Uterus in Obg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Here is a comprehensive overview of the uterus in Obstetrics & Gynecology, drawn from Berek & Novak's Gynecology, Sabiston Textbook of Surgery, Creasy & Resnik's Maternal-Fetal Medicine, and Junqueira's Basic Histology.
The Uterus - Obstetrics & Gynecology
Anatomy
The uterus is a fibromuscular, intraperitoneal organ that sits posterior to the bladder and anterior to the rectum. The non-pregnant uterus typically weighs 40-80 g.
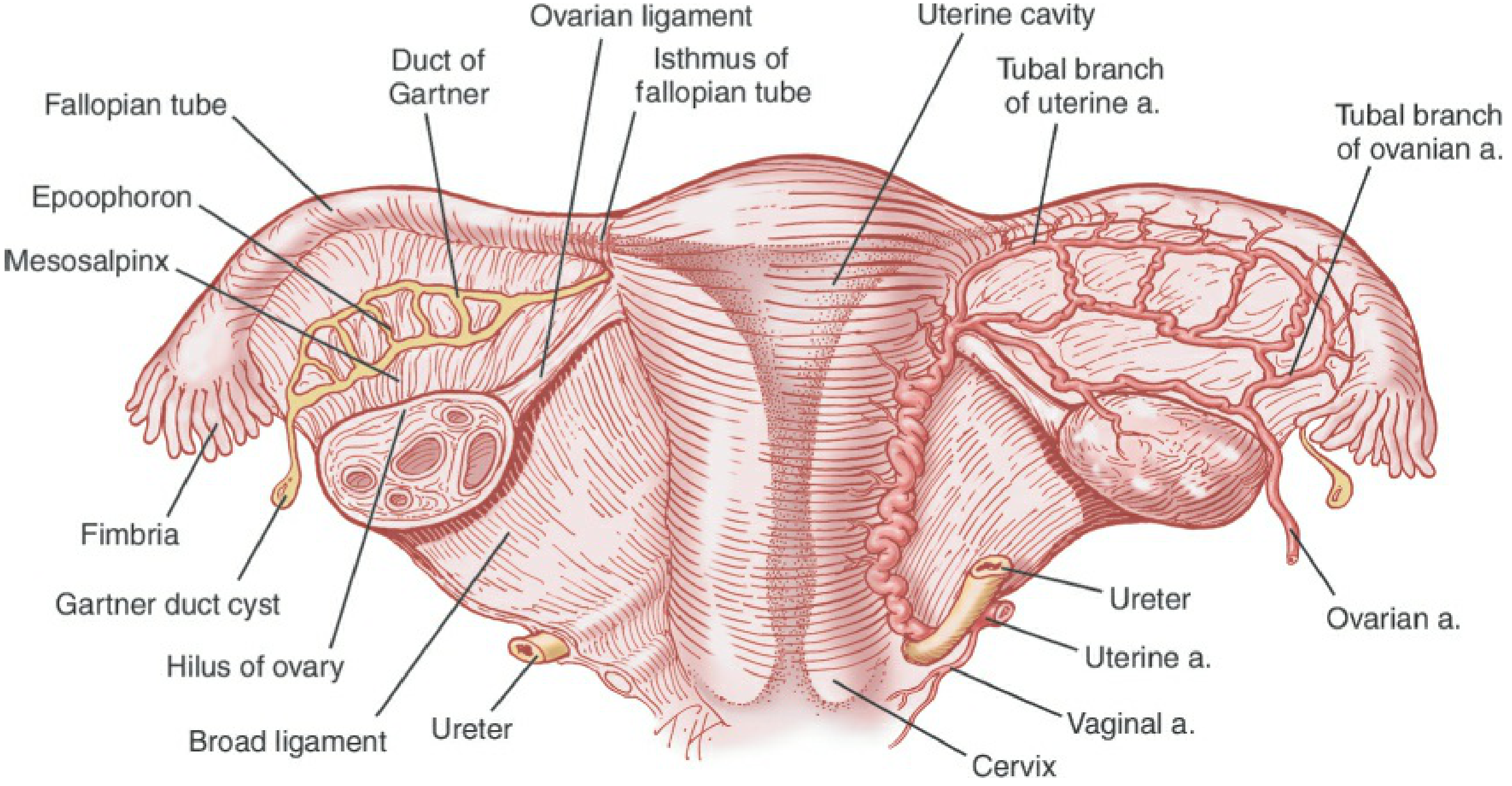
Regions of the Uterus
| Region | Description |
|---|---|
| Fundus | Curved superior area above the entry of the fallopian tubes |
| Corpus (Body) | Main muscular body; 2-3x larger than the cervix in adults |
| Cornu | Funnel-shaped upper lateral areas where the fallopian tubes insert |
| Isthmus (Lower Uterine Segment) | Area where the endocervical canal opens into the endometrial cavity; thins significantly during pregnancy |
| Cervix | Lower cylindrical structure with internal os (opens to isthmus) and external os (opens to vagina) |
- Uterine cavity is triangular in shape, lined by columnar gland-forming endometrium
- Endocervical canal is approximately 2-3 cm long
Layers of the Uterine Wall
The uterine wall has three distinct layers:
1. Perimetrium (Serosa)
Outer connective tissue layer, continuous with the broad ligaments; covered by mesothelium (peritoneum) over most of the corpus and posterior cervix.
2. Myometrium
- Thick middle layer of smooth muscle fibers, 1.5-2.5 cm thick
- Three interwoven layers of smooth muscle - inner and outer fibers run parallel to the long axis, middle layer is circular
- Some outer fibers are continuous with the round ligament and fallopian tubes
- During pregnancy: undergoes hyperplasia early, then hypertrophy driven by estrogen and mechanical distension; grows from ~70 g to ~1100 g at term
- After delivery: smooth muscle cells shrink and many undergo apoptosis
3. Endometrium
- Inner mucosal layer; simple columnar epithelium (ciliated + secretory cells)
- Contains tubular uterine glands that penetrate the full thickness
- Two concentric zones:
- Basal layer: adjacent to myometrium; not shed during menstruation; contains basal ends of glands and straight arteries; regenerates the functional layer
- Functional layer: superficial; shed during each menstrual cycle; contains the bulk of glands, spiral arteries, and surface epithelium
Blood Supply to the Endometrium
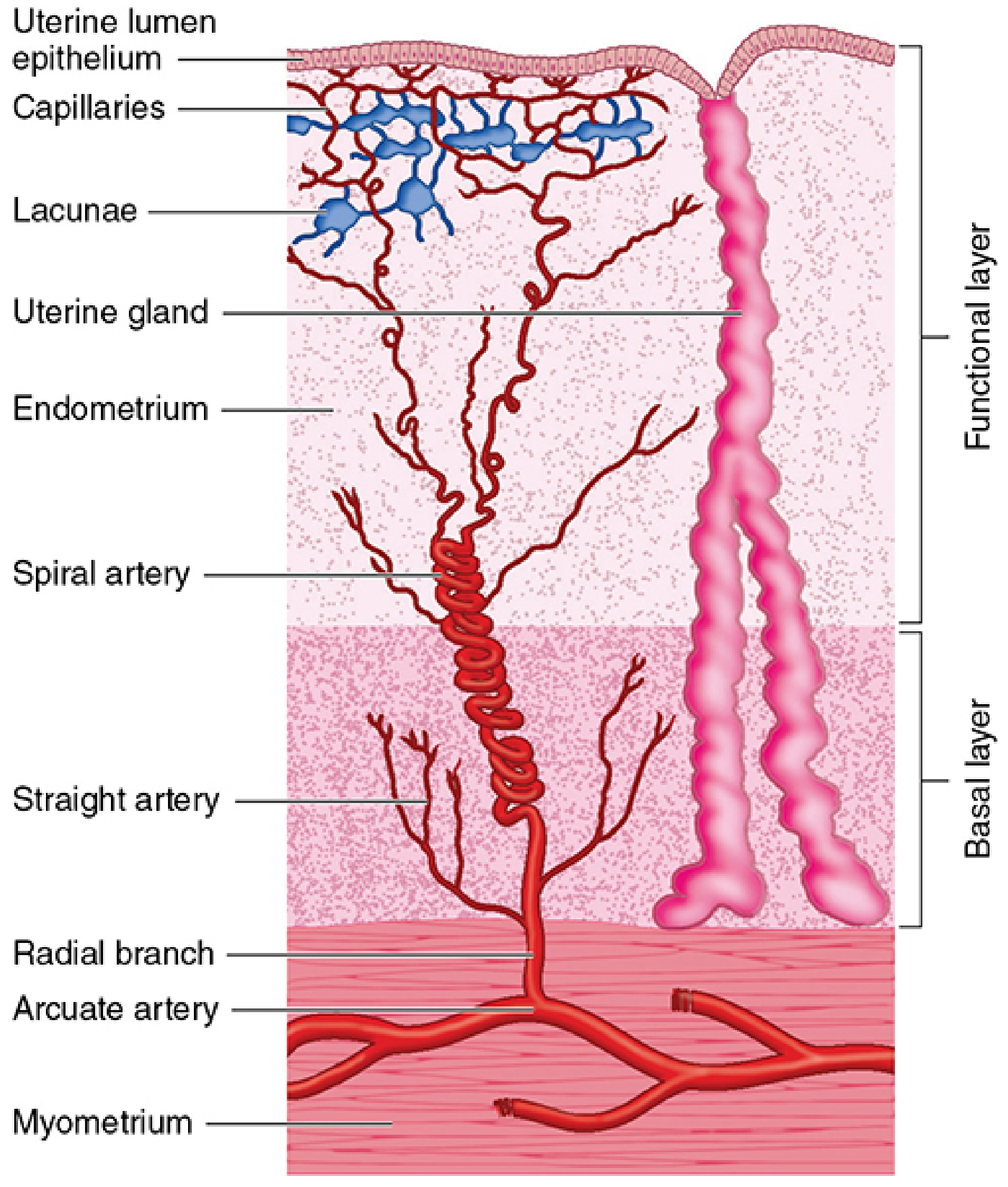
- Arcuate arteries (in myometrium) → radial arteries → two terminal branches:
- Straight arteries: supply only the basal layer; NOT sensitive to progesterone
- Spiral arteries: supply the functional layer; uniquely sensitive to progesterone; coil and elongate during the secretory phase; vasoconstrict at menstruation causing ischemia and shedding of the functional layer
- Uterine arteries branch from the internal iliac arteries; anastomose with the ovarian and vaginal arteries
- In pregnancy: uterine blood flow increases 10-fold (from 2% to 17% of cardiac output at term); 80-90% of uterine blood flow goes to the placenta
Ligamentous Support
The uterus is held in position by several structures:
| Ligament | Attachment | Function |
|---|---|---|
| Round ligament | Uterine cornu → inguinal ring → labia majora | Maintains anteversion; does NOT provide significant pelvic organ support |
| Broad ligament | Lateral surface of uterus → lateral pelvic sidewall | Double layer of peritoneum; carries neurovascular supply; does not provide major support |
| Cardinal ligament (Mackenrodt's) | Lateral pelvic diaphragm → fuses medially with vagina | Primary support of uterus at the level of the cervix; uterine arteries travel within it |
| Uterosacral ligament | Upper posterior cervix → 3rd sacral vertebra | Supports cervix and upper vagina; frames the rectum posteriorly; interdigitates with cardinal ligament fibers |
| Vesicouterine pouch | Anteriorly separates uterus from bladder | |
| Rectouterine pouch (Pouch of Douglas) | Posteriorly separates uterus from rectum | Deepest point of peritoneal cavity |
Important surgical note: The ureter crosses under the uterine artery within the cardinal ligament, approximately 2-3 cm lateral to the cervix - the classic "water under the bridge" relationship. This is the most common site of iatrogenic ureteral injury during gynecologic surgery.
Innervation
- Sympathetic: via hypogastric and ovarian plexus
- Parasympathetic: lumbosacral plexus (S2-S4)
- Afferent (pain) fibers: travel with sympathetic fibers in the lumbosacral plexus (T11-T12)
- The uterovaginal plexus is the primary nerve supply to the uterus
Cervix
- Exocervix (portio vaginalis): covered by stratified squamous epithelium
- Endocervical canal: covered by mucus-secreting columnar epithelium
- Squamocolumnar junction (SCJ): the transformation zone where the two epithelia meet - most vulnerable area for development of squamous neoplasia (CIN/cervical cancer)
- Eversion/ectopy: columnar epithelium extending onto the exocervix; normal in childhood, pregnancy, and with OCP use
- After menopause: transformation zone recedes into the endocervical canal
- Cervical mucus: clear and thin around ovulation (estrogen effect); scant and thick in post-ovulatory phase (progesterone effect)
- Cervix is primarily fibrous connective tissue (collagen I, collagen III, elastin, glycosaminoglycans) with only a small amount of smooth muscle
Menstrual/Uterine Cycle
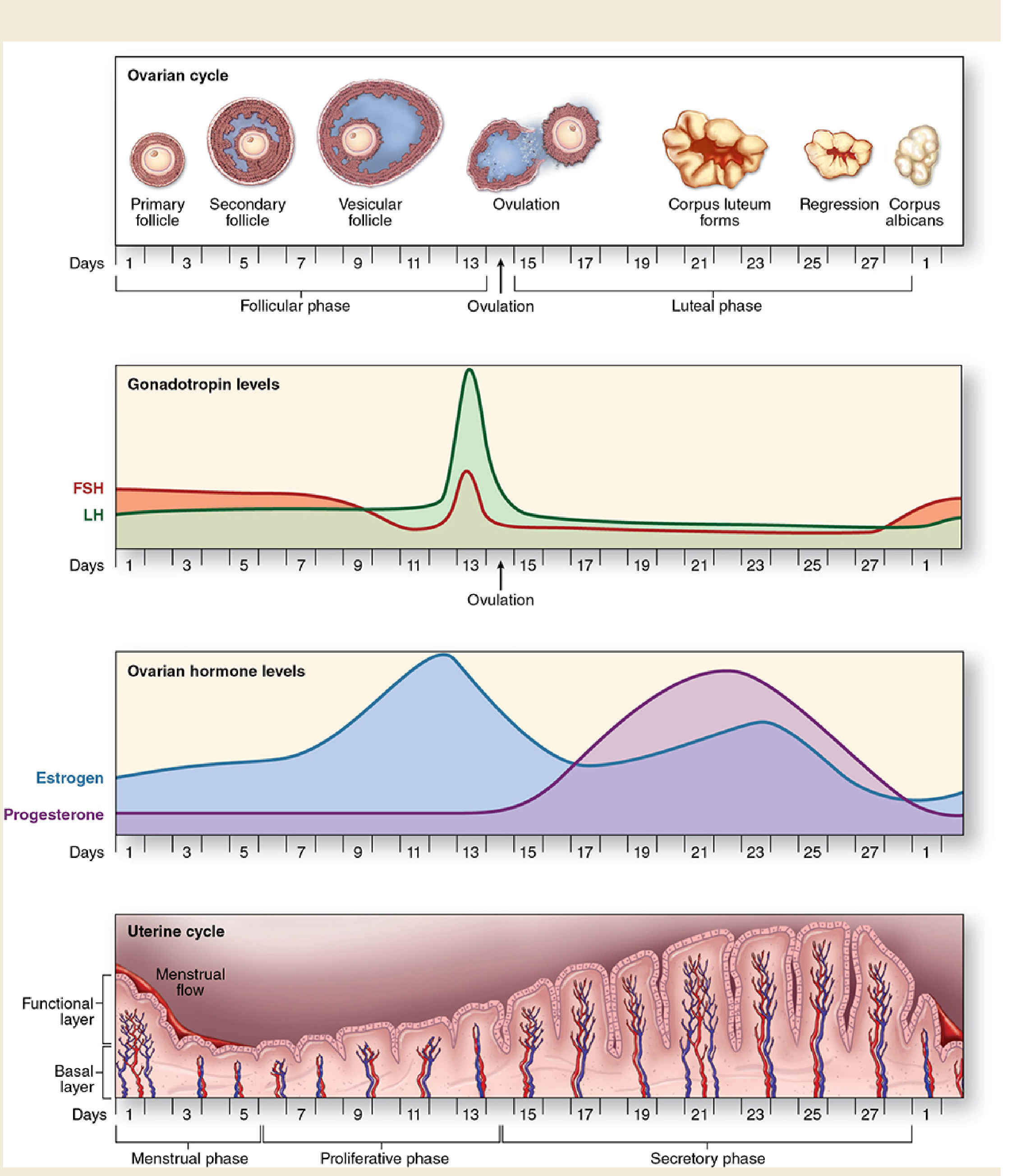
| Phase | Days | Hormone | Uterine Changes |
|---|---|---|---|
| Menstrual | 1-5 | Progesterone/estrogen fall | Spiral artery vasoconstriction → ischemia → shedding of functional layer |
| Proliferative | 5-14 | Estrogen (rising) | Endometrium regenerates; glands elongate; straight proliferating glands |
| Secretory | 15-28 | Progesterone + Estrogen (post-ovulation) | Glands become tortuous and secretory; spiral arteries coil; stroma becomes edematous and decidual |
Uterine Changes in Pregnancy
- Weight increases from 70 g to 1100-1200 g at term
- Volume increases from 10 mL to 5 L
- Myometrial smooth muscle transitions from quiescent to contractile state at term
- Lower uterine segment: the isthmus does NOT undergo hypertrophy; thins progressively as pregnancy advances - important in caesarean surgery
- Cervical remodeling occurs in 4 phases: softening → ripening → dilation → postpartum repair
Positions of the Uterus
- Version: angle of the uterus relative to the vagina
- Anteversion (normal) vs. Retroversion
- Flexion: angle between the uterine corpus and the cervical long axis
- Anteflexion (normal) vs. Retroflexion
- Abnormal positioning may result from endometriosis, adhesions, or fibroids
Sources: Berek & Novak's Gynecology, p. 178-179, 207; Sabiston Textbook of Surgery, p. 2785; Creasy & Resnik's Maternal-Fetal Medicine, Ch. 6; Junqueira's Basic Histology, p. 1129-1136
This is a shared conversation. Sign in to Orris to start your own chat.