Hepatic encephalopathy
Reading File
Finding Sources
Searching PubMed
"hepatic encephalopathy"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, detailed content from multiple authoritative sources. Let me compile the full answer.
Hepatic Encephalopathy (HE)
Definition
Hepatic encephalopathy encompasses a wide array of transient, reversible neurologic and psychiatric manifestations seen in patients with chronic liver disease and portal hypertension, and also in acute liver failure (ALF). It develops in 50-70% of patients with cirrhosis, and its occurrence is a poor prognostic indicator - projected 1-year survival is ~42% and 3-year survival ~23% without liver transplantation (LT).
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1815
Classification
HE is classified by 4 factors: underlying disease, severity, time course, and precipitating factors.
By Underlying Disease (EASL/AASLD Types)
| Type | Underlying Cause |
|---|---|
| Type A | Acute liver failure (ALF) |
| Type B | Portosystemic bypass/shunts without hepatocellular disease |
| Type C | Cirrhosis with portal hypertension (most common) |
Severity: West Haven Criteria + SONIC Classification
| West Haven Grade | Intellectual Function | Neuromuscular | SONIC Category |
|---|---|---|---|
| 0 | Normal | Normal | Unimpaired |
| Minimal | Subtle changes in work/driving | Minor visual-perception abnormalities | Covert HE |
| 1 | Trivial lack of awareness, euphoria/anxiety, shortened attention; impaired add/subtract | Minor abnormalities | Covert HE |
| 2 | Lethargy, disorientation to time, personality change | Asterixis | Overt HE |
| 3 | Somnolence/semistupor, responsiveness to verbal stimuli, gross disorientation | Asterixis | Overt HE |
| 4 | Coma | No asterixis | Overt HE |
Covert HE (grade 0-minimal-1) affects approximately half of all patients with cirrhosis but is commonly overlooked because it does not drive patients to seek medical care. It still negatively impacts quality of life, driving ability, and workplace performance.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1781
Pathophysiology
The diagram below from Sleisenger & Fordtran summarizes the key mechanisms:
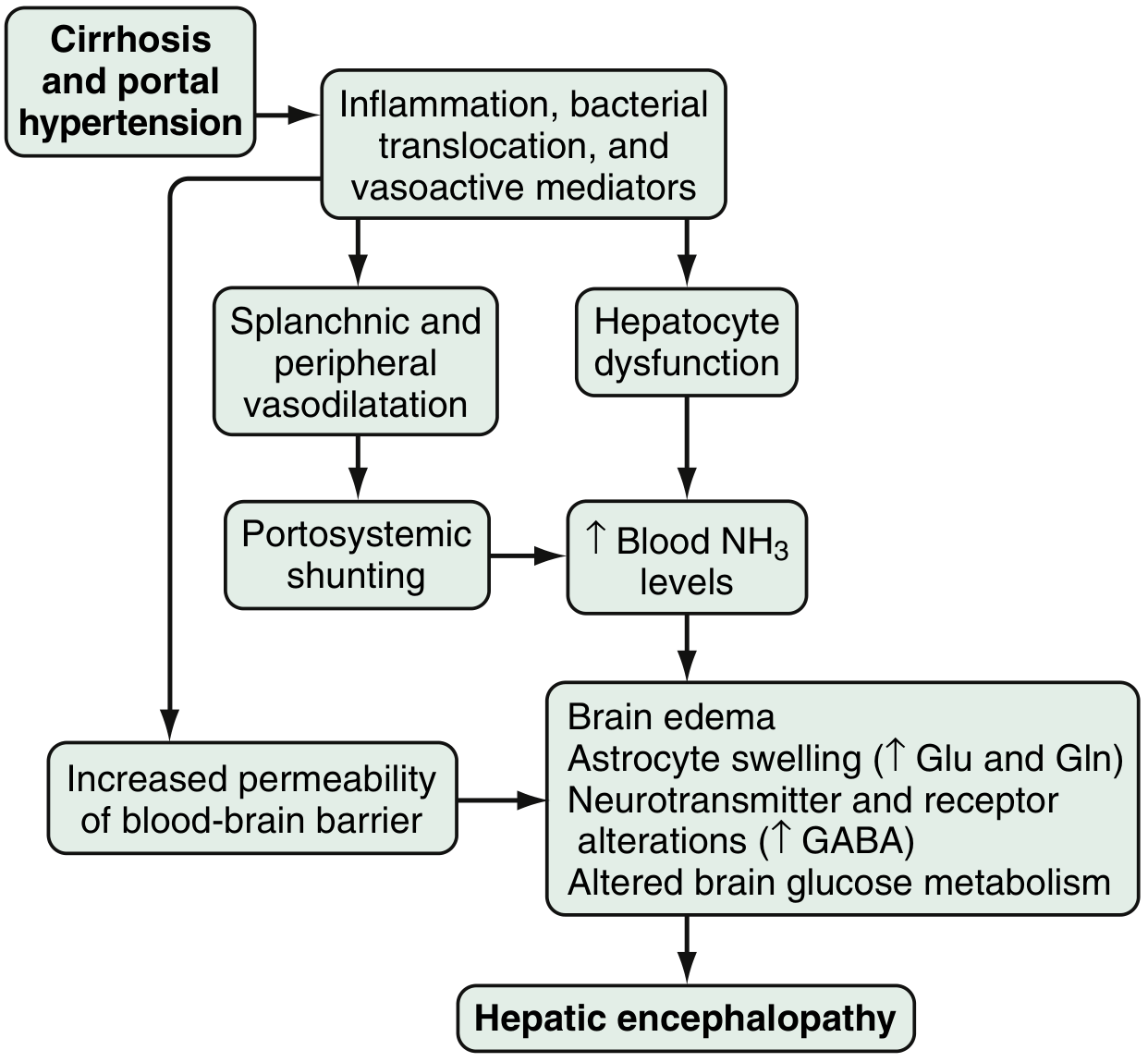
1. Ammonia - The Central Neurotoxin
- Source: Colon bacteria metabolize proteins/nitrogenous products → ammonia; enterocytes synthesize ammonia from glutamine
- Ammonia enters the portal circulation and is normally cleared by hepatocytes
- In cirrhosis: reduced hepatocyte function + portosystemic shunting → arterial hyperammonemia (seen in up to 90% of HE patients)
- Ammonia crosses the blood-brain barrier (increased permeability): preferentially taken up by the cerebellum and basal ganglia
- Effects on the brain: astrocyte swelling, cytotoxic brain edema, impaired transport of neuroactive compounds (e.g., myoinositol), direct inflammatory response in astrocytes
- Astrocytes respond by converting glutamate → glutamine (via glutamine synthetase) → osmotic astrocyte swelling
2. GABA-Benzodiazepine System
- Increased sensitivity of astrocyte peripheral-type benzodiazepine receptors enhances activation of the GABA-A/benzodiazepine system
- A feed-forward loop: astrocytes produce neurosteroids (allopregnanolone, tetrahydrodeoxycorticosterone) → further activates GABA-A receptors → net CNS inhibition
- This explains why benzodiazepines can precipitate/worsen HE
3. Other Factors
-
Manganese deposition: accumulates in basal ganglia (especially globus pallidus) → dopaminergic dysfunction; produces characteristic T1-hyperintensity on MRI
-
Altered amino acid profile: increased aromatic amino acids (false neurotransmitters), decreased branched-chain amino acids
-
Inflammatory mediators: systemic inflammation (from bacterial translocation, infections) synergizes with hyperammonemia
-
Nitric oxide, serotonin, short-chain fatty acids, mercaptans: additional contributing neurotoxins
-
Gut microbiome: differences in colonic mucosal microbiota between cirrhotic patients with and without HE
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1815-1816
Precipitating Factors
Approximately 25% of HE episodes are precipitated by sedative drugs; other common triggers (in descending frequency):
| Precipitant | Approximate Contribution |
|---|---|
| Sedatives/benzodiazepines | ~25% |
| GI hemorrhage | ~18% |
| Drug-induced azotemia | ~15% |
| Other azotemia (dehydration, renal failure) | ~15% |
| Excessive dietary protein | ~10% |
| Hypokalemia, constipation, infections | Remainder |
Additional precipitants: TIPS placement (transjugular intrahepatic portosystemic shunt) - predisposes to HE especially in elderly patients.
- Bradley and Daroff's Neurology in Clinical Practice, p. 1781
Clinical Features
Presentation spans a continuum from imperceptible changes to deep coma:
- Early/covert: forgetfulness, alterations in handwriting, difficulty driving, sleep-wake cycle reversal
- Overt: asterixis (flapping tremor), agitation, disinhibited behavior, disorientation, confusion
- Severe: somnolence, stupor, coma, seizures
Asterixis ("liver flap") - graded 0-4 (0 = absent, 4 = almost continuous flapping tremors). It is not specific to HE but is a hallmark sign.
Key distinction from ALF-related encephalopathy:
- ALF: mania evolving to deep coma, nausea/vomiting common, abdominal pain common
- Chronic HE (portal-systemic): blunted consciousness, onset may be insidious, rarely presents with N/V or abdominal pain
Diagnosis
No single test definitively confirms HE - it is a clinical diagnosis of exclusion.
Blood Tests
- Serum ammonia: elevated in up to 90% of HE, but neither sensitive nor specific - normal ammonia does NOT exclude HE; elevated ammonia does not confirm it
- Standard LFTs (bilirubin, enzymes, albumin, INR) are usually abnormal
- Arterial ammonia offers no advantage over venous in chronic liver disease
Neuropsychometric Tests
- Stroop test (psychomotor speed, cognitive flexibility) - validated for HE; available as a smartphone app (EncephalApp)
- Portosystemic Encephalopathy Syndrome Test
- These are especially useful for detecting covert/minimal HE
EEG
- Characteristic: bursts of moderate-to-high amplitude (100-300 μV), low-frequency (1.5-2.5 Hz) waves with frontal predominance in severe HE
- Even patients without clinical signs may show reduced mean dominant frequency
MRI / MR Spectroscopy
- T1-weighted MRI: bilateral T1-hyperintensity in the globus pallidus (from manganese deposition) - regression occurs after successful LT
- MR Spectroscopy: increased glutamine/glutamate peak (Glx) at ~2.5 ppm; decreased myoinositol and choline signals; N-acetylaspartate (neuronal marker) remains normal
- MRI is useful to exclude structural causes (subdural hematoma, Wernicke's, cerebellar atrophy)
Critical Flicker Frequency (CFF)
- Assesses cerebral cortex function; reliable marker of minimal HE
Important: None of these findings are specific for HE. Diagnosis requires exclusion of other causes of cerebral dysfunction (hypoglycemia, hyponatremia, medication ingestion, intracranial hemorrhage especially if focal deficits present).
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1816; Bradley and Daroff's Neurology, p. 1782
Treatment
Step 1: Identify and Correct Precipitating Factors
This is the first and most important step - treat GI bleeding, infections (including SBP), electrolyte abnormalities (especially hypokalemia), discontinue sedatives, correct dehydration/azotemia.
Step 2: Reduce Ammonia Production/Absorption
Lactulose (nonabsorbable disaccharide)
- First-line treatment - cornerstone of HE management
- Dose: 30-60 g/day orally; titrate to 2-3 soft stools/day
- Mechanism: metabolized by colonic bacteria → acidic byproducts → catharsis + reduced intestinal pH → inhibits NH₃ absorption (NH₃ → NH₄⁺, which is not absorbed)
- Can be given per rectum (enema) in patients at aspiration risk
- Side effects: abdominal cramping, flatulence, diarrhea, electrolyte imbalance
Rifaximin
- Non-absorbable antibiotic targeting gut flora
- 400 mg PO every 8 hours (or 550 mg twice daily for secondary prophylaxis)
- Used alone or (preferably) in combination with lactulose for overt HE and prevention of recurrence
- Superior to other antibiotics; used in the pivotal trial that led to its FDA approval for HE
- Side effects minimal given negligible systemic absorption
Other antibiotics (neomycin, metronidazole): historically used but largely replaced by rifaximin due to better safety profile.
Step 3: Nutritional Management
- Do NOT restrict protein - previous practice of protein restriction is not beneficial and may worsen sarcopenia (which itself is a risk factor for HE)
- Vegetable and dairy proteins preferred over animal proteins (more favorable calorie-to-nitrogen ratio)
- Branched-chain amino acid (BCAA) supplementation: shown to have beneficial effect on HE and reduces hospitalizations; does not affect mortality or quality of life (oral BCAAs); IV BCAAs show benefit without increased mortality
- Small, frequent meals; avoid prolonged fasting
Additional Therapies
- Zinc supplementation: zinc deficiency is common in cirrhosis; supplementation may improve HE
- Probiotics/prebiotics: modulate gut microbiome; emerging evidence for secondary prophylaxis
- TIPS management: if TIPS-related HE, TIPS embolization with coils to reduce shunted volume in refractory cases
Definitive Treatment
-
Liver transplantation (LT): the only definitive treatment; generally reverses HE
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1817; Rosen's Emergency Medicine, p. 1235
Prognosis
- Development of HE indicates advanced cirrhosis and poor prognosis
- Cumulative 1-year survival: 20-42%; 3-year survival: 15-23% without LT
- Minimal/covert HE affects ~50% of all cirrhotic patients and impairs driving, quality of life, and work performance - it increases risk of progression to overt HE
- About 20,000 patients per year are hospitalized in the US for HE (2005-2009 data)
Summary Table: Key Management Points
| Aspect | Key Points |
|---|---|
| First step | Identify & treat precipitant |
| Ammonia reduction | Lactulose (1st line) + Rifaximin (add-on or prophylaxis) |
| Diet | No protein restriction; prefer vegetable/dairy protein; BCAAs |
| Monitoring | Target 2-3 soft stools/day on lactulose |
| Covert HE | Screen all cirrhotic patients; EncephalApp (Stroop) |
| TIPS-related HE | Usually responds to conventional Rx; refractory → coil embolization |
| Definitive | Liver transplantation |
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Ch. 94); Bradley and Daroff's Neurology in Clinical Practice (Ch. 84); Rosen's Emergency Medicine; Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Recent evidence note: A 2025 meta-analysis (PMID 40812534) found that proton pump inhibitor (PPI) use is associated with increased risk of HE in cirrhotic patients - a clinically relevant consideration when managing these patients. A 2026 systematic review (PMID 41942881) assessed risk prediction models for HE in liver cirrhosis, highlighting the importance of early identification. A 2025 meta-analysis (PMID 40081810) documented that HE also occurs in non-cirrhotic portal hypertension, not just cirrhosis.
Stroke new treatment guidelines 2026
Reading File
Finding Sources
Searching PubMed
"ischemic stroke"[MeSH Terms] AND "guideline"[pt]
Searching the Web
stroke treatment guidelines 2025 2026 AHA ASA updates thrombectomy thrombolysis
Reading Web Page
https://dig.pharmacy.uic.edu/faqs/2026-2/april-2026-faqs/upd…
Reading Article
PMID: 41582814
Reading Article
PMID: 42095756
Reading Web Page
https://newsroom.heart.org/news/new-guideline-expands-stroke…
Reading Article
PMID: 41942818
Reading Article
PMID: 41249078
I now have comprehensive, detailed data from the 2026 AHA/ASA guidelines plus supporting ESO and ILEP consensus papers. Here is the full synthesized answer:
Stroke Treatment Guidelines 2026
The 2026 AHA/ASA Guideline - Overview
Published January 26, 2026 in the journal Stroke, the 2026 AHA/ASA Guideline for the Early Management of Patients With Acute Ischemic Stroke replaces the 2018 guideline and its 2019 update. It is the most comprehensive revision in nearly a decade and synthesizes evidence from landmark trials published through early 2025. The guideline covers prehospital evaluation, acute reperfusion therapy, in-hospital management, and early secondary prevention.
Stroke remains the #4 leading cause of death in the US, affecting ~800,000 people annually.
Key Updates at a Glance
| Area | What Changed |
|---|---|
| IV Thrombolysis - drug choice | Tenecteplase now co-endorsed equally with alteplase |
| IV Thrombolysis - time window | Extended beyond 4.5 hrs in select patients with advanced imaging |
| Endovascular thrombectomy (EVT) | Expanded eligibility: up to 24 hrs, large cores, posterior circulation |
| Blood pressure post-IVT | Aggressive SBP <140 mmHg after IVT NOT recommended |
| Glycemic management | Less aggressive; intensive glucose control not recommended |
| Pediatric stroke | First-ever dedicated AIS recommendations for children |
| Mobile stroke units | Formally endorsed for pre-hospital care |
| Dysphagia | Updated screening and management guidance |
| Secondary prevention | Expanded antiplatelet and lipid management recommendations |
1. Intravenous Thrombolysis (IVT)
Drug Choice: Tenecteplase is Now Equal to Alteplase
The 2026 guideline co-endorses tenecteplase as a first-line agent for IVT, no longer just an "alternative" to alteplase. Both are recommended equally for eligible patients presenting within 4.5 hours.
| Drug | Dose | Administration |
|---|---|---|
| Tenecteplase | 0.25 mg/kg IV (max 25 mg) | Single IV bolus push |
| Alteplase | 0.9 mg/kg IV (max 90 mg) | 10% as bolus, remainder over 60 min |
Tenecteplase's practical advantage: a single bolus with no infusion, reducing dosing complexity in time-critical settings. Multiple large RCTs (including TRACE-3 and others) support this change.
Extended Time Window for IVT (New)
The standard 4.5-hour window remains, but IVT is now reasonable in two additional scenarios identified on advanced imaging (perfusion CT or MRI):
- Patients who awaken with stroke within 9 hours from the midpoint of sleep (wake-up stroke)
- Patients 4.5 to 9 hours from last known well with evidence of salvageable ischemic penumbra on advanced imaging
This is based on the EXTEND and TRACE-3 trials demonstrating benefit beyond 4.5 hours in carefully selected patients with penumbral tissue.
Modified Contraindications
The approach to IVT contraindications has been revised - some previously absolute contraindications have been updated based on newer evidence.
2. Endovascular Thrombectomy (EVT / Mechanical Thrombectomy)
Expanded Eligibility (Major Update)
EVT eligibility has been significantly broadened:
- Time window: Up to 24 hours from symptom onset (or last known well) when advanced imaging (CT perfusion/MRI) demonstrates salvageable brain tissue - previously 16-24 hours was only for selected patients
- Large infarct cores: Selected patients with larger established infarcts may now be eligible based on imaging criteria (reflecting ASPECTS score data and DEFUSE/DAWN trial concepts extended)
- Posterior circulation strokes: New evidence incorporated supporting EVT for basilar artery occlusion and other posterior circulation LVO
- Bridging therapy: Patients eligible for both IVT and EVT should receive both sequentially without delaying EVT for the IVT infusion to complete
3. Blood Pressure Management
Before IVT
- BP must be < 185/110 mmHg before initiating IVT (unchanged)
- Maintain < 180/105 mmHg during and for 24 hours after IVT
After IVT - New Recommendation
- Intensive SBP lowering to < 140 mmHg in the first 24 hours after IVT is NOT recommended - it has not been associated with improved functional outcomes and may be harmful
- This is a change from prior practice that sometimes pushed for aggressive BP lowering post-thrombolysis
After Successful EVT (ESO 2026 Update)
The 2025/2026 ESO guideline update on BP management (published May 2026) aligns with the AHA/ASA:
- Against intensive SBP < 140 mmHg in the first 24 hours after successful mechanical thrombectomy (high-certainty evidence)
- Routine pre-hospital BP lowering in suspected stroke: not advised (moderate-certainty evidence)
In Intracerebral Hemorrhage (ICH)
- Early SBP reduction to < 140 mmHg supported in patients with small-to-moderate hematomas to limit expansion (expert consensus; net benefit remains uncertain for all ICH)
4. Glycemic (Blood Sugar) Management
- Less aggressive glycemic control is now endorsed for patients with persistent hyperglycemia after AIS
- Intensive insulin therapy targeting tight glucose control is not recommended - evidence shows no benefit and potential for hypoglycemic harm
- A reasonable target is generally treating significant hyperglycemia (e.g., glucose > 180 mg/dL) without pursuing intensive normalization
5. Pediatric Acute Ischemic Stroke - First-Ever Dedicated Recommendations
This is one of the most significant additions to the 2026 guideline. For the first time, the AHA/ASA provides specific guidance for stroke in children, covering:
- Age-appropriate diagnostic criteria and imaging
- Eligibility criteria for IVT and EVT in the pediatric population
- Pediatric-specific dosing considerations
- Recognition that children have different stroke etiologies (e.g., cardiac, hematologic) than adults
6. Prehospital Care and Systems of Care
- Mobile Stroke Units (MSUs): Formally endorsed - vehicles equipped with CT scanners and telemedicine capability that allow diagnosis and IVT administration before hospital arrival, shown to significantly reduce time-to-treatment and long-term disability
- EMS triage refinement: Improved protocols for bypassing closer non-thrombectomy-capable hospitals to go directly to comprehensive stroke centers (CSCs) for patients with suspected LVO
- Telestroke: Continued strong endorsement for rural/underserved areas
7. Secondary Prevention Updates
Antiplatelet Therapy
- Dual antiplatelet therapy (DAPT) with aspirin + clopidogrel or aspirin + ticagrelor for 21 days is endorsed for non-disabling minor ischemic stroke or high-risk TIA (POINT/CHANCE trial data), then transition to single antiplatelet
- For patients within the 4.5-hour window with minor stroke, DAPT without thrombolysis is an option
Lipid Management (ILEP 2026 Consensus)
The ILEP 2026 Lipid Consensus Paper provides updated guidance:
- LDL-C contributes to ~1/3 of all ischemic strokes
- Up to 40% of post-stroke patients receive no lipid-lowering therapy - a major gap
- Intensive upfront combination LLT (statin + ezetimibe ± PCSK9 inhibitor) recommended for secondary stroke prevention
- LDL-C target for secondary prevention: < 55 mg/dL (< 1.4 mmol/L)
- Early and aggressive treatment emphasized to prevent recurrence (40% recurrence risk within 5 years without adequate LLT)
Atrial Fibrillation Detection
- Prolonged cardiac monitoring (≥ 72 hours, preferably long-term implantable loop recorder) recommended after cryptogenic stroke to detect paroxysmal AF
Patent Foramen Ovale (PFO)
ESO 2024 PFO guideline: PFO closure is recommended in selected patients aged < 60 with cryptogenic stroke and high-risk PFO features (large shunt, atrial septal aneurysm).
8. Dysphagia Management
- Formal swallowing screen before any oral intake is strongly recommended for all AIS patients
- Early speech therapy involvement for aspiration prevention
- The 2026 neuroprognostication guidelines (PMID 41942818) include recovery of swallow function as a prognostically important parameter in critically ill stroke patients
9. Neuroprognostication in Critically Ill AIS (New 2026 Guidelines)
A separate 2026 guideline (PMID 41942818) addresses ICU-level stroke patients:
- Avoid premature neuroprognostication - a key good-practice statement
- Early neurological improvement within 24 hours of revascularization is a moderately reliable predictor of good functional outcome
- No single clinical variable reliably predicts poor outcome - multimodal assessment is required
- Special guidance for counseling families of patients with large hemispheric infarction before neurological decline
Summary: What's Most Clinically Impactful
- Tenecteplase is now a first-line choice - simplifies delivery, equivalent efficacy to alteplase
- Extended IVT window to 9 hours in wake-up/late-window strokes with penumbral imaging - more patients eligible
- EVT up to 24 hours with imaging selection - significantly more patients eligible for clot removal
- Posterior circulation and large cores are no longer automatic exclusions from EVT
- Don't aggressively lower BP post-IVT (< 140 mmHg target abandoned)
- Mobile stroke units endorsed as a system-of-care standard
- First pediatric AIS guidelines - a long-awaited addition
- DAPT for 21 days in minor stroke/high-risk TIA remains strong evidence-based practice
Primary Source: 2026 AHA/ASA Guideline for Early Management of AIS - Prabhakaran S et al., Stroke, January 26, 2026. DOI: 10.1161/STR.0000000000000513
Supporting sources: ESO 2026 BP guideline | ILEP Lipid Consensus 2026 | Neuroprognostication 2026 | ESO PFO 2024
This is a shared conversation. Sign in to Orris to start your own chat.