Mri vs ct scan in case of stroke
Reading File
Finding Sources
Finding Sources
Searching the Web
MRI vs CT scan in stroke diagnosis comparison 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full answer:
MRI vs CT Scan in Stroke
The Bottom Line Up Front
CT is first-line in the acute setting; MRI is the more sensitive and definitive study. In nearly every emergency department, a non-contrast CT is obtained immediately upon suspected stroke arrival. MRI, particularly diffusion-weighted imaging (DWI), is the gold standard for diagnosing ischemic stroke but has practical limitations in the acute phase.
CT Scan in Stroke
What it does well
- Hemorrhage detection: Non-contrast CT is highly sensitive and specific for acute intracranial hemorrhage (ICH, subarachnoid, subdural). This is the single most important use - distinguishing hemorrhagic from ischemic stroke changes management completely.
- Speed: Can be obtained and interpreted within minutes of arrival. Guidelines target brain imaging within 20 minutes of ED arrival.
- Availability: Widely available, including at rural/community hospitals, often with telemedicine interpretation support.
- Cost: Significantly cheaper than MRI.
- Ease: Suitable even for critically ill, combative, or claustrophobic patients.
- SAH diagnosis: Head CT is diagnostic in ~90% of subarachnoid hemorrhage (SAH) cases within the first 24 hours.
Limitations
- Insensitive for acute ischemic stroke: Most acute ischemic strokes are NOT visible on non-contrast CT in the first few hours. The scan in the early window is essentially "normal" in ischemic stroke, which is expected.
- Poor posterior fossa visualization: Bony artifact limits detection of brainstem and cerebellar infarcts.
- Radiation exposure: Uses ionizing X-rays.
Example - CT showing hemorrhagic stroke (hypertensive ICH, left putamen):
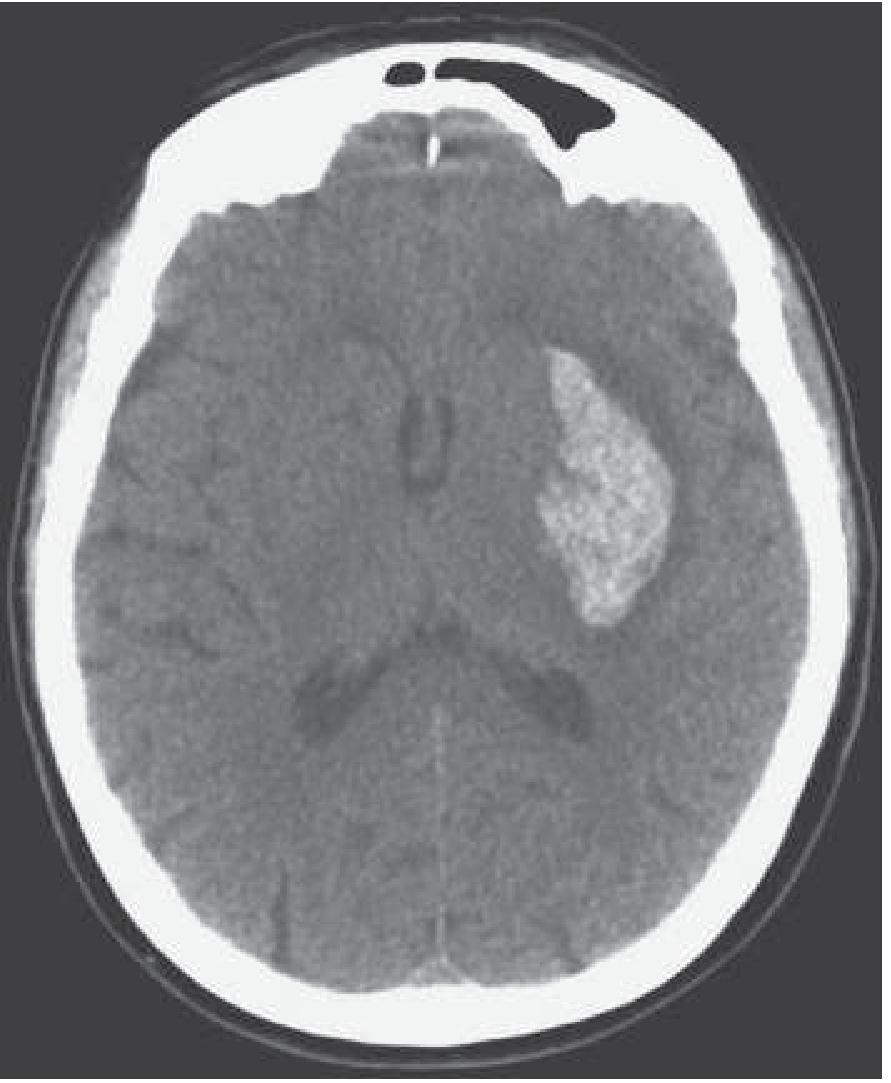
Non-contrast CT: the bright (hyperdense) area in the left basal ganglia = acute hemorrhage. - Harrison's Principles of Internal Medicine 22E
CT Angiography (CTA) - An Important Companion
CTA (CT with contrast for vessels) is now routinely obtained in suspected large vessel occlusion (LVO) - proximal MCA, carotid, or basilar artery - to identify candidates for endovascular thrombectomy. CT perfusion can also help delineate salvageable penumbra vs. core infarct. - Washington Manual of Medical Therapeutics
MRI in Stroke
What it does well
- Diffusion-weighted imaging (DWI): The most sensitive sequence for acute ischemia. Shows restricted diffusion (bright signal) within minutes of onset - far earlier than CT can detect infarction. This is the modality of choice when the diagnosis needs confirmation. - Adams & Victor's Principles of Neurology 12th ed.
- Posterior fossa: No bony artifact; excellent for brainstem, cerebellum, and small lacunar infarcts.
- Small/lacunar infarcts: CT routinely misses small deep infarcts; DWI does not.
- Stroke mimics: Better differentiation of tumors, demyelination (MS), encephalitis, abscess.
- Vascular imaging: MR Angiography (MRA) is a non-invasive way to assess carotid and intracranial vessels; MR Venography (MRV) evaluates for cerebral venous thrombosis.
- Old vs. new infarcts: Can distinguish acute (DWI bright, ADC dark) from chronic (DWI dark, T2 bright/gliosis).
MRI sequences and their uses:
| Sequence | Best For | Acute Ischemia Appearance |
|---|---|---|
| DWI | Earliest detection of ischemia | Bright (restricted diffusion) |
| ADC map | Confirms true restriction | Dark (low ADC) |
| FLAIR | Edema, gliosis, chronic changes | Bright (after ~6 hours) |
| T2 | Infarcts, inflammation, tumors | Bright (delayed) |
| T1 | Subacute hemorrhage, anatomy | Dark (edema); bright (subacute blood) |
| GRE / SWI | Microbleeds, old hemorrhage | Dark "blooming" |
From Adams & Victor's Principles of Neurology, Table 33-3
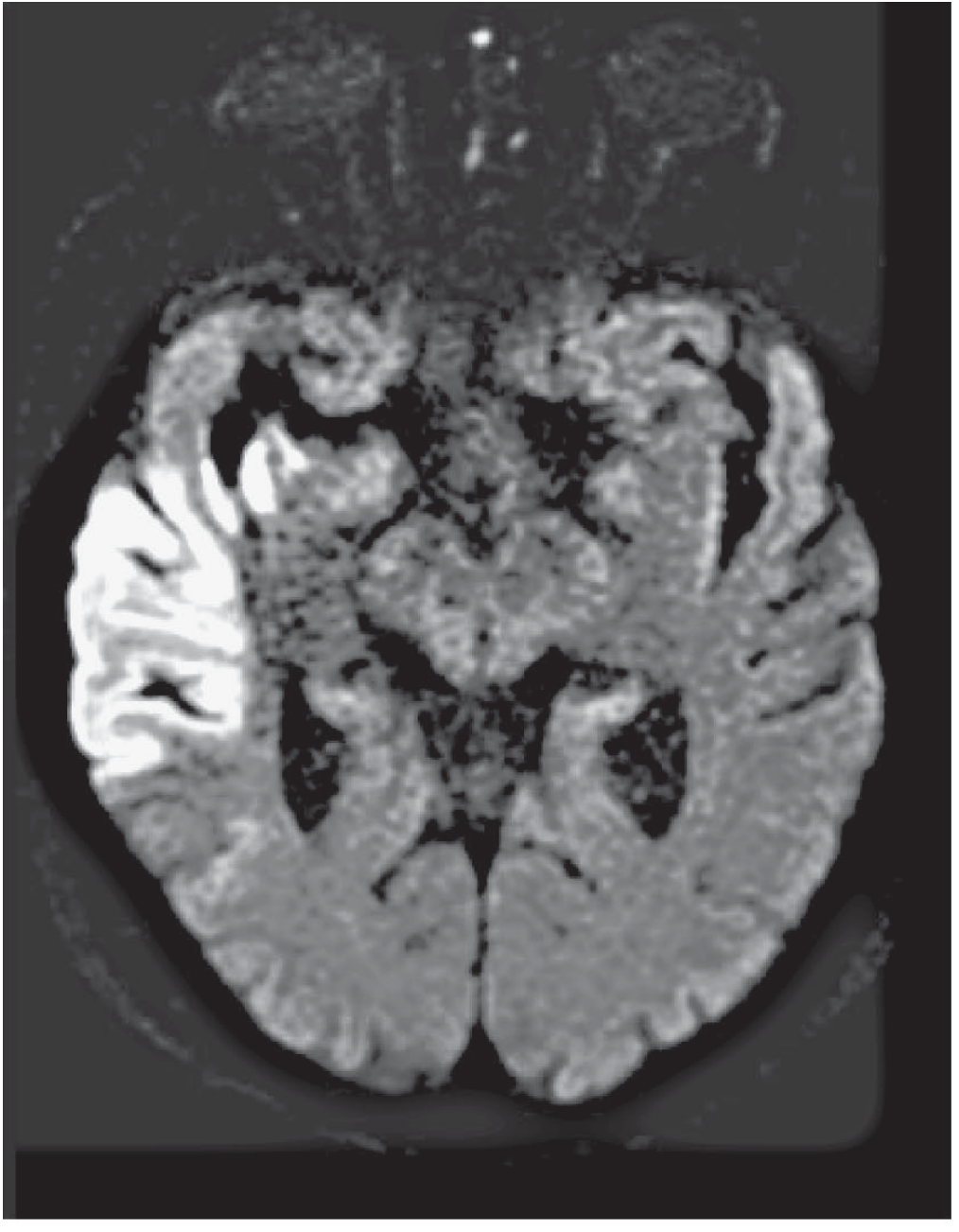
MRI DWI showing right MCA territory infarction (bright = acute ischemia):
Corresponding T2-FLAIR of the same patient (early vasogenic edema):
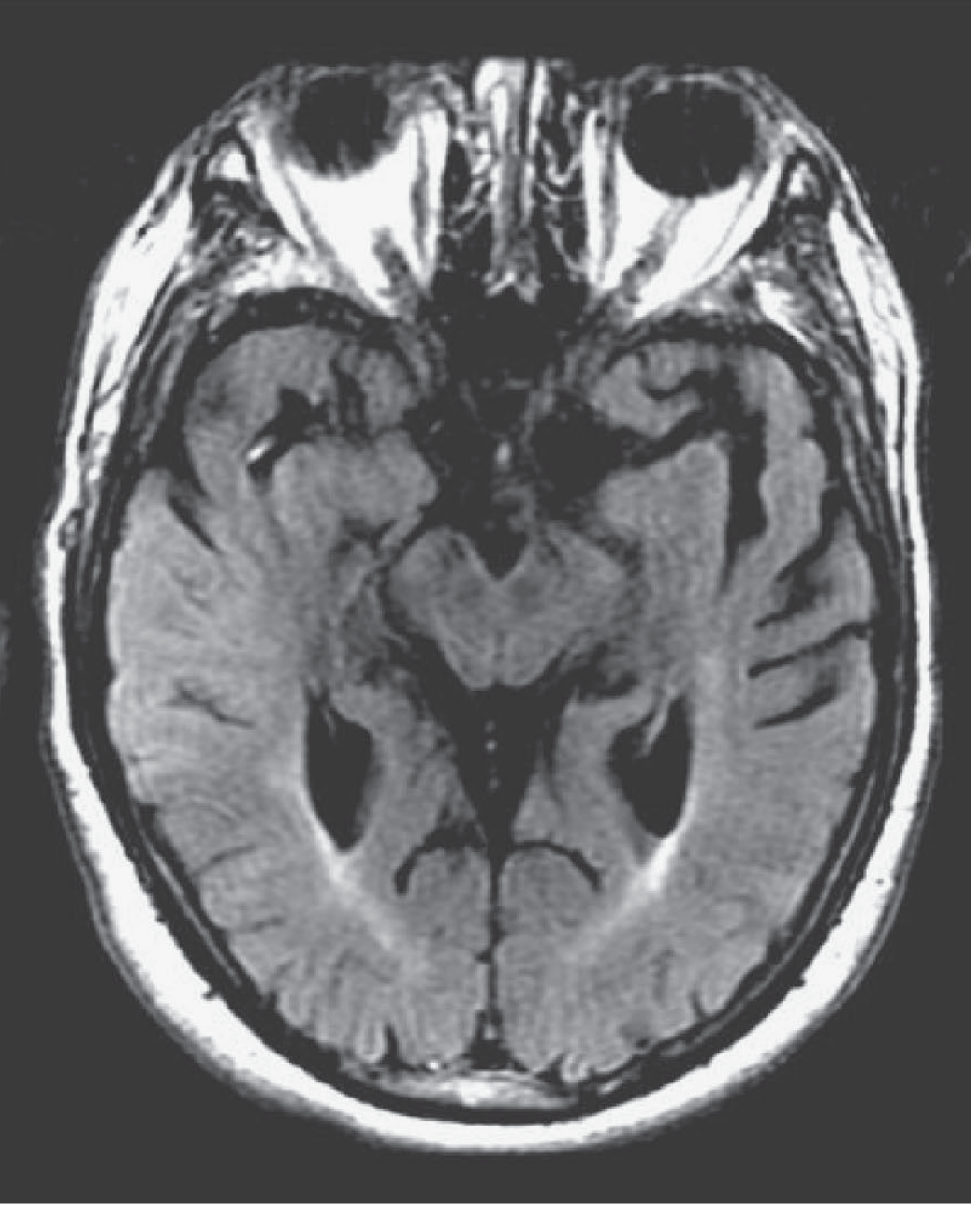
Figure 33-3: Right MCA infarction is clearly bright on DWI (left image), with subtle FLAIR changes (right). - Adams & Victor's Principles of Neurology 12th ed.
Limitations
- Time: Takes longer than CT; delays thrombolysis decision.
- Availability: Not universally available 24/7, especially in resource-limited settings.
- Contraindications: Pacemakers, metallic implants, severe claustrophobia.
- Cost: More expensive than CT.
- Acutely ill patients: Hard to image unstable, combative, or intubated patients.
- As Harrison's puts it: "MRI is more expensive and time consuming than CT and less readily available. Claustrophobia and the logistics of imaging acutely critically ill patients also limit its application."
Head-to-Head Comparison
| Feature | CT (Non-contrast) | MRI (DWI) |
|---|---|---|
| Speed | Fast (minutes) | Slower (20-40 min) |
| First-line acute stroke | Yes | Usually second-line |
| Hemorrhage detection | Excellent | Good (GRE/SWI); CT remains preferred |
| Acute ischemia (<6 hrs) | Poor / negative | Excellent |
| Posterior fossa | Poor (bone artifact) | Excellent |
| Small lacunar infarcts | Miss most | Detects most |
| Availability | Widely available | Limited in many EDs |
| Cost | Lower | Higher |
| Radiation | Yes | No |
| Thrombolysis decision | Standard tool | Can substitute if CT unavailable |
| Penumbra assessment | CT perfusion | MR perfusion |
| Vascular imaging | CTA | MRA |
Clinical Decision Framework
Acute presentation (0-4.5 hours, thrombolysis window):
- Do CT first - to rule out hemorrhage (absolute contraindication to tPA).
- CT negative + clinical stroke = treat (tPA decision does not require MRI).
- MRI/DWI if diagnosis uncertain or posterior circulation stroke suspected.
Suspected posterior circulation / brainstem stroke:
- MRI is strongly preferred - CT misses most of these.
Suspected small lacunar infarct:
- MRI DWI is the preferred modality.
Suspected cerebral venous thrombosis:
- MRI + MRV is the study of choice.
When CT is negative but SAH still suspected:
- CT-negative SAH → perform lumbar puncture (look for xanthochromia).
TIA / minor stroke (non-acute):
- MRI DWI should be performed to confirm the diagnosis and identify at-risk tissue.
Summary in one sentence: Non-contrast CT is the immediate, mandatory first step in any acute stroke to rule out hemorrhage and decide on thrombolysis, while MRI-DWI is the most sensitive modality for confirming ischemic stroke, detecting posterior fossa lesions, and differentiating stroke from mimics when time allows.
Sources: Harrison's Principles of Internal Medicine 22E, Adams & Victor's Principles of Neurology 12th Ed., Tintinalli's Emergency Medicine, Washington Manual of Medical Therapeutics, Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.