Tracheo esophageal prosthesis
Reading File
Finding Sources
Finding Sources
Searching PubMed
tracheoesophageal prosthesis voice restoration laryngectomy
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of the Tracheoesophageal (TE) Prosthesis:
Tracheoesophageal (TE) Prosthesis
What It Is
A tracheoesophageal (TE) prosthesis is a small one-way silicone valve inserted into a surgically created tract (tracheoesophageal fistula/TEF) between the posterior wall of the tracheal stoma and the anterior wall of the cervical esophagus. It is the gold standard for voice rehabilitation after total laryngectomy.
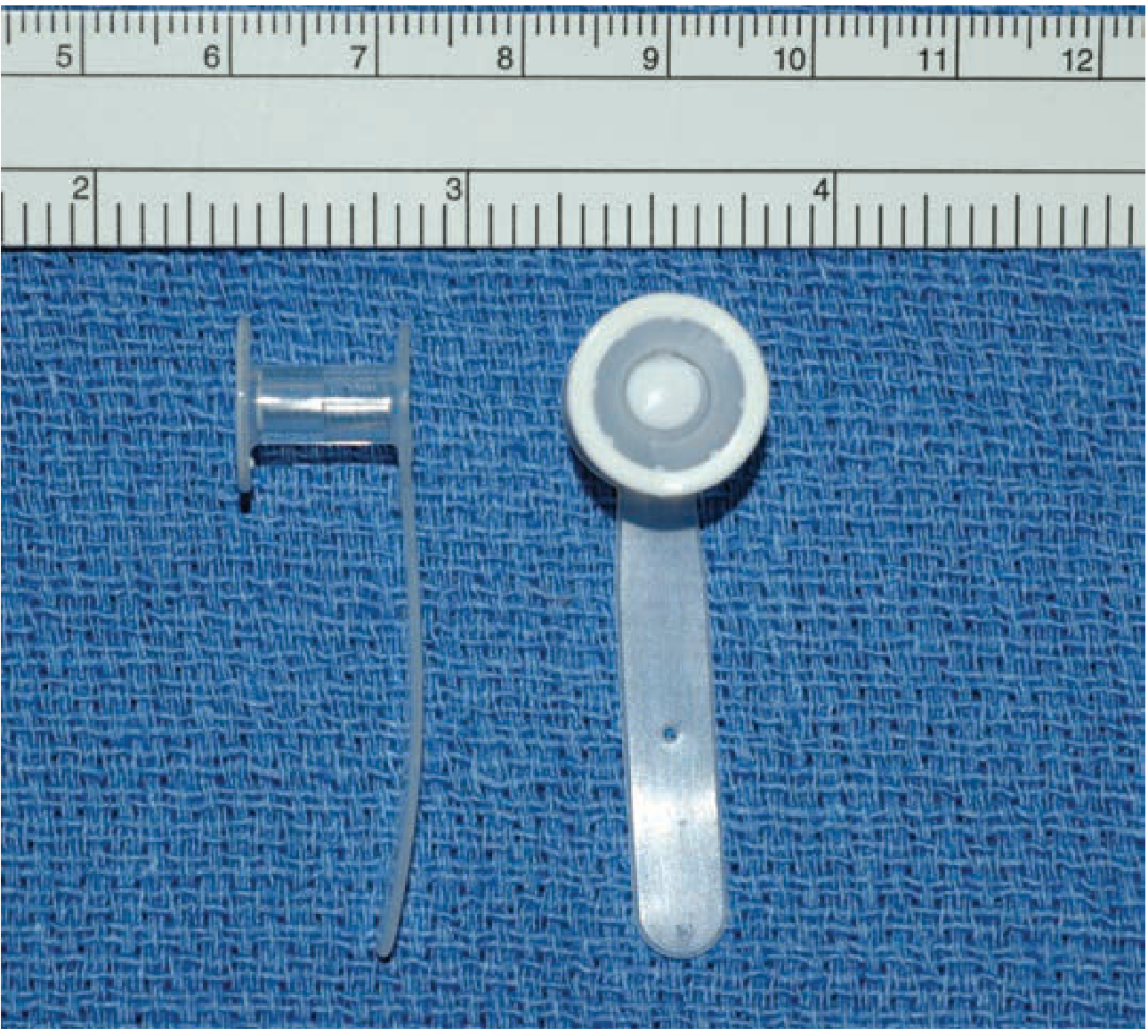
The bobbin-shaped TE prosthesis: the smaller flange sits in the esophagus; the larger flanged end with the retention tab sits at the posterior tracheostoma.
Why It Is Used
After total laryngectomy, the patient loses the natural voice-producing larynx. Three options exist for speech rehabilitation:
| Method | Description | Success Rate |
|---|---|---|
| Tracheoesophageal voice (TEP) | Air diverted via prosthesis to vibrate esophagus | >90% functional speech |
| Electrolarynx | Electric vibration device held against neck/cheek | Useful post-op but robotic quality |
| Esophageal speech | Patient swallows and belches air to create sound | <20% achieve fluent speech |
TEP is the preferred option because voice production can be achieved on the day of insertion in many patients.
Mechanism of Action
- The patient occludes the tracheostoma with a thumb or finger (or a hands-free heat-moisture exchanger valve)
- Exhalation forces air through the one-way prosthesis valve into the upper esophagus
- The air vibrates the esophageal walls (similar to a belch), generating a tone
- The patient articulates this tone into speech using the lips, tongue, and palate
The valve prevents retrograde passage of food or saliva from the esophagus into the trachea (aspiration prevention).
Timing of Placement
- Primary TEP: Created at the time of laryngectomy (if wound-healing complications are not anticipated)
- Secondary TEP: Created as an outpatient procedure ~4 weeks post-resection, using a flexible esophagoscope to guide puncture placement
- Primary and secondary TEP have similarly high complication rates; the extent of pharyngeal reconstruction (not prior radiation) is a more important factor in timing selection
Types of Prostheses
| Type | Description |
|---|---|
| Indwelling (non-removable) | Placed/removed by a clinician only; lasts 3-6+ months; e.g., Provox (Atos Medical) |
| Patient-removable | Patient can insert/remove for cleaning; replaced more frequently |
Well-known commercial prostheses include Provox Vega and the Blom-Singer series.
Complications
1. Leakage (most common)
- Around the valve (peri-prosthetic): due to enlargement of the TEF fistula - fluid tracks around the outside of the prosthesis
- Through the valve lumen: valve dysfunction/failure
- Confirmed by having the patient drink a colored liquid (e.g., grape juice) while inspecting the prosthesis
- Risk: aspiration pneumonia
- Management: Remove prosthesis, insert a Foley catheter (uninflated) to maintain fistula patency until specialist follow-up. Do NOT attempt catheter placement if the tract is <2 weeks old (risk of false passage)
2. Valve aspiration/extrusion
- Prosthesis dislodges and can be aspirated
- Symptoms: persistent cough, dyspnea, respiratory distress
- Diagnosis: chest radiograph (prosthesis is radiopaque)
- The TEF tract closes within 24-48 hours of dislodgement - a Foley or red rubber catheter must be inserted promptly to maintain patency
- Requires otolaryngology consultation
3. Biofilm formation
- Candida colonization on silicone degrades the valve, causing it to fail
- Limits prosthesis lifespan
- Antifungal prophylaxis (nystatin, amphotericin lozenges) and antifungal-impregnated prostheses have been studied to reduce biofilm
4. Cricopharyngeal spasm
- Can impair sound production / fluency
- Managed with botulinum toxin injection into the cricopharyngeus (percutaneous or endoscopic)
- A test block with 1% lidocaine infiltration can predict response
5. Stenosis of the TEF tract
- Can develop post-operatively; may present as difficulty producing speech in addition to dysphagia
Emergency Management Summary (TE Prosthesis in the ED)
| Problem | Action |
|---|---|
| Leaking prosthesis | Remove prosthesis; insert uninflated Foley catheter to maintain TEF patency; ENT follow-up next day |
| Aspirated/extruded prosthesis | CXR; insert Foley/red rubber catheter to maintain tract; ENT consult |
| Tract <2 weeks old | Do NOT attempt catheter - risk of false passage |
Role of the Speech-Language Pathologist (SLP)
SLP involvement is essential throughout the process:
- Pre-operative counseling on speech options
- Prosthesis sizing and fitting
- Voice training post-insertion
- Long-term compliance and troubleshooting
Recent Evidence
Two recent systematic reviews are relevant:
-
Biofilm strategies on voice prostheses (Tsikopoulos et al., J Voice 2025, PMID 37625903) - reviews approaches to inhibit Candida/bacterial biofilm on silicone, which is the primary driver of prosthesis failure.
-
TE voice therapy post-laryngectomy (Sparks et al., J Voice 2026, PMID 38000962) - systematic review confirming the importance of structured voice therapy in optimizing outcomes after TE prosthesis placement.
Sources: Tintinalli's Emergency Medicine, 9th ed. | Cummings Otolaryngology Head and Neck Surgery | Schwartz's Principles of Surgery, 11th ed.
Terminal care of head and neck cancer patients
Reading File
Finding Sources
Finding Sources
Searching PubMed
"head and neck cancer" AND "palliative care" AND "end of life"
Reading File
Finding Sources
Searching PubMed
"head and neck cancer" AND "palliative care"
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive material. Let me compile the full response.
Terminal / Palliative Care of Head and Neck Cancer Patients
Overview and Scope
Head and neck cancer accounts for ~8,000 cases per year in England and Wales, and approximately half of all patients will die from their illness and require palliative support. The WHO defines palliative care as "total active care of patients whose disease is not responsive to curative treatment," encompassing physical, psychological, social, and spiritual dimensions.
These patients represent a uniquely complex group because:
- The disease and its treatments profoundly impair functions essential to human identity - communication, swallowing, and breathing
- The boundary between "radical" and "palliative" treatment is blurred (e.g., major resections with limited prognosis)
- Functional deficits lead to social isolation and depression
- Histological confirmation of recurrence can be difficult after prior treatments
An estimated 20% of head and neck cancer patients qualify for palliative care input at the time of initial diagnosis, with an average survival of 5 months within this cohort.
When to Refer for Palliative Care
Indications for palliative care referral (Shuman et al.):
- Unresectable locoregional disease and/or distant metastasis at initial presentation
- Recurrent unresectable disease and/or distant metastasis after treatment
- Patients unable to tolerate anticancer treatment due to disease stage, comorbidity, functional status, or patient preference
A proactive approach integrating palliative care early in the disease trajectory (not just immediately before death) is now strongly advocated.
Symptom Prevalence in Terminal Head and Neck Cancer
| Symptom | Prevalence Range (across studies) |
|---|---|
| Pain | 62-99% (severe pain in ~77%) |
| Dysphagia | 45-90% |
| Weight loss / anorexia | 43-98% |
| Breathing / airway difficulties | 22-52% |
| Feeding difficulties | 32-89% |
| Fatigue / weakness | ~39% |
| Bleeding | 9-47% |
Patients had a mean of 4.7 symptoms in the last 6 months of life.
1. Pain Management
Types of cancer pain:
- Nociceptive pain - from local compression or invasion by the tumour
- Neuropathic pain - from peripheral/central nervous system dysfunction (due to tumour or prior treatment)
- Mixed presentations are common
WHO Pain Ladder approach:
- Step 1: Non-opioids (e.g., regular paracetamol)
- Step 2: Add weak opioid (e.g., codeine)
- Step 3: Substitute strong opioid - morphine remains the drug of choice for moderate-to-severe pain
Neuropathic pain additions:
- First-line: anti-convulsant (gabapentin) or anti-depressant (amitriptyline)
- Nerve compression: trial of dexamethasone (corticosteroid)
- Refractory: methadone, ketamine, interventional pain procedures
Breakthrough pain:
- Defined as transient exacerbation despite stable background analgesia
- Use short-acting opioid preparations: oral morphine (oramorph/oxynorm)
- Newer formulations: fentanyl (sublingual, buccal, intranasal) - equal efficacy, faster onset, but reserved for movement-related or sudden short-lived pain; requires baseline of ≥60 mg oral morphine equivalent
Opioid-induced neurotoxicity - accumulation of metabolites causes:
- Myoclonus, visual hallucinations, confusion, drowsiness
- Management: reduce dose if pain controlled, check renal function (metabolites accumulate), or opioid switch (e.g., morphine → oxycodone / hydromorphone)
- If renal impairment: use renally-independent opioids e.g., alfentanil
Route of administration - a key challenge in head and neck cancer:
- Oral route often unavailable - use PEG/gastrostomy tube (note: do NOT crush sustained-release preparations - use Zomorph granules or MST Continus suspension)
- Transdermal fentanyl patches: changed every 72 hours; suitable only once pain is stable; less flexible for titration
- Subcutaneous infusion via syringe driver is often preferred in the terminal phase
2. Respiratory Tract Secretion Management
At end of life, retained secretions cause distress for the patient and family ("death rattle"). Three main anti-secretory drugs:
| Drug | Notes |
|---|---|
| Glycopyrronium | Preferred - less sedation, less agitation than hyoscines |
| Hyoscine hydrobromide | Effective; may cause agitation/sedation |
| Hyoscine butylbromide | Peripheral action; less CNS penetration |
- Balance: reduce secretions without making them too tenacious
- If oral/gastrostomy route unavailable: transdermal hyoscine hydrobromide (Scopoderm) patches
3. Communication Difficulties
As disease progresses, speech becomes increasingly impaired:
- Alternative aids: electronically generated speech devices, written communication
- Loss of communication subtleties has a profound psychological impact
- Advance care planning (ACP) becomes especially important early, while patients can still communicate
- Open-ended discussions about goals of care and future complications should be proactive
4. Terminal Haemorrhage ("Carotid Blowout")
This is a feared catastrophic event, but actual incidence is lower than perceived:
- Rupture of the carotid artery system occurs in an estimated 3-5% of patients who have undergone major head and neck resections
Risk factors:
- Tumour-related: proximity to the carotid artery
- Treatment-related: previous radical neck dissection and/or radiotherapy; post-operative wound healing problems
- Systemic: coagulopathy; age >50; 10-15% weight loss; comorbidities (e.g., diabetes)
Warning signs:
- A herald (sentinel) bleed may precede the fatal haemorrhage
- Visible ballooning or pulsation of the carotid
Prevention:
- Review and stop anticoagulants (warfarin, heparin)
- Review drugs affecting platelet function: NSAIDs, aspirin, SSRIs
- If sentinel bleed occurs: arterial embolization by interventional radiology can delay or abrogate further bleeding
Emergency management (Ubogagu and Harris guidelines):
| Step | Action |
|---|---|
| 1 | Stay with the patient and family to reduce anxiety and distress |
| 2 | Use dark towels to reduce visibility of blood |
| 3 | Give anxiolytic: midazolam 10 mg deep intramuscular injection (rapid onset, short duration) |
| 4 | Pre-emptively prescribe midazolam before the event occurs |
- Goal of midazolam: reduce patient's awareness and distress; provides retrograde amnesia if the patient survives
- Opioids are generally not needed unless haemorrhage is not terminal and patient reports pain
- At home: full MDT discussion required; community healthcare teams and ambulance service must be briefed in advance
5. Airway Obstruction
Causes at end of life:
- Retention of secretions
- Tumour encroachment into the airway or tracheostomy
Management:
- Decision-making about escalation must be pre-planned
- Palliative surgical options: tracheostomy or tumour debulking in the airway (if appropriate)
- Stridor: high-dose dexamethasone 8-16 mg subcutaneously may reduce peritumour oedema
- Pre-emptive prescription of midazolam (anxiolytic) for the terminal event
6. Holistic / Psychosocial Care
Depression
- Highly prevalent; independently predicts poorer quality of life
- Head and neck cancer patients have a disproportionately higher suicide risk than the general cancer population (linked to male predominance, tobacco/alcohol use, limited social support)
- Screen with brief tools: anhedonia (loss of interest/pleasure) and low mood
- Treatment: psychotherapy + antidepressants
- SSRIs first-line over tricyclics (better tolerability)
- Caution: SSRIs increase GI bleeding risk - significant consideration in this group
- Mirtazapine: useful if appetite stimulation and sedation are acceptable (give at night)
Spiritual Care
- Explore meaning, purpose, hope, and coping at every consultation
- Example questions: "What gives you hope and strength?" / "How are you coping?"
Ethical Issues
Four principles framework:
- Autonomy - patient's right to decide
- Beneficence - act to provide benefit
- Non-maleficence - avoid harm
- Justice - fair use of resources
Key ethical challenges specific to head and neck cancer:
- Provision of artificial nutrition and hydration as death approaches (especially when patient preference is unclear)
- Communication difficulties making patient-centred decision-making harder - forward planning while patients can still communicate is essential
Multidisciplinary Team
Terminal care of head and neck cancer patients requires an integrated MDT including:
- Specialist palliative care physician and nurses
- Otolaryngologist / head and neck surgeon
- Speech-language pathologist
- Dietitian
- Clinical psychologist / psychiatrist
- Chaplain / spiritual care
- Social worker
- Community nursing / hospice teams
- Ambulance service (for home-based terminal events)
Note on recent evidence: A 2024 review on ethics and palliation in head and neck surgery (Hochfelder & Shuman, Surg Oncol Clin N Am 2024, PMID 39244287) addresses the ethical complexities in this population and supports early, integrated palliative involvement.
Primary source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 21 - "The Role and Challenges in Providing Palliative Care to Head and Neck Cancer Patients"
Masked mastoiditis
Reading File
Finding Sources
Finding Sources
Searching PubMed
masked mastoiditis diagnosis complications treatment
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
All the key content has been gathered. Here is the complete, structured overview:
Masked Mastoiditis
Definition
Masked mastoiditis is a form of chronic mastoiditis in which the typical overt clinical signs of acute mastoiditis (post-auricular swelling, erythema, tenderness, pinna protrusion) are absent or suppressed, yet granulation tissue formation and bone erosion continue silently within the mastoid. It is called "masked" because the clinical presentation is misleadingly quiet while the disease progresses - often to serious intratemporal or intracranial complications.
Two things are key to its successful diagnosis and management:
- Cummings Otolaryngology
Pathogenesis / Why It Is "Masked"
The condition arises almost exclusively in patients who have received multiple courses of antibiotics for acute otitis media (AOM). The mechanism:
- Antibiotics partially treat the middle ear and most of the mastoid
- A focal area of persistent infection in the mastoid does not respond - typically behind a blocked aditus
- Granulation tissue blocks the aditus ad antrum, creating an anaerobic pocket
- Anaerobic organisms (Peptococcus spp., Bacteroides spp.) thrive in this low-virulence environment
- An indolent osteitis develops, causing little or no pain - hence the disease is "masked"
- Meanwhile, bone destruction continues and complications develop insidiously
Clinical Features
The presentation is characteristically subdued, especially in children:
| Feature | Description |
|---|---|
| History | Prior AOM apparently resolved after antibiotics |
| Symptoms (children) | Persistent mild irritability, diarrhea, tugging at the ear |
| Pain | Chronic but not severe auricular and post-auricular pain |
| Tenderness | Slight but definite tenderness to percussion over the mastoid cortex |
| Otorrhoea | Usually absent (tympanic membrane may be intact or near-normal) |
| Tympanic membrane | Often thickened but intact; may appear near-normal |
| Post-auricular swelling | May be absent, or if present - painless (unlike typical acute mastoiditis) |
In the infant shown below, the only visible sign was subtle protrusion of the left ear - with no post-auricular erythema or pain:
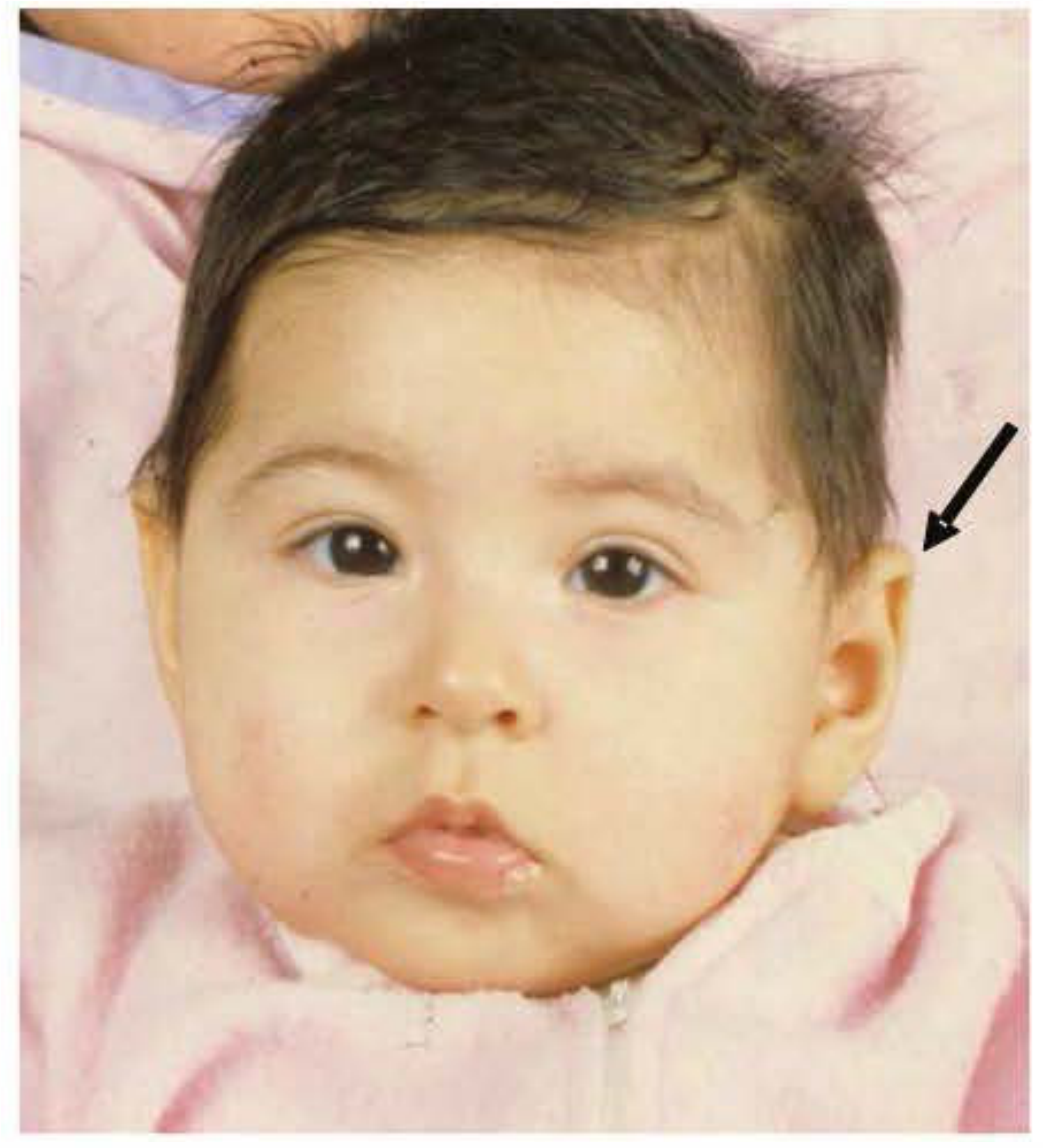
Clinical photograph of baby with left "masked mastoiditis." Arrow points to the protruding left ear. (Shambaugh - Surgery of the Ear, Fig. 26-4)
Diagnosis
A high index of suspicion is essential. Never be falsely reassured by a normal-looking tympanic membrane in a patient with persistent ear symptoms and prior antibiotic courses.
CT scan of the temporal bones is the investigation of choice:
- Shows localized opacification in an otherwise aerated mastoid (focal disease, not diffuse)
- Identifies bone destruction, coalescence, and extent of disease

Axial temporal bone CT: opacification of the middle ear (white arrow) and mastoid (black arrow). (Cummings Otolaryngology, Fig. 141.3)
- CT with IV contrast is recommended when intracranial or vascular complications are suspected (to look for thrombophlebitis, epidural or intracranial involvement)
- A low threshold for CT should be maintained in any child with persistent ear symptoms following antibiotic treatment
Complications
Because the diagnosis is delayed, masked mastoiditis commonly presents with a complication already established. In the landmark series of 9 cases by Holt and Gates, the following intratemporal and intracranial complications were found:
| Complication | Cases (n=9) |
|---|---|
| Epidural abscess | 2 |
| Meningitis | 2 |
| Meningitis + epidural abscess | 1 |
| Brain abscess | 2 |
| Cerebritis | 1 |
| Facial nerve paralysis | 1 |
Other potential complications include:
- Subperiosteal abscess (can be painless)
- Labyrinthitis (acute suppurative)
- Petrous apicitis (Gradenigo's syndrome: otorrhoea, ipsilateral abducens palsy, retro-orbital pain)
- Sigmoid sinus thrombosis
- Bezold's abscess (spread to digastric triangle)
Treatment
Surgical mastoidectomy is the definitive and only curative treatment. Medical management alone is insufficient for established masked mastoiditis.
- Cortical mastoidectomy is typically performed to eradicate the diseased air cell system
- Surgical excision eliminates symptoms and resolves the focal infection
- If a subperiosteal abscess is present, drainage is performed at the same time
- IV antibiotics are given perioperatively and directed by culture results
Chronic mastoiditis is a surgical condition - antibiotics alone will not eliminate the disease, and their continued use simply perpetuates the "masking" effect.
Key Teaching Points
| Point | Detail |
|---|---|
| Cause | Partial antibiotic treatment of AOM creates an anaerobic pocket of indolent osteitis |
| Organisms | Anaerobic (Peptococcus, Bacteroides) - low virulence, minimal symptoms |
| Trap | Normal or near-normal TM does not exclude significant mastoid disease |
| Investigation | Low threshold for CT temporal bones (with contrast if complications suspected) |
| Treatment | Surgical mastoidectomy - not more antibiotics |
| Risk | Presents with established intracranial complications (brain abscess, meningitis) |
A recent 2026 case report (PMID 41994730) documented masked mastoiditis presenting as pneumococcal meningoencephalitis in an elderly patient - reinforcing that this diagnosis can be missed at any age and in any setting, including the emergency department.
Sources: Cummings Otolaryngology Head and Neck Surgery | Shambaugh Surgery of the Ear | K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.