Laboratory diagnosis of myocardial infarction
Reading File
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction" AND "cardiac biomarkers" AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compose the full answer.
Laboratory Diagnosis of Myocardial Infarction
Myocardial infarction (MI) is diagnosed through a triad of clinical symptoms, electrocardiographic changes, and laboratory biomarkers. The laboratory component relies on detecting proteins released from irreversibly damaged myocytes into the bloodstream. Below is a thorough breakdown.
1. Pathophysiologic Basis of Biomarker Release
When coronary blood flow is interrupted, myocyte necrosis begins after approximately 20 minutes of ischemia. As the plasma membrane of necrotic cells becomes leaky, intracellular proteins - both cytoplasmic (free pool) and structural (myofilament-bound) - escape into the interstitium and ultimately reach the bloodstream. The quantity, timing, and peak level of these markers depend on:
- Volume of damaged myocardium
- Blood flow and lymphatic drainage in the infarct zone
- Rate of elimination of the marker from circulation
- Whether reperfusion has occurred (reperfusion causes earlier and higher peaks due to rapid "washout")
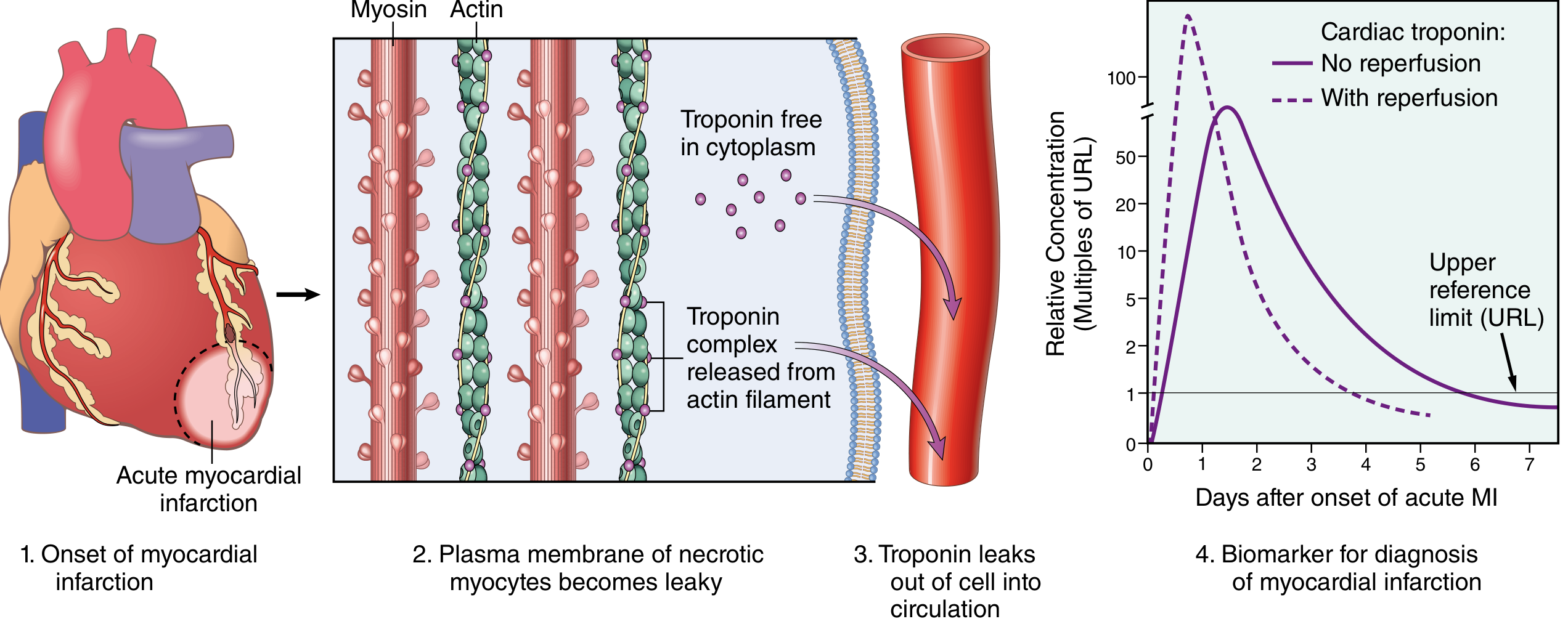
Troponin release in MI: free cytoplasmic pool causes an early rise; structural complex release sustains elevations. With reperfusion (dashed line), peak is higher and earlier; without reperfusion (solid line), the curve is broader and peaks later. - Robbins & Cotran, Pathologic Basis of Disease
2. Cardiac Troponins (cTnI and cTnT) - Primary Biomarkers
Structure and Cardiac Specificity
Cardiac troponin I (cTnI) and cardiac troponin T (cTnT) are components of the troponin-tropomyosin complex that regulates calcium-mediated contraction of cardiac muscle. Both have cardiac-specific isoforms not found in significant amounts in adult skeletal muscle, making them highly specific for myocardial injury.
Kinetics After MI
| Parameter | Timeline |
|---|---|
| First detectable rise | 2-4 hours after onset |
| Peak concentration | 24-48 hours |
| Return to baseline | 7-10 days (cTnI), 10-14 days (cTnT) |
| With reperfusion | Peak earlier and higher (washout effect) |
Diagnostic Threshold: The 99th Percentile Rule
The current universal standard, established by the ESC/ACC and reinforced through successive Universal MI Definition documents, requires:
- A rise and/or fall of cTn with at least one value above the 99th percentile upper reference limit (URL) of a healthy reference population
- The pattern of rise and fall (delta troponin) helps distinguish acute MI from chronic elevation (e.g., CHF, renal failure, sepsis)
"An increased concentration of cTn greater than the 99th percentile URL is required in the diagnosis of AMI." - Tietz Textbook of Laboratory Medicine, 7th Ed.
High-Sensitivity Cardiac Troponin (hs-cTn)
High-sensitivity assays (hs-cTnI, hs-cTnT) can detect troponin in the blood of 90-100% of patients with AMI at the time of hospital arrival. Key features:
- Allow earlier rule-in/rule-out protocols (0h/1h or 0h/2h algorithms)
- Can detect very small amounts of myocardial injury that older assays missed
- Increased sensitivity comes at some cost to specificity (34-80% depending on cutoff), so clinical context remains essential
- Serial measurements and delta criteria (absolute/relative change) are critical to distinguish acute from chronic injury
"New high-sensitivity cardiac troponins have improved ability to detect ischemia. The high-sensitivity troponins identify 90% to 100% of patients with AMI at the time of arrival using the lowest cut point." - Tintinalli's Emergency Medicine
3. Older / Secondary Biomarkers
Creatine Kinase-MB (CK-MB)
CK-MB was the gold standard before troponins. It is the MB isoenzyme of creatine kinase, with higher cardiac selectivity than total CK. Its role has diminished substantially:
- Rise: 4-6 hours after MI
- Peak: 18-24 hours
- Return to baseline: 48-72 hours (much faster than troponin)
- Limitation: Present in both skeletal and cardiac muscle - lacks the specificity of cTn
- Current role: No longer recommended for initial diagnosis of NSTEMI. May be used to detect reinfarction (since it clears faster, a secondary rise can be detected while troponin remains elevated from the initial event). - Washington Manual of Medical Therapeutics
Myoglobin
- A non-specific heme protein present in both cardiac and skeletal muscle
- Earliest to rise after MI (1-2 hours), peaks at 4-8 hours, returns to baseline within 24 hours
- Very sensitive but not cardiac-specific - elevated in skeletal muscle injury, renal failure
- Historical use: early rule-out in the first 2 hours; now superseded by hs-cTn
- A negative myoglobin within 4 hours of symptom onset had high negative predictive value
Lactate Dehydrogenase (LDH)
- LDH-1 isoenzyme (predominant in heart) rises later than CK-MB
- Rise: 24-48 hours
- Peak: 3-6 days
- Return to baseline: 8-14 days
- Flipped LDH ratio: LDH-1 > LDH-2 (normally LDH-2 > LDH-1) is characteristic of MI
- Largely replaced by troponin but still used in late-presenting patients (>24-72 hrs after event) where troponin may have peaked/fallen but LDH remains elevated
Aspartate Aminotransferase (AST/SGOT)
- Historically used, now abandoned for cardiac diagnosis
- Rises at 8-12 hours, peaks at 18-36 hours, normalizes by 3-4 days
- Present in liver, red cells, skeletal muscle - completely non-specific
4. Summary: Biomarker Kinetics Comparison
| Marker | Rise | Peak | Returns to Normal | Specificity |
|---|---|---|---|---|
| hs-cTn (cardiac troponin) | 1-3 h | 12-24 h | 7-14 days | Highest |
| cTn (conventional) | 2-4 h | 24-48 h | 7-10 days | High |
| CK-MB | 4-6 h | 18-24 h | 48-72 h | Moderate |
| Myoglobin | 1-2 h | 4-8 h | 24 h | Low |
| LDH (LDH-1) | 24-48 h | 3-6 days | 8-14 days | Low-moderate |
| AST | 8-12 h | 18-36 h | 3-4 days | Very low |
5. Non-Cardiac Causes of Troponin Elevation ("Troponin Leak")
Low-level troponin elevation without the characteristic rise-and-fall pattern of AMI can occur in:
- Congestive heart failure (chronic myocyte stress)
- Pulmonary embolism
- Renal failure (impaired clearance)
- Sepsis and critical illness
- Myocarditis
- Myocardial trauma (contusion)
- Hypertensive emergency
- Tachyarrhythmias
- Post-cardioversion / post-ablation
"Serial measurements may be helpful in distinguishing different etiologies." - Robbins & Cotran, Pathologic Basis of Disease
The delta troponin (change in value over time) is the key discriminator: an acute rise-and-fall pattern with a significant delta (e.g., >20% relative or absolute change per assay) supports AMI, while a flat persistently elevated level suggests chronic injury.
6. Other Supporting Laboratory Tests
While not diagnostic of MI by themselves, these tests are routinely ordered:
| Test | Finding in MI | Purpose |
|---|---|---|
| CBC | Leukocytosis (12,000-15,000/μL) within hours | Stress response; peaks day 2-3 |
| ESR / CRP | Elevated (CRP peaks day 2-3) | Inflammatory marker; prognostic |
| Blood glucose | Often elevated | Stress hyperglycemia; poor prognosis marker |
| Lipid profile | Cholesterol falls acutely after MI (within 24 h) | Baseline/risk; must measure within 24h or wait 6-8 weeks |
| BNP / NT-proBNP | Elevated with significant LV dysfunction | Identifies pump failure, risk stratification |
| Coagulation tests | D-dimer, PT/INR | Pre-anticoagulation baseline |
| Renal function (BMP/CMP) | Baseline before contrast/medications | |
| ABG | Hypoxemia | If respiratory compromise |
7. Universal Definition of MI - Biochemical Criterion
Per the Fourth Universal Definition of MI (2018, ESC/ACC/AHA/WHF), the detection of a rise and/or fall of cardiac troponin with at least one value above the 99th percentile URL is the biochemical cornerstone for all types of MI (Types 1-5), along with at least one of:
- Symptoms of acute myocardial ischemia
- New ischemic ECG changes
- Development of pathological Q waves
- Imaging evidence of new loss of viable myocardium or regional wall motion abnormality consistent with ischemic etiology
- Identification of a coronary thrombus by angiography or autopsy
8. Practical Approach: Serial Sampling Protocol
- On presentation (T=0): Draw troponin immediately
- At 1-3 hours (T+1 or T+3): Repeat troponin (0h/1h or 0h/3h protocol depending on assay)
- At 6 hours: If initial samples negative, repeat at 6h to maximize sensitivity
- A negative hs-cTn at 0h AND 1-2h with low clinical probability effectively rules out AMI in most patients
Key sources:
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Chapter on Cardiac Function (Apple, Kavsak, Jaffe)
- Robbins & Cotran Pathologic Basis of Disease (10th Ed.) - Chapter 12: Clinical Features of MI
- Tintinalli's Emergency Medicine - Serum Markers of Myocardial Injury
- The Washington Manual of Medical Therapeutics - Laboratories
- Frameworks for Internal Medicine - Acute Coronary Syndrome
Recent evidence (2024-2026): A 2026 systematic review (PMID: 41500560) examined biomarker utility specifically in Type 2 MI (supply-demand mismatch), highlighting that troponin patterns and clinical context remain essential for distinguishing MI subtypes even with hs-cTn assays.
This is a shared conversation. Sign in to Orris to start your own chat.