Approach to fever
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content to deliver a thorough answer on the approach to fever. Let me compile this into a well-structured response.
Approach to Fever
1. Definition and Normal Temperature
The traditional "normal" of 98.6°F (37.0°C) came from a 150-year-old study of axillary measurements. Contemporary data show the mean axillary temperature is closer to 96.75°F (36°C) and mean oral temperature ~36.5°C (98°F). Body temperature follows a circadian rhythm - nadir in early morning (~6 AM) and zenith in the afternoon.
Fever is defined as a body temperature above the usual range of normal, typically accepted clinically as:
- Oral temperature ≥38.3°C (101°F)
- Rectal temperature is 0.5°C higher; axillary is 0.5°C lower
2. Pathophysiology
The Pyrogen Cascade
When bacteria, viruses, or tissue breakdown products are present, macrophages, leukocytes, and large granular killer lymphocytes phagocytize them and release cytokines - the endogenous pyrogens. The most important is IL-1 (Interleukin-1), also called endogenous pyrogen, which:
- Reaches the hypothalamus via the bloodstream
- Stimulates release of prostaglandins (especially PGE2) via arachidonic acid pathway
- Raises the hypothalamic thermostat set-point
- The body responds by vasoconstriction + shivering (chills/rigors) to generate and conserve heat until the new set-point is reached
Other key pyrogenic cytokines include IL-6 and TNF-α.
Exogenous pyrogens (e.g., bacterial lipopolysaccharide/endotoxin from gram-negative bacteria) act indirectly - they stimulate cytokine release with several hours' latency. As little as one ten-millionth of a gram of endotoxin LPS can cause fever.
The mechanism of defervescence: when the set-point is lowered (e.g., by antipyretics inhibiting prostaglandin synthesis), the patient sweats and vasodilates to dissipate excess heat.
Source: Guyton and Hall Textbook of Medical Physiology; Goldman-Cecil Medicine
3. Causes of Fever
Fever can be broadly categorized as:
Infectious (most common)
| Category | Examples |
|---|---|
| Bacterial | Pneumonia, UTI, endocarditis, abscess, meningitis, TB, septicemia |
| Viral | Influenza, EBV, CMV, HIV, dengue, hepatitis |
| Fungal | Histoplasmosis, cryptococcosis, candidiasis |
| Parasitic | Malaria, toxoplasmosis, visceral leishmaniasis |
Non-infectious Inflammatory
- Connective tissue diseases: SLE, RA, vasculitis (giant cell arteritis), adult-onset Still's disease
- Autoinflammatory syndromes: Familial Mediterranean fever, PFAPA, TRAPS
- Inflammatory bowel disease
- Sarcoidosis, IgG4 disease
Malignant
- Lymphomas (Hodgkin's - classic Pel-Ebstein fever)
- Leukemias
- Solid tumors: renal cell carcinoma, hepatocellular carcinoma, colon, breast, pancreatic
- Atrial myxoma
Miscellaneous / Other
- Drug fever - virtually any drug can cause it, even after long-term use; commonly allopurinol, carbamazepine, phenytoin, sulfonamides, beta-lactams, vancomycin, isoniazid. Often with eosinophilia + lymphadenopathy (DRESS/DIHS)
- Pulmonary embolism / DVT (thromboembolic)
- Adrenal insufficiency
- Factitious / fraudulent fever
- Hematoma resorption
- Post-surgical (5 W's: Wind, Water, Wound, Walking, Wonder drugs - i.e., drugs)
4. Clinical Approach
History - Key Points
| Domain | What to Ask |
|---|---|
| Fever pattern | Duration, onset, periodicity (quotidian, tertian, quartan, Pel-Ebstein), associated rigors/sweats |
| Localizing symptoms | Cough, dysuria, headache, stiff neck, diarrhea, joint pain, rash, sore throat |
| Epidemiology | Travel history, animal/zoonotic exposure, sexual history, IV drug use, sick contacts |
| Medical history | Recent procedures, dental work, indwelling catheters/prosthetics, recent antibiotics, prior infections |
| Medications | All drugs (including recent additions), immunosuppressants |
| Social history | Occupation, recreational activities, dietary habits (unpasteurized dairy, raw meat) |
| Immune status | HIV status, diabetes, malignancy, transplant, splenectomy |
Key patterns to recognize:
- Pel-Ebstein fever (cyclic weeks of fever then afebrile) - Hodgkin's lymphoma
- Tertian fever (48-hr cycle) - P. vivax/P. ovale malaria
- Quartan fever (72-hr cycle) - P. malariae malaria
- Fever + rigors - bacteremia, malaria, pyelonephritis
- Fever without tachycardia (relative bradycardia) - typhoid, Legionella, brucellosis, drug fever, factitious fever
- Night sweats - TB, lymphoma, HIV, brucellosis
Physical Examination
- Vital signs: temperature, HR, BP, RR, SpO2, weight loss
- General: toxicity, altered consciousness, rash distribution
- Skin/mucous membranes: rash (macular, petechial, pustular, eschar), jaundice, pallor
- Eyes: conjunctival petechiae, Roth spots (endocarditis), papilledema, fundoscopy for retinal vasculitis
- Lymph nodes: generalized vs. regional; size, tenderness, consistency
- ENT: pharyngitis, sinuses, otitis, oral ulcers
- Respiratory: consolidation, effusion
- CVS: new murmur (endocarditis), pericardial rub
- Abdomen: hepatosplenomegaly, tenderness, masses, peritonism
- Genitourinary: CVA tenderness, prostate, pelvic exam
- Neurological: meningism (neck stiffness, Kernig's, Brudzinski's)
- Joints: arthritis
- Extremities: Osler's nodes, Janeway lesions, clubbing, splinter hemorrhages
5. Investigations
Mandatory First-Line
| Test | Rationale |
|---|---|
| CBC with differential | Neutrophilia (bacterial), lymphocytosis (viral), eosinophilia (parasitic/drug), pancytopenia |
| ESR, CRP | Markers of inflammation |
| LFTs, RFTs, electrolytes | Organ involvement, baseline |
| Blood cultures × 3 (before antibiotics) | Bacteremia, sepsis, endocarditis |
| Urine R/M + culture | UTI, pyelonephritis |
| Chest X-ray | Pneumonia, TB, malignancy |
| Peripheral blood smear | Malaria, hemolytic anemia |
| Malaria antigen/PCR | If travel history or endemic area |
Second-Line (Directed by Clinical Findings)
- Serology: Widal (typhoid), Weil-Felix, VDRL, HIV, EBV/CMV, Brucella, Coxiella, Bartonella
- Imaging: Ultrasound abdomen (abscess, hepatosplenomegaly), CT (occult abscess, lymphoma), Echo (endocarditis)
- Lumbar puncture: meningism, unexplained encephalopathy
- TST / IGRA: suspected TB
- Bone marrow biopsy: fever + pancytopenia, suspected hematologic malignancy
- ANA, RF, ANCA, complement levels: if autoimmune suspected
- Ferritin (very high): Adult Still's disease, hemophagocytic lymphohistiocytosis (HLH)
- Procalcitonin: helpful in differentiating bacterial from non-bacterial
6. Fever of Unknown Origin (FUO)
Classic FUO Definition (Harrison's 22E, 2025):
- Fever ≥38.3°C on at least two occasions
- Illness duration ≥3 weeks
- No known immunocompromised state
- Diagnosis uncertain after thorough history, examination, and obligatory basic workup
Modern modification: 3 days of inpatient investigation OR 3 outpatient visits
FUO Categories and Prevalence (Modern Industrialized World):
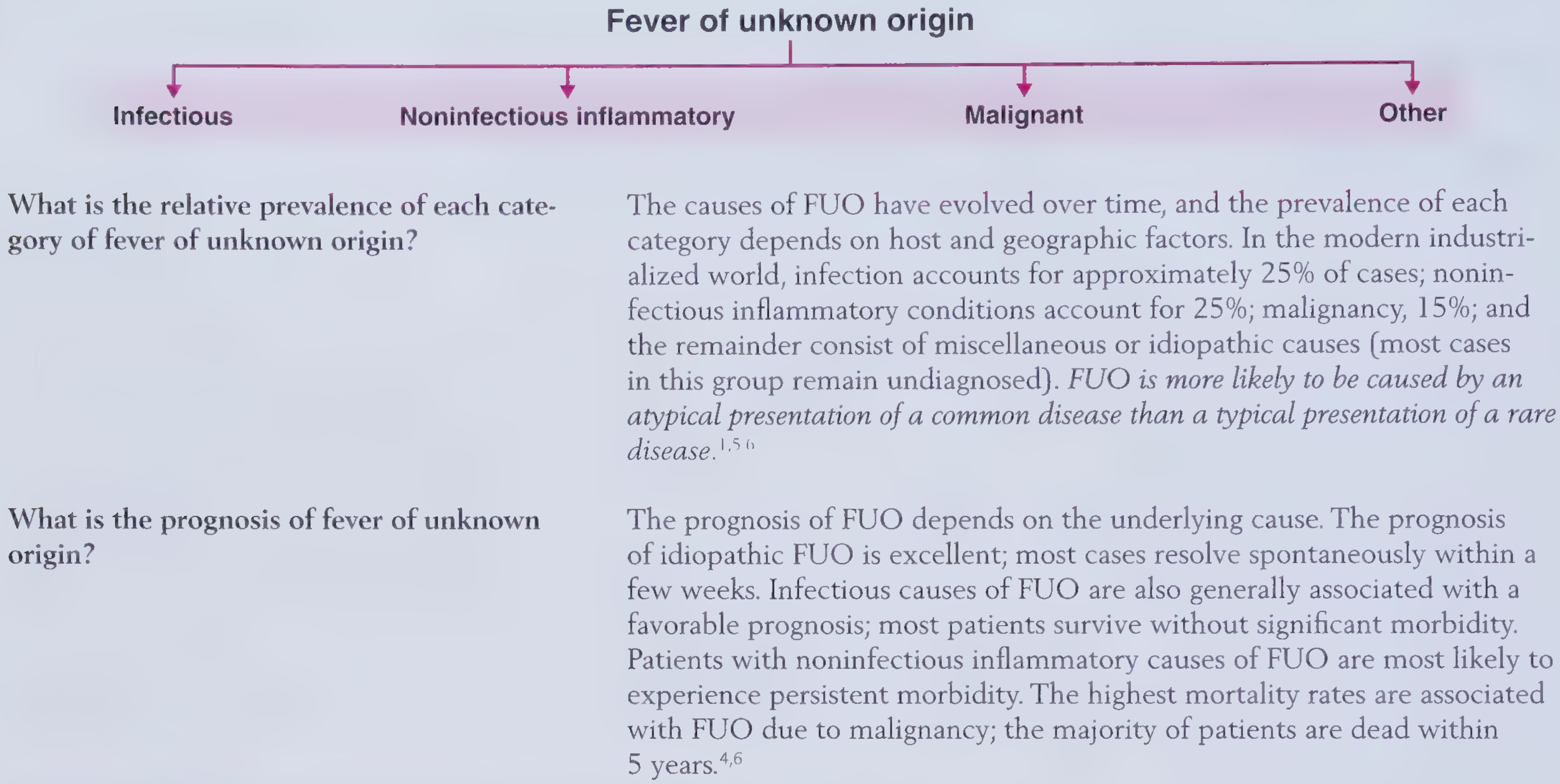
Key principle: FUO is more likely to be an atypical presentation of a common disease than a typical presentation of a rare disease.
FUO Workup Approach (Potentially Diagnostic Clues - PDCs):
- Repeat history - search for PDCs (pets, travel, occupational exposures, drug history)
- Repeat physical exam - daily exam for new signs
- Obligatory panel: CBC, ESR, CRP, ferritin, LFTs, RFTs, ANA, RF, SPEP, blood cultures × 3, urine culture, CXR, abdominal ultrasound, TST/IGRA
- PDC-directed testing - echo if murmur, MRI spine if back pain, temporal artery biopsy if elderly + high ESR, etc.
- 18F-FDG-PET/CT: when PDC-guided tests non-diagnostic; highly sensitive for occult infection, malignancy, vasculitis - best performed when ESR/CRP is elevated
- Tissue biopsy: liver, bone marrow, lymph node - especially if granulomatous disease suspected
Source: Harrison's Principles of Internal Medicine 22E; Frameworks for Internal Medicine; Goldman-Cecil Medicine
7. Special Considerations
Fever in the Immunocompromised Host
- Signs of inflammation including fever, pain, and erythema may be absent or blunted
- Consider a wider differential including opportunistic organisms
- Risk depends on specific defect:
- Neutropenia (chemotherapy): gram-negative bacteremia, invasive fungi, HSV
- T-cell defects (HIV, post-transplant): PCP, CMV, Toxoplasma, Cryptococcus, NTM, TB
- Splenectomy: encapsulated organisms (Streptococcus pneumoniae, H. influenzae, Meningococcus)
- Anti-TNF therapy: intracellular pathogens (TB, Histoplasma)
Fever in Surgery / Hospital Setting (Postoperative Fever - "5 W's")
| Time Postop | Cause |
|---|---|
| Days 1-2 | Wind - atelectasis, aspiration pneumonia |
| Day 3-5 | Water - UTI (catheter-related) |
| Day 5-7 | Wound - surgical site infection |
| Day 5+ | Walking - DVT/PE (thromboembolism) |
| Anytime | Wonder drugs - drug fever, C. diff (antibiotics) |
8. Management
Antipyretic Treatment
- Paracetamol (acetaminophen): first-line, inhibits prostaglandin synthesis centrally; dose 500mg-1g every 4-6 hours
- NSAIDs (ibuprofen, naproxen): effective antipyretics/anti-inflammatories; avoid in renal impairment, bleeding risk, dengue
- Aspirin: effective but avoid in children (Reye's syndrome) and dengue
- Physical cooling (sponging, cooling blankets): adjunct for very high temperatures
Empirical Antibiotics
- Should NOT be started blindly except in hemodynamically unstable patients or suspected meningitis
- Blood cultures must be drawn before starting antibiotics
- Early, appropriate antibiotics improve outcomes in bacteremia and sepsis
- Empirical therapy guided by the most likely source and local resistance patterns
Treating Underlying Cause
Fever itself is often beneficial (enhanced immune function) and does not always need suppression. Treat the underlying cause; symptomatic antipyretics for patient comfort and to prevent febrile seizures in children.
Key Clinical Pearls:
- Absence of fever does not exclude serious infection (especially in the elderly, uremic, or on steroids)
- Relative bradycardia (pulse-temperature dissociation) suggests typhoid, Legionella, brucellosis, or drug fever
- Very high ferritin (>10,000 µg/L) points toward HLH or Adult Still's disease
- A diagnosis of FUO is more often an atypical common disease than a rare exotic one
- Do not start antibiotics in stable FUO - the "therapeutic trial" approach delays diagnosis and confounds culture results
Sources: Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E; Guyton and Hall Textbook of Medical Physiology; Frameworks for Internal Medicine; Bailey and Love's Short Practice of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.