Explain me about relationship of PTH on bone
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
PTH and Bone: A Complete Overview
1. PTH - Quick Background
Parathyroid hormone (PTH) is an 84-amino acid peptide secreted by the parathyroid glands. Its primary role is to maintain serum calcium within a narrow range. Bone is one of its three main target organs (along with kidney and intestine). The receptor for PTH on bone cells is PTH1R (PTH/PTHrP receptor type 1), found on osteoblasts and osteocytes - but notably not on osteoclasts.
2. Effects of PTH on Blood Calcium and Phosphate
When PTH is infused, blood calcium rises while blood phosphate falls:
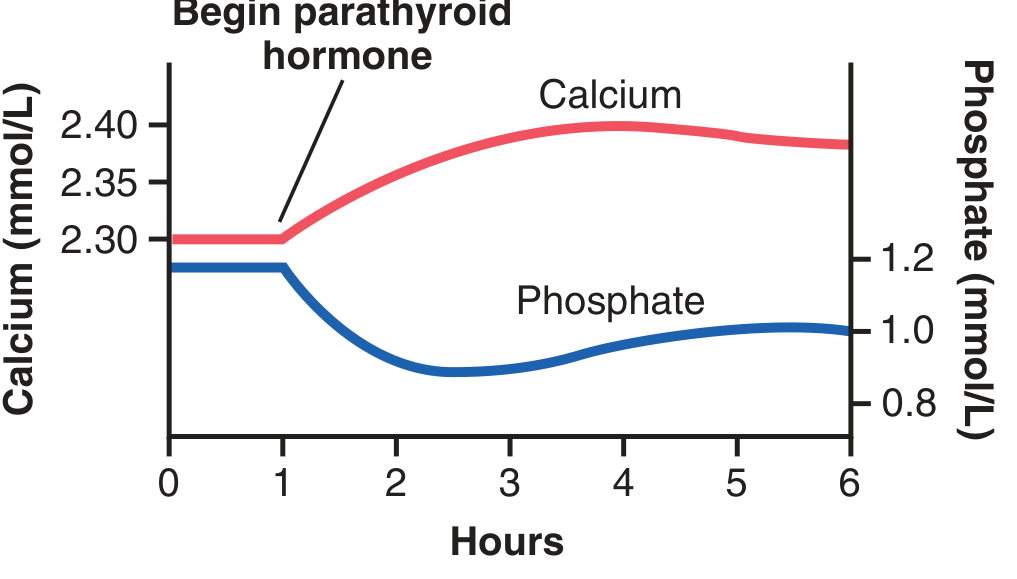
Figure: Approximate changes in calcium and phosphate concentrations during PTH infusion. Calcium rises within 1 hour; phosphate falls even faster due to renal excretion (Guyton and Hall Textbook of Medical Physiology, p. 989)
3. How PTH Mobilizes Calcium from Bone
PTH acts on bone through two distinct phases:
Phase 1 - Rapid Osteolysis (Minutes to Hours)
- PTH binds receptors on osteoblasts and osteocytes, activating the osteocytic membrane calcium pump
- The osteocytic membrane system is a network of interconnected cells spanning the entire bone, separated from extracellular fluid by a membrane layer
- Normally, bone fluid calcium is only ~1/3 of extracellular fluid calcium - PTH drives the pump harder, pulling calcium phosphate out of amorphous bone crystals into extracellular fluid
- This process - osteolysis - occurs without destroying the bone's fibrous/gel matrix
- Blood calcium begins rising within minutes of PTH exposure
"PTH activates the calcium pump strongly, thereby causing rapid removal of calcium phosphate salts from the amorphous bone crystals that lie near the cells."
- Guyton and Hall Textbook of Medical Physiology, p. 989
Phase 2 - Slow Osteoclastic Resorption (Days to Weeks)
- PTH stimulates osteoblasts/osteocytes to produce RANKL (Receptor Activator of NF-kB Ligand)
- RANKL binds RANK receptors on osteoclast precursors, driving their differentiation into mature, active osteoclasts
- PTH also reduces OPG (osteoprotegerin) production by osteoblasts - OPG is the decoy protein that normally blocks RANKL-RANK binding
- This slow phase takes several days to develop fully and leads to actual bone resorption (destruction of collagen matrix + mineral)
- After months of excess PTH, osteoclastic resorption dominates, and bones can develop large cavities filled with multinucleated osteoclasts
4. The RANKL/OPG/RANK Axis (Key Molecular Mechanism)
This is the central signaling system linking PTH to osteoclasts:
| Player | Source | Role |
|---|---|---|
| RANKL | Osteoblasts (stimulated by PTH) | Activates osteoclast differentiation and activity |
| RANK | Osteoclast precursors/osteoclasts | Receptor for RANKL |
| OPG (Osteoprotegerin) | Osteoblasts | Decoy receptor - blocks RANKL from reaching RANK, inhibits resorption |
| PTH | Parathyroids | Increases RANKL, decreases OPG - net effect: more osteoclast activity |
"PTH acts on the osteoblast to induce membrane-bound and secreted soluble forms of a protein called RANK (RANKL). RANKL acts on osteoclasts and osteoclast precursors to increase both the numbers and activity of osteoclasts."
- Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 1211
5. PTH and Sclerostin Inhibition
PTH also inhibits sclerostin production by osteocytes. Sclerostin is a protein that blocks osteoblast proliferation by inhibiting the Wnt/β-catenin pathway. By suppressing sclerostin:
- The Wnt pathway is disinhibited
- Osteoblast proliferation and bone formation is enhanced
- This is part of the anabolic mechanism of PTH
This pathway is exploited therapeutically: romosozumab (anti-sclerostin antibody) is used in osteoporosis, though unlike PTH, it suppresses rather than stimulates osteoclast activity.
6. Intermittent vs. Continuous PTH - The Anabolic vs. Catabolic Paradox
This is one of the most clinically important concepts regarding PTH and bone:
| Mode | Effect on Bone | Mechanism |
|---|---|---|
| Intermittent / Low-dose | Anabolic - net bone formation | Stimulates osteoblasts via cAMP/IGF-1 pathways; sclerostin inhibition dominates |
| Continuous / High-dose (endogenous excess or constant infusion) | Catabolic - net bone resorption | RANKL upregulation dominates; osteoclast activity exceeds osteoblast activity |
"Brief or intermittent treatment with PTH is anabolic; it stimulates bone deposition through cAMP/IGF-1 pathways in osteocytes and osteoblasts. Conversely, prolonged and continuous treatment is catabolic; it increases production of RANKL molecules by osteoblasts and T lymphocytes."
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology
This distinction underpins the clinical use of teriparatide (PTH 1-34) and abaloparatide (PTHrP analog) as once-daily subcutaneous injections for osteoporosis - the pulsatile/intermittent pattern tips the balance toward bone formation.
7. Bone as a Calcium Buffer
Bone contains ~1000x more calcium than all extracellular fluids combined. PTH uses bone as a massive reservoir:
- Short-term calcium deficit → PTH rapidly pulls calcium from exchangeable amorphous bone crystals
- Prolonged deficit (months to years) → osteoclastic resorption provides sustained calcium release
- If this continues too long (e.g., dietary calcium deficiency), bones eventually become depleted
"In effect, the bones provide a large buffer-reservoir of calcium that can be manipulated by PTH."
- Guyton and Hall Textbook of Medical Physiology, p. 991
8. Pathological States
Hypoparathyroidism
- Osteocytic resorption decreases, osteoclasts become nearly inactive
- Serum calcium falls (can drop from 9.4 to 6-7 mg/dL in 2-3 days after parathyroidectomy)
- Bones paradoxically remain strong (no excess resorption)
- Clinically: tetany, laryngospasm, risk of death from respiratory obstruction
Primary Hyperparathyroidism
- Usually caused by a parathyroid adenoma
- Prolonged PTH excess → massive osteoclast activation → bones become weak, develop large cavities
- Serum calcium elevated; phosphate low
- Classic bone finding: osteitis fibrosa cystica (brown tumors, "salt and pepper" skull on X-ray)
Secondary Hyperparathyroidism (Chronic Kidney Disease)
- Low 1,25(OH)2D + phosphate retention → reduced calcium → elevated PTH
- Continuous PTH stimulation causes renal osteodystrophy
- Both osteoclastic resorption AND osteoblast activation occur, but with pathological coupling
Summary Table
| PTH Effect on Bone | Mechanism | Time Course |
|---|---|---|
| Rapid calcium/phosphate mobilization | Osteolysis via osteocytic membrane pump | Minutes |
| Slow bone resorption | RANKL→RANK → osteoclast activation | Days to weeks |
| OPG inhibition | Reduces decoy receptor for RANKL | Hours to days |
| Sclerostin suppression | Disinhibits Wnt/β-catenin → osteoblast proliferation | Hours |
| Intermittent → anabolic | cAMP/IGF-1 → net bone formation | With pulsatile exposure |
| Continuous → catabolic | Net resorption via dominant RANKL effect | With sustained exposure |
Sources: Guyton and Hall Textbook of Medical Physiology (p. 989-993) | Katzung's Basic and Clinical Pharmacology, 16th Ed. (p. 1211-1215) | Brenner and Rector's The Kidney, 2-Volume Set (p. 2398)
This is a shared conversation. Sign in to Orris to start your own chat.