Heart failure, definition,types, pathophysiology,clinical features,diagnosis, management
Reading File
Finding Sources
Searching PubMed
"heart failure" management guidelines
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Searching Images
heart failure pathophysiology neurohormonal activation RAAS sympathetic
Loading Image
I now have all the information needed to write a comprehensive, well-structured answer on heart failure. Let me compile the full response.
Heart Failure — Comprehensive Overview
1. Definition
Heart failure (HF) is a clinical syndrome resulting from the inability of the heart to meet the metabolic requirements of the body at normal filling pressures. It is characterized by symptoms (dyspnea, fatigue, fluid retention) caused by a structural or functional cardiac abnormality. Importantly, pulmonary congestion may be absent — hence the preferred term "heart failure" over the older "congestive heart failure."
— Textbook of Family Medicine 9e
2. Types / Classification
A. By Ejection Fraction
| Type | EF | Mechanism |
|---|---|---|
| HFrEF (Heart Failure with Reduced EF) | < 40–45% | Impaired LV systolic contraction |
| HFmrEF (mid-range EF) | 40–49% | Mixed systolic/diastolic features |
| HFpEF (Heart Failure with Preserved EF) | ≥ 50% | Impaired LV filling/relaxation (diastolic dysfunction) |
HFpEF and HFrEF are nearly equally prevalent. HFpEF is characterized by increased LV stiffness, impaired relaxation, and elevated filling pressures with preserved contractile function.
B. By Side of Failure
- Left-sided HF: Causes pulmonary congestion → dyspnea, orthopnea, paroxysmal nocturnal dyspnea (PND), pink frothy sputum
- Right-sided HF: Causes systemic venous congestion → JVD, peripheral edema, hepatomegaly, ascites
- Biventricular HF: Both ventricles fail; most chronic HF is ultimately biventricular
C. By Onset
- Acute HF: Rapid onset (e.g., acute MI, flash pulmonary edema)
- Chronic HF: Gradual, compensated or decompensated
D. By Output
- Low-output HF: Most common; reduced cardiac output (IHD, cardiomyopathy, valvular disease)
- High-output HF: Paradoxically high CO (>4 L/min/m²) but still cannot meet demands — causes include hyperthyroidism, beriberi, severe anemia, Paget's disease, arteriovenous malformations, multiple myeloma
E. ACC/AHA Staging (complements NYHA)
| Stage | Description | NYHA Equivalent |
|---|---|---|
| A | At-risk; no LV dysfunction, no symptoms | — |
| B | LV dysfunction; asymptomatic | Class I |
| C | LV dysfunction; symptomatic on exertion | Class II–III |
| D | Refractory HF; symptoms at rest despite maximal therapy | Class IV |
F. NYHA Functional Classification
| Class | Symptoms |
|---|---|
| I | No limitation of physical activity |
| II | Slight limitation — comfortable at rest, symptoms with ordinary activity |
| III | Marked limitation — comfortable at rest, symptoms with less-than-ordinary activity |
| IV | Unable to carry out any activity without symptoms; symptoms at rest |
3. Pathophysiology
Primary Mechanism — LV Remodeling
The old hemodynamic model has been replaced by the neurohormonal/LV remodeling model. An initial cardiac injury (MI, hypertension, valvular disease, etc.) triggers LV stretching and dilation → reduced LV function. Remodeling is reversible with appropriate therapy.
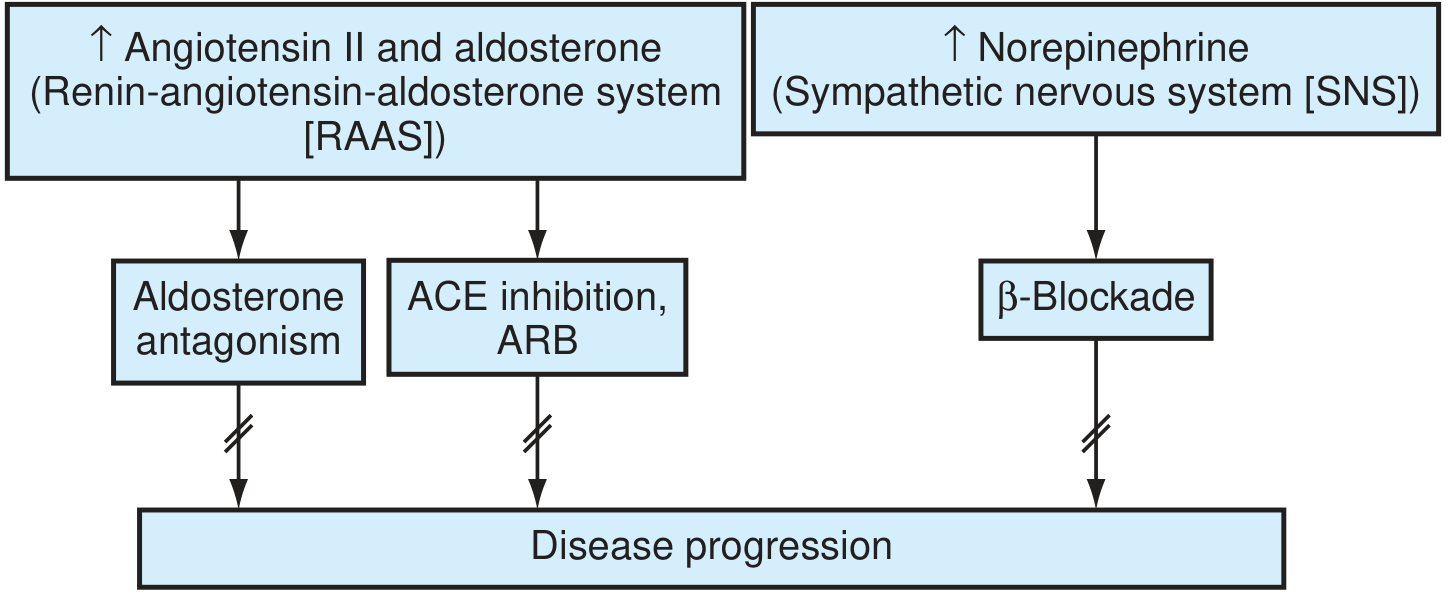
Neurohormonal Activation
Two key systems are activated:
1. Renin-Angiotensin-Aldosterone System (RAAS)
- Angiotensin II → cardiac myocyte apoptosis, hypertrophy, ventricular fibrosis
- Angiotensin II → ↑ aldosterone → further adverse remodeling, Na⁺/water retention
- Aldosterone "escapes" ACE inhibitor suppression → need for selective aldosterone blockade
2. Sympathetic Nervous System (SNS)
- ↑ Circulating catecholamines → β-adrenoceptor downregulation
- Catecholamines → cAMP-dependent Ca²⁺ overload of myocytes → direct toxicity
- ↑ Myocardial O₂ consumption, LVH, potentially fatal arrhythmias
Additional mediators:
- ↑ Endothelin-1 (from dysfunctional endothelium) → vasoconstriction
- ↑ Inflammatory cytokines → exacerbate endothelial dysfunction
- ↑ MMPs and tissue inhibitors → cardiac fibrosis and collagen deposition
- Altered Ca²⁺ fluxes, β-adrenergic receptor changes, metabolic shift to glycolysis
Compensatory Mechanisms (and their limits)
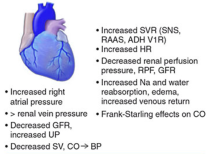
| Compensation | Mechanism | Long-term Effect |
|---|---|---|
| Frank-Starling | ↑ Preload → ↑ stroke volume | Leads to ventricular dilation |
| Tachycardia | SNS activation | ↑ O₂ demand, arrhythmias |
| Vasoconstriction | ↑ SVR via RAAS/SNS/ADH | ↑ Afterload, ↑ cardiac work |
| Na⁺/H₂O retention | RAAS + ADH | Edema, pulmonary congestion |
| Ventricular hypertrophy | Pressure/volume overload | Diastolic dysfunction, fibrosis |
4. Clinical Features
Symptoms
| Left HF | Right HF |
|---|---|
| Dyspnea on exertion | Peripheral edema (pitting, bilateral) |
| Orthopnea (need ≥2 pillows) | Weight gain |
| Paroxysmal nocturnal dyspnea | Abdominal distension/discomfort |
| Nocturnal cough | Anorexia, nausea (bowel edema) |
| Fatigue, reduced exercise tolerance | Fatigue |
| Cardiac wheeze ("cardiac asthma") | — |
Signs
General: Tachycardia, pallor, cyanosis, cachexia (in advanced HF)
Cardiovascular:
- Displaced, heaving apex beat (LV dilatation)
- S3 gallop (pathological — indicates volume overload/poor systolic function)
- S4 gallop (indicates non-compliant LV — diastolic dysfunction)
- Murmurs (mitral regurgitation from annular dilation)
- Pulsus alternans (severe LV dysfunction)
Respiratory:
- Bibasal crepitations (pulmonary edema)
- Dullness to percussion at lung bases (pleural effusion)
- Cheyne-Stokes respiration (in severe HF, low cardiac output to brain)
Venous/Systemic:
- Raised JVP
- Hepatojugular reflux
- Pitting pedal/ankle edema → sacral edema (in bedbound)
- Hepatomegaly (tender in acute RHF)
- Ascites (chronic RHF)
Framingham Criteria for HF Diagnosis
Major criteria: PND, neck vein distension, rales, cardiomegaly on CXR, acute pulmonary edema, S3 gallop, ↑ CVP, hepatojugular reflux.
Minor criteria: Bilateral ankle edema, nocturnal cough, dyspnea on exertion, hepatomegaly, pleural effusion, ↓ vital capacity by 1/3, tachycardia (HR >120).
Diagnosis requires 2 major or 1 major + 2 minor criteria.
5. Diagnosis
Investigations
ECG:
- May show LVH, LBBB, AF, prior MI (Q waves), or be non-specific
- Wide QRS (>120 ms) — indicates dyssynchrony, relevant for CRT candidacy
Chest X-Ray (CXR) — classic ABCDE features:
- Alveolar edema ("bat-wing" perihilar shadowing)
- B-lines / Kerley B lines (interstitial edema)
- Cardiomegaly (cardiothoracic ratio >0.5)
- Dilated upper lobe veins (cephalization)
- Effusion (pleural — usually bilateral; if unilateral, right > left)
Echocardiography (KEY investigation):
- Confirms LV/RV size and function, wall motion, EF, valve disease, diastolic filling patterns
- Differentiates HFrEF from HFpEF
- Guides therapy (CRT, LVAD, transplant assessment)
Biomarkers:
- BNP / NT-proBNP: Elevated in HF; highly sensitive; used for diagnosis and monitoring. Elevated BNP (>100 pg/mL) or NT-proBNP (>300 pg/mL) strongly supports HF; levels >400 pg/mL indicate more severe disease
- Troponin: Elevated in acute decompensation or ischemic etiology
- Renal function / electrolytes: Creatinine, eGFR, K⁺ (critical for drug dosing)
- Liver function: ALT, AST, bilirubin (hepatic congestion in RHF)
- CBC: Anemia (precipitant/exacerbant); eosinophilia (eosinophilic myocarditis)
- TFTs: Hypothyroidism/hyperthyroidism as cause
Additional (selected cases):
- Cardiac MRI: Gold standard for myocardial viability, infiltrative disease, myocarditis, sarcoidosis
- Coronary angiography: If ischemic etiology suspected or revascularization planned
- Endomyocardial biopsy: For suspected giant cell myocarditis, cardiac sarcoidosis, amyloid (unexplained new HF)
- Cardiopulmonary exercise testing: Objective functional assessment; guides transplant listing (peak VO₂ <14 mL/kg/min = high mortality, transplant consideration)
- Sleep study: OSA/central sleep apnea — highly prevalent and can worsen HF
6. Management
General Principles / Non-Pharmacological
- Salt restriction: <2 g sodium/day
- Fluid restriction: 1.5–2 L/day in moderate-severe HF
- Daily weight monitoring: >2 kg/day rise → contact team
- Cardiac rehabilitation / supervised exercise: Improves functional capacity in stable HFrEF
- Smoking cessation, alcohol limitation (alcohol is a direct myocardial toxin)
- Vaccinations: Annual influenza; pneumococcal
- Avoid NSAIDs (Na⁺ retention, renal impairment), non-DHP CCBs (verapamil/diltiazem in HFrEF), TZDs (fluid retention)
Pharmacological Management — HFrEF (EF <40%)
The "four pillars" of HFrEF therapy (all reduce mortality):
1. ACE Inhibitors (ACEi) / ARBs
- ACEi (enalapril, ramipril, lisinopril): First-line; block Ang II formation → reduce preload, afterload, and adverse remodeling
- ARBs (valsartan, candesartan): Used if ACEi-intolerant (cough, angioedema)
- Titrate to target dose; monitor renal function and K⁺
2. Beta-Blockers (BB)
- Evidence-based agents: Carvedilol, bisoprolol, metoprolol succinate (not all β-blockers have proven mortality benefit in HF)
- Block SNS activation → ↓ catecholamine toxicity, ↓ HR, ↓ arrhythmias
- Start low, titrate slow; do not initiate in acutely decompensated HF
- CIBIS-II, MERIT-HF, COPERNICUS — landmark mortality-reducing trials
3. Mineralocorticoid Receptor Antagonists (MRA)
- Spironolactone / eplerenone: Block aldosterone's cardiac/renal effects
- Indicated for NYHA class II–IV, LVEF ≤35%
- Monitor K⁺ and creatinine closely (hyperkalemia risk)
- Post-MI with HF → eplerenone (EPHESUS trial)
4. SGLT2 Inhibitors (SGLT2i) — the "new pillar"
- Dapagliflozin / empagliflozin: Reduce HF hospitalization and cardiovascular death
- Benefit seen in both HFrEF and HFpEF
- Recent meta-analysis (PMID: 39731023) confirms safety and effectiveness in acute HF as well
5. ARNI (Angiotensin Receptor-Neprilysin Inhibitor)
- Sacubitril/valsartan (Entresto): Replaces ACEi in symptomatic HFrEF (NYHA II–III)
- Dual mechanism: ARB (blocks AT1R) + neprilysin inhibitor (↑ natriuretic peptides)
- PARADIGM-HF trial: Reduced CV death/HF hospitalization vs. enalapril
- Must washout ACEi for 36 hours before starting to avoid angioedema
6. Diuretics (symptom relief, not mortality benefit)
- Loop diuretics (furosemide, bumetanide): First-line for fluid overload; IV in acute decompensation
- Thiazides: Add-on for diuretic resistance
- Aldosterone antagonists (spironolactone): Both diuretic and prognostic benefit
7. Digoxin
- Reduces hospitalizations; no mortality benefit in HFrEF (DIG trial)
- Consider for symptomatic HFrEF in sinus rhythm refractory to other therapy, or for rate control in AF with HF
- Narrow therapeutic index; target level 0.5–0.8 ng/mL
8. Hydralazine + Isosorbide Dinitrate
- Vasodilator combination; indicated in patients intolerant of ACEi AND ARBs
- Particularly beneficial in African-American patients (A-HeFT trial)
Pharmacological Management — HFpEF (EF ≥50%)
No therapy has convincingly reduced mortality in HFpEF. Management focuses on:
- Symptom control: Diuretics for congestion
- Risk factor treatment: Hypertension (strict BP control), AF rate/rhythm control, diabetes, obesity
- SGLT2 inhibitors: Dapagliflozin (DELIVER trial) and empagliflozin (EMPEROR-Preserved) — reduced HF hospitalizations
- MRAs: Spironolactone may reduce hospitalization (TOPCAT trial, regional subgroup analysis)
Device Therapy
| Device | Indication |
|---|---|
| ICD (Implantable Cardioverter Defibrillator) | LVEF ≤35% on optimal medical therapy ≥3 months; primary prevention of sudden cardiac death |
| CRT (Cardiac Resynchronization Therapy) | LVEF ≤35%, NYHA II–IV, LBBB with QRS ≥150 ms (or ≥130 ms with LBBB) |
| CRT-D (CRT + ICD) | Both above indications combined |
| LVAD (Left Ventricular Assist Device) | Advanced HF as bridge to transplant or destination therapy |
ICD is indicated for patients with LVEF ≤35%, at least 40 days post-MI and revascularization, or 3 months after initiation of optimal medical treatment in non-ischemic patients.
Surgical / Advanced Therapies
- Coronary revascularization (CABG/PCI): When ischemia is the primary etiology and viable myocardium exists
- Valve repair/replacement: For significant mitral or aortic valve disease contributing to HF
- MitraClip: Transcatheter mitral valve repair in HFrEF with secondary MR (COAPT trial)
- Cardiac transplantation: For end-stage HF (NYHA IV), peak VO₂ <14 mL/kg/min, on optimal therapy; ~50% 10-year survival
- CPAP/BiPAP: For coexisting OSA (central sleep apnea may worsen with adaptive servo-ventilation — SERVE-HF trial showed harm)
Management of Acute Decompensated HF
- Positioning: Sit upright (reduces preload)
- O₂/NIV: High-flow O₂; CPAP/BiPAP for pulmonary edema
- IV Loop diuretics: Furosemide IV (reduces preload, relieves congestion)
- Vasodilators: IV nitrates (GTN) for afterload/preload reduction — particularly in hypertensive pulmonary edema
- Inotropes: Dobutamine, milrinone — for cardiogenic shock / severe low output (short-term only; no mortality benefit)
- Vasopressors: Norepinephrine for cardiogenic shock with hypotension
- Continue/restart BB and RAAS therapy as soon as hemodynamically stable
- Identify and treat precipitants: FAILURE mnemonic — Forgot medications, Arrhythmia/Anemia, Ischemia/Infection, Life-style (salt/fluid), Urine output ↓ (renal failure), Raised BP, Embolism (PE)
Summary Table
| Domain | Key Points |
|---|---|
| Definition | Inability of heart to meet body's metabolic needs at normal filling pressures |
| Types | HFrEF (EF<40%), HFpEF (EF≥50%), HFmrEF; L/R/biventricular; acute/chronic; high/low output |
| Pathophysiology | LV remodeling driven by RAAS (Ang II, aldosterone) and SNS (catecholamines) activation |
| Clinical | Dyspnea, orthopnea, PND, fatigue; S3 gallop, displaced apex, elevated JVP, basal crepitations, edema |
| Diagnosis | Echo (cornerstone), BNP/NT-proBNP, CXR, ECG; MRI/biopsy in selected cases |
| Management HFrEF | ACEi/ARNI + β-blocker + MRA + SGLT2i (four pillars); diuretics for symptoms; ICD/CRT for devices |
| Management HFpEF | Diuretics + SGLT2i; aggressive RF control; no mortality-reducing drug proven |
| Acute HF | O₂, IV diuretics, vasodilators, treat precipitants; inotropes for shock |
— Textbook of Family Medicine 9e (Rakel), Braunwald's Heart Disease, Harrison's Principles of Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.