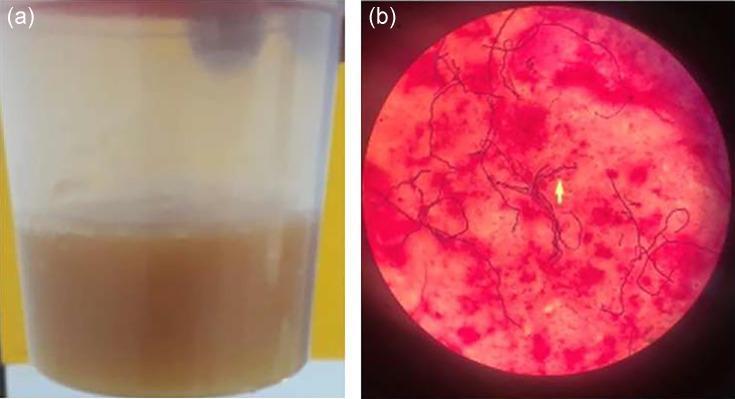
| Appearance | Turbid, purulent | Turbid/cloudy | Clear/yellow | Clear |
| WBC count | >50,000/mm³ (often much higher) | 2,000–50,000 | <2,000 | <200 |
| % PMNs | >75–90% | >50% | <25% | <25% |
| Gram stain | Positive <50% | Negative | Negative | Negative |
| Culture | Positive (gold standard) | Negative | Negative | — |
| Crystals | Absent (but coexistence possible) | Present (gout/CPPD) | Absent | — |
Key caveat: A WBC <50,000/mm³ does not exclude septic arthritis, especially in immunocompromised patients. Conversely, the presence of crystals does not exclude concurrent infection — if WBC >50,000, treat both.
Diagnostic Workup
Laboratory
- Blood cultures × 2 — positive in up to 50%; obtain before starting antibiotics
- Serum WBC: leukocytosis in only ~50% of cases — insensitive
- ESR: elevated in ~90%; CRP: useful to track resolution
- Procalcitonin: shows promise but needs further validation
- In young patients/IVDU: urethra/cervix/pharynx/rectal cultures for gonococcal disease
- Metabolic workup if unusual organism suspected: iron studies, complement levels
Imaging
- Plain radiography: usually normal early; provides baseline; may show joint space widening or erosion
- Ultrasound: confirms effusion; guides arthrocentesis of deep joints (hip, sacroiliac)
- MRI with contrast: preferred modality for diagnostic uncertainty and assessment of concurrent osteomyelitis, soft tissue involvement, fibrocartilaginous joints
- CT: useful for sacroiliac or sternoclavicular joints
- Bone scintigraphy: detects infection earlier than other modalities (increased symmetric uptake)
Differential Diagnosis
| Condition | Key distinguishing features |
|---|---|
| Gout/Pseudogout | Crystals on synovial fluid; WBC typically <50,000; may coexist with infection |
| Reactive arthritis | Migratory polyarthritis; less effusion; WBC usually <50,000; follows GI/GU infection |
| Transient (toxic) synovitis | Children 3 months–6 years; hip; afebrile; normal WBC/ESR; self-limited |
| Osteomyelitis | May produce adjacent joint effusion; both can coexist |
| Juvenile idiopathic arthritis | More gradual onset; often polyarticular |
| Lyme arthritis | Endemic area; less debilitated; check serology |
| RA/Psoriatic arthritis | Chronic course; septic arthritis can supervene — the sudden worsening of one joint in well-controlled polyarthritis warrants aspiration |
| Rheumatic fever | Migratory polyarthritis; may mimic gonococcal bacteremia |
Treatment
1. Antibiotics — Empirical (Start ASAP After Cultures)
Gram stain guides initial selection; modify when sensitivities return. Duration: 2–6 weeks (typically 4 weeks for S. aureus).
| Gram Stain Result / Clinical Scenario | Empirical Regimen |
|---|---|
| Gram-positive cocci | Vancomycin 15 mg/kg IV (covers MRSA) |
| Gram-negative bacilli | Ceftazidime, cefepime, imipenem, meropenem, or pip-tazo |
| No organisms on Gram stain (healthy adult) | Vancomycin alone |
| No organisms + immunocompromised/IVDU | Vancomycin + anti-pseudomonal agent (cefepime 2g IV or imipenem) |
| N. gonorrhoeae suspected | Ceftriaxone 1g IV q24h; also treat for chlamydia (doxycycline 100mg BID × 7 days) |
| Sickle cell | Vancomycin + ciprofloxacin (Salmonella coverage) |
| MSSA confirmed | Switch to nafcillin/oxacillin or cefazolin |
Targeted Therapy (Goldman-Cecil Table)
| Organism | First Choice | Alternative |
|---|---|---|
| MSSA | Nafcillin/oxacillin 1.5–2g IV q4–6h or cefazolin | Vancomycin or daptomycin |
| MRSA | Vancomycin or daptomycin 6–10 mg/kg q24h | Linezolid; dalbavancin |
| Penicillin-sensitive Strep | Penicillin G or ceftriaxone | Vancomycin |
| Enterobacteriaceae / Salmonella | Ceftriaxone | Ciprofloxacin |
| P. aeruginosa | Cefepime 2g IV q8–12h | Ceftazidime, imipenem, ciprofloxacin |
2. Joint Drainage
- Serial needle aspiration: standard initial approach for most joints; performed daily until clinical improvement
- Arthroscopic irrigation and debridement: preferred for hip (deep joint, difficult needle access); post-ACL reconstruction septic arthritis; failure to respond to needle aspiration
- Open surgical drainage: reserved for life-threatening complications (necrotizing fasciitis), failed arthroscopic management, or anatomically inaccessible joints
- Gonococcal arthritis rarely requires surgery
3. Adjunctive Measures
- Immobilization initially, then early mobilization to prevent contractures
- Dexamethasone (short course) in children may speed symptom resolution
- Treat underlying source (cellulitis, UTI, pneumonia, endocarditis)
Gonococcal Arthritis — Special Considerations
- Most common cause of infectious arthritis in sexually active adults <40 years
- Two presentations:
- Purulent monoarthritis (large or distal joints, elbows/knees)
- Triad: tenosynovitis + dermatitis (pustular/vesicular skin lesions) + polyarthralgias — associated with bacteremia
- Synovial fluid cultures often negative (positive in only 25–50%); culture pharynx, cervix/urethra, rectum, and blood — PCR of all sites increases yield
- Screen for coexisting STIs (syphilis, HIV, chlamydia, hepatitis B/C)
- Treatment: Ceftriaxone 1g IM/IV q24h until improvement, then oral step-down; consult current CDC guidelines for emerging resistance
- Prognosis: Good — rarely causes joint destruction compared to nongonococcal septic arthritis
Prognosis
- Loss of function occurs in 25–50% of patients even with adequate treatment
- Worse outcomes with: delayed diagnosis, MRSA, prosthetic joints, RA, immunosuppression
- Bacteremia from septic arthritis carries risk of seeding other sites — assess for endocarditis if S. aureus bacteremia is confirmed
Sources: Rosen's Emergency Medicine; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.