Iron and it's deficiency disorders, NACP and all - Pedia MBBS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching the Web
NACP National Anemia Control Programme India iron deficiency pediatric MBBS
Reading File
Reading File
Reading Web Page
https://www.nhm.gov.in/images/pdf/programmes/child-health/gu…
Loading Image
Reading File
I now have comprehensive data. Let me compile the complete, detailed answer for a Pediatrics MBBS student covering iron metabolism, IDA, and NACP/NNACP/NIPI/Anemia Mukt Bharat.
Iron and Iron Deficiency Disorders - Pediatrics MBBS
1. Iron in the Body - Normal Metabolism
Total body iron: ~4-5 g (males ~3450 mg, females ~2450 mg)
Distribution of Iron
| Pool | Males (mg) | Females (mg) |
|---|---|---|
| Hemoglobin | 2100 | 1750 |
| Myoglobin | 300 | 250 |
| Enzymes (cytochromes, catalase, peroxidase) | 50 | 50 |
| Storage (ferritin + hemosiderin) | 1000 | 400 |
- ~65% as hemoglobin, ~4% as myoglobin, ~1% in heme enzymes, ~0.1% as plasma transferrin, 15-30% in storage
Iron Transport and Storage
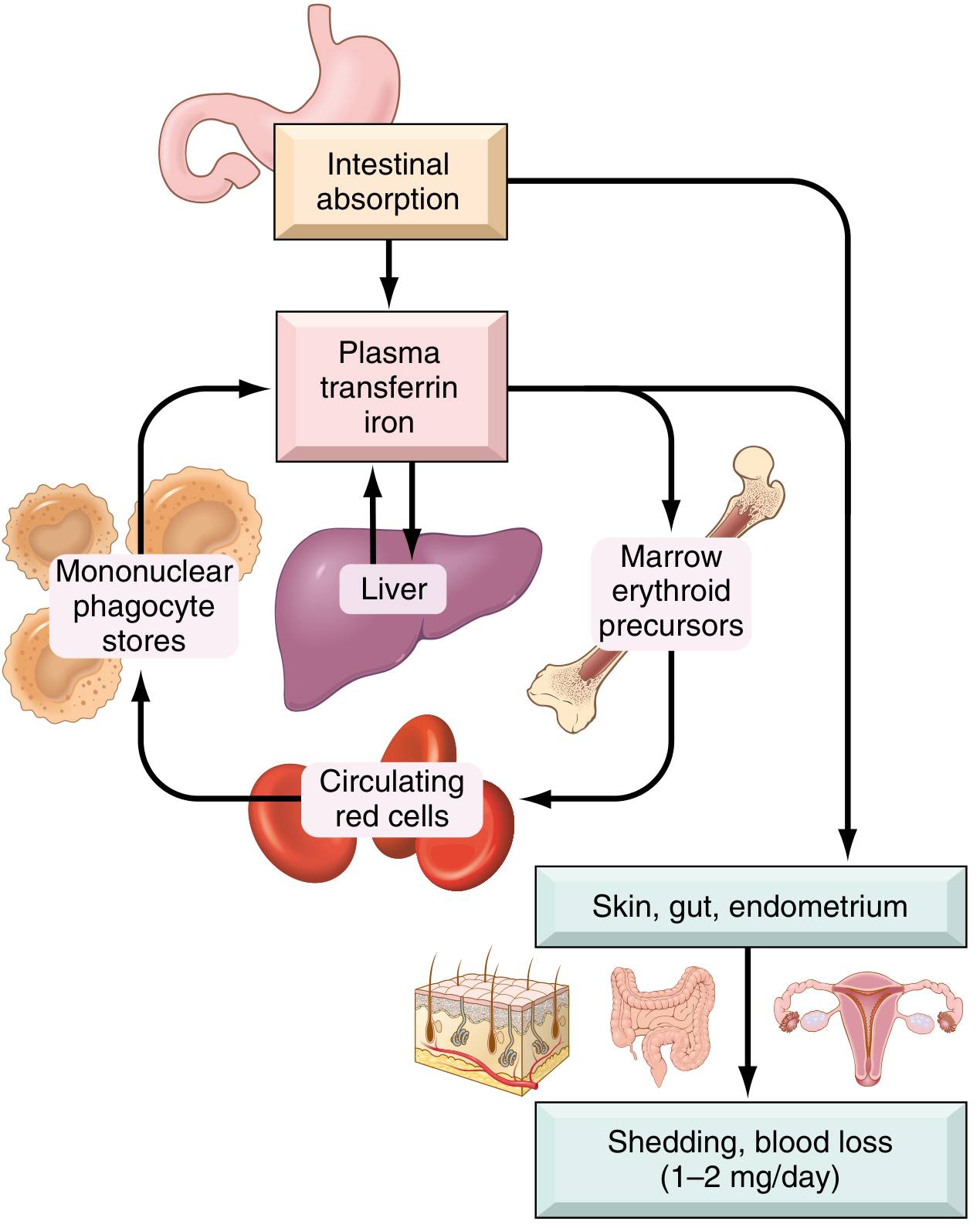
- Transferrin (beta-globulin, synthesized in liver): transports iron in plasma; normally ~1/3 saturated; serum iron ~120 µg/dL males, ~100 µg/dL females
- Ferritin: major storage form; iron bound to apoferritin protein shell (mol wt ~460 kDa, up to 4000 atoms/molecule); highest in hepatocytes and RES cells; plasma ferritin correlates with body iron stores (normal: >12 µg/L; iron deficiency: <12 µg/L)
- Hemosiderin: insoluble aggregates of partially degraded ferritin within lysosomes; stains blue-black with Prussian blue (potassium ferrocyanide); predominates in iron overload
- Transferrin delivers iron to erythroid precursors via receptor-mediated endocytosis; iron then goes to mitochondria where heme is synthesized
Iron Absorption (Duodenum)
- Daily diet contains 10-20 mg iron; only 10-15% absorbed
- Heme iron (from animal products): ~20% absorbed, transported by separate heme transporter
- Non-heme iron: Fe³⁺ reduced to Fe²⁺ by ferrireductases (b cytochromes), then taken up by DMT1 (divalent metal transporter 1); only 1-5% absorbed
- Fe²⁺ crosses the basolateral membrane via ferroportin, oxidized to Fe³⁺ by hephaestin/ceruloplasmin, then binds plasma transferrin
- Enhancers: ascorbic acid (Vit C), citric acid, amino acids, sugars
- Inhibitors: phytates (cereals), tannins (tea), calcium, phosphates
Hepcidin - The Master Regulator
- Peptide synthesized by liver
- When iron stores are high OR inflammation → hepcidin ↑ → binds ferroportin → ferroportin degraded → iron trapped in enterocytes as mucosal ferritin (lost when cells slough) → ↓ iron absorption; also blocks iron release from macrophages
- When iron stores are low → hepcidin ↓ → ferroportin intact → ↑ iron absorption
- Anemia of chronic disease = ↑ hepcidin → functional iron deficiency
- Hemochromatosis = ↓ hepcidin → excess absorption
Daily Iron Loss
- Males: ~0.6 mg/day (shed cells)
- Females: ~1-2 mg/day (+ menstrual losses)
- Net requirement: 1 mg must be absorbed daily
2. Iron Deficiency Anemia (IDA)
Most common nutritional disorder worldwide. In India, ~80% of children <3 years, ~58% pregnant women, ~56% adolescent girls are anemic.
Causes (Etiology)
1. Dietary deficiency (most common in infants/toddlers):
- Exclusive breastfeeding beyond 6 months without complementary feeding
- Cow's milk as main diet (low iron + inhibits absorption + causes occult GI blood loss)
- Predominantly plant-based diet (low bioavailability)
- Premature/low birth weight infants (depleted fetal stores)
2. Increased demand:
- Rapid growth: infants (6 months-2 years), adolescent growth spurt
- Pregnancy and lactation
3. Impaired absorption:
- Celiac disease, post-gastric surgery, achlorhydria
- Malabsorption syndromes
4. Chronic blood loss (most common cause in adults and older children):
- GI: hookworm, Meckel's diverticulum, IBD, peptic ulcer
- Urinary: hematuria
- Menstrual losses (adolescent girls)
Stages of Iron Deficiency (Important for MCQs)
| Stage | Description | Labs |
|---|---|---|
| Stage 1 - Iron depletion | Storage iron depleted, no anemia | ↓ Ferritin, bone marrow iron absent; Hb normal |
| Stage 2 - Iron-deficient erythropoiesis | Marrow runs out of iron; erythropoiesis falls | ↓ Serum iron, ↑ TIBC, ↓ transferrin saturation, ↑ free erythrocyte protoporphyrin (FEP) |
| Stage 3 - Iron deficiency anemia | Overt microcytic hypochromic anemia | ↓ Hb, ↓ MCV, ↓ MCH, ↑ RDW |
Clinical Features
General anemia symptoms:
- Pallor (conjunctival, palmar, nail beds), fatigue, exertional dyspnea, tachycardia
Specific to iron deficiency (even before anemia):
- Pica - craving for non-food substances (mud/clay = geophagia, ice = pagophagia, starch = amylophagia) - common in children
- Koilonychia (spoon-shaped nails)
- Angular stomatitis (cracking at corners of mouth)
- Glossitis (smooth, sore tongue)
- Brittle hair and nails
- Blue sclerae
- Plummer-Vinson syndrome (in adults): IDA + dysphagia + esophageal web
- Behavioral/developmental effects in children: irritability, poor attention span, impaired cognitive development, reduced school performance (may not be fully reversible even after iron treatment)
- Increased susceptibility to lead toxicity (pica + increased absorption of heavy metals)
- Breath-holding spells in toddlers
Growth retardation in severe/prolonged deficiency
Lab Findings (IDA)
| Parameter | IDA | Normal |
|---|---|---|
| Hb | ↓ | M >13 g/dL, F >12 g/dL, children >11 g/dL |
| MCV | ↓ (<80 fL) - microcytic | 80-100 fL |
| MCH | ↓ | 27-33 pg |
| MCHC | ↓ - hypochromic | 32-36 g/dL |
| RDW | ↑ (anisocytosis) | <14.5% |
| Serum iron | ↓ (<50 µg/dL) | 100-120 µg/dL |
| TIBC | ↑ (>360 µg/dL) | 250-370 µg/dL |
| Transferrin saturation | ↓ (<16%) | 20-50% |
| Serum ferritin | ↓ (<12 µg/L) - EARLIEST indicator | 20-200 µg/L |
| Serum transferrin receptor (sTfR) | ↑ | Useful to distinguish IDA from ACD |
| Reticulocyte count | Normal or ↓ | 0.5-1.5% |
| Blood smear | Microcytic hypochromic RBCs, target cells, pencil cells | - |
| Bone marrow | Absent stainable iron (Prussian blue negative) - GOLD STANDARD | Present |
Key MCQ fact: Serum ferritin is the most sensitive and specific single test for iron depletion. Serum ferritin is an acute phase reactant - may be falsely normal/elevated in inflammation even with iron deficiency.
Transferrin saturation = (Serum iron / TIBC) × 100; <16% suggests IDA
Peripheral Blood Smear - IDA
- Microcytic, hypochromic RBCs
- Anisocytosis, poikilocytosis
- Pencil (cigar) cells
- Target cells
- Thrombocytosis (reactive - in chronic blood loss)
Differential Diagnosis
| Feature | IDA | Thalassemia trait | ACD |
|---|---|---|---|
| MCV | ↓↓ | ↓ (usually more ↓) | Normal/↓ |
| RDW | ↑↑ | Normal | Normal |
| Serum iron | ↓ | Normal | ↓ |
| TIBC | ↑ | Normal | ↓/Normal |
| Ferritin | ↓ | Normal/↑ | Normal/↑ |
| Mentzer index (MCV/RBC) | >13 (IDA) | <13 (thalassemia) | - |
3. WHO Hb Cutoffs for Anemia Diagnosis
| Age/Group | Hb cutoff (g/dL) |
|---|---|
| 6-59 months | <11.0 |
| 5-11 years | <11.5 |
| 12-14 years | <12.0 |
| Women (non-pregnant) ≥15 years | <12.0 |
| Pregnant women | <11.0 |
| Men ≥15 years | <13.0 |
4. Treatment of IDA
Oral Iron (First Line)
- Ferrous salts (ferrous sulfate, ferrous gluconate, ferrous fumarate) - ferrous (Fe²⁺) absorbed better than ferric (Fe³⁺)
- Therapeutic dose in children: 3-6 mg/kg/day of elemental iron in 2-3 divided doses
- Best absorbed on empty stomach, but can give with food to reduce GI side effects
- Vitamin C (ascorbic acid) with iron enhances absorption
- Avoid with milk, tea, antacids
- Duration: Continue for 3 months after Hb normalizes to replenish stores
- Response monitoring:
- Reticulocyte count rises in 4-7 days (earliest response)
- Hb rises by ~1 g/dL/week
- Decision on effectiveness at 4 weeks (expect ≥2 g/dL rise)
Parenteral Iron
- Indications: malabsorption, non-compliance, severe ongoing blood loss exceeding oral absorption capacity, intolerance to oral iron
- Options: iron sucrose, ferric carboxymaltose, iron dextran
- Risk: anaphylaxis (especially iron dextran)
Blood Transfusion
- Only in severe symptomatic anemia (Hb <5-6 g/dL) with hemodynamic compromise or cardiac failure
- Use packed RBCs (10-15 mL/kg slowly)
Dietary advice
- Increase iron-rich foods: red meat, poultry, fish (heme iron); dark green leafy vegetables, legumes (non-heme iron)
- Cook in iron vessels (increases iron content of food)
- Vitamin C-rich foods with meals
- Reduce tea/coffee consumption with meals
- Delayed cord clamping at birth (2-3 min) - increases iron stores in newborn by ~50-75 mg
5. NACP / NNACP and Related Government Programs (India)
This is a frequently tested topic in Indian MBBS/PG exams. The program has evolved through several phases:
Evolution of the Program
| Year | Program Name | Key Change |
|---|---|---|
| 1970 | National Nutritional Anaemia Prophylaxis Programme (NNAPP) | First national program; targeted pregnant women |
| 1991 | National Nutritional Anaemia Control Programme (NNACP) | Renamed; emphasis shifted from prevention to management; dose increased to 100 mg elemental iron for adults |
| 2013 | National Iron Plus Initiative (NIPI) | Life cycle approach; expanded to all age groups including adolescents and children 6 months-10 years |
| 2018 | Anemia Mukt Bharat (AMB) | Current program; 6×6×6 strategy |
Anemia Mukt Bharat (AMB) - 2018 - The Current Program
Goal: Reduce anemia prevalence by 3 percentage points per year across target age groups
6×6×6 Strategy:
- 6 target beneficiary groups: Preschool children (6-59 months), School children (5-9 years), Adolescents (10-19 years), Pregnant women, Lactating women, Women of reproductive age (WRA, 15-49 years)
- 6 interventions:
- Prophylactic IFA supplementation
- Deworming (biannual)
- Intensified year-round behavior change communication (BCC)
- Testing for anemia using digital hemoglobinometers
- Non-nutritional anemia management (malaria, hemoglobinopathies)
- Fortified rice distribution via PDS
- 6 delivery platforms: AWCs (Anganwadi), ASHA, Schools, PHCs/CHCs, BPHUs, digital monitoring
NIPI / AMB - Iron Supplementation Schedule
Prophylactic IFA Supplementation:
| Age Group | Dose | Frequency | Duration |
|---|---|---|---|
| Infants 6-11 months | 20 mg elemental iron + 100 µg folic acid (liquid/drops) | Biweekly (every 2 weeks) | Throughout the period |
| Children 12-59 months | 20 mg elemental iron + 100 µg folic acid | Biweekly | Throughout the period |
| Children 5-10 years | 45 mg elemental iron + 400 µg folic acid (tablet) | Weekly | Throughout the year |
| Adolescents 10-19 years | 100 mg elemental iron + 500 µg folic acid (tablet) | Weekly | Throughout the year |
| Pregnant women | 100 mg elemental iron + 500 µg folic acid | Daily | 180 days (100 days antenatal + 100 days postnatal) |
| Lactating women | 100 mg elemental iron + 500 µg folic acid | Daily | 180 days postpartum |
| WRA (15-49 years) | 100 mg elemental iron + 500 µg folic acid | Weekly | Throughout the year |
Key MCQ: Preschool children (6-59 months) receive IFA biweekly | School children (5-9 yr) receive IFA weekly
Treatment Doses Under NIPI:
| Age Group | Severity | Dose |
|---|---|---|
| 6-59 months | Mild (Hb 10-10.9 g/dL) OR Moderate (Hb 7-9.9 g/dL) | 3 mg/kg/day elemental iron for 2 months |
| 6-59 months | Severe (Hb <7 g/dL) | Refer urgently to DH/FRU |
| 5-10 years | Mild/Moderate | 3 mg/kg/day for 2 months |
| 5-10 years | Severe (Hb <8 g/dL) | Refer urgently |
| 10-19 years | Mild/Moderate | 60 mg elemental iron daily for 3 months |
| 10-19 years | Severe (Hb <8 g/dL) | Refer urgently |
Treatment response monitoring: Hb estimation after 2 months of treatment; target Hb >11 g/dL (under-5) or appropriate age cutoff. If no response in 2 months → refer.
IFA Syrup Dose for Anemic Children 6 months-5 years (NIPI):
| Age / Weight | Dose |
|---|---|
| 6-12 months (6-10 kg) | 1 mL IFA syrup once daily |
| 1-3 years (10-14 kg) | 1.5 mL IFA syrup once daily |
| 3-5 years (14-19 kg) | 2 mL IFA syrup once daily |
WIFS (Weekly Iron and Folic Acid Supplementation)
- Specifically for school-going adolescents
- 100 mg iron + 500 µg folic acid weekly for boys and girls aged 10-19 years (school/non-school)
- Implemented through teachers (in-school) and AWC/ASHA (out-of-school)
- Combined with biannual deworming
6. Prevention of IDA - Summary
| Intervention | Detail |
|---|---|
| Delayed cord clamping | 2-3 min after birth; ↑ neonatal iron stores by 50-75 mg |
| Breastfeeding | Encourages first 6 months; iron in breast milk is highly bioavailable |
| Iron-fortified formula | For non-breastfed infants |
| Complementary feeding | Start at 6 months; include iron-rich foods |
| IFA prophylaxis (NIPI/AMB) | As per schedule above |
| Deworming | Biannual (Albendazole 400 mg); reduces GI blood loss from helminths |
| Vitamin C supplementation | Enhances non-heme iron absorption |
| Dietary diversification | Promote iron-rich foods; cooking in iron vessels |
Key MCQ Pearls
- Most common nutritional deficiency worldwide = Iron deficiency
- Most sensitive test for iron depletion = Serum ferritin (first to fall, last to normalize)
- Gold standard for tissue iron = Bone marrow Prussian blue stain (absent stainable iron)
- Earliest response to iron therapy = Reticulocyte count rises in 4-7 days
- Pica is pathognomonic of iron deficiency (not just anemia)
- Mentzer index = MCV/RBC count: >13 favors IDA, <13 favors thalassemia trait
- Hepcidin = master regulator of iron absorption; ↑ in inflammation (ACD), ↓ in IDA and hemochromatosis
- Koilonychia = spoon-shaped nails, specific to IDA
- NIPI introduced the life cycle approach in 2013; AMB (2018) uses 6×6×6 strategy
- IFA for children 6-59 months = 20 mg iron + 100 µg folate, biweekly
- IFA for 5-10 years = 45 mg iron + 400 µg folate, weekly
- IFA for adolescents = 100 mg iron + 500 µg folate, weekly
- Therapeutic dose of iron in children = 3-6 mg/kg/day (treatment); prophylactic = 1-2 mg/kg/day
- Cow's milk anemia: exclusively cow's milk fed infants develop IDA due to low iron content + GI blood loss from cow's milk protein intolerance
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goodman & Gilman's Pharmacological Basis of Therapeutics; Guyton & Hall - Medical Physiology; The Harriet Lane Handbook (23rd ed.); NHM India - NIPI Guidelines & Anemia Mukt Bharat Operational Guidelines; National Iron Plus Initiative - PMC6886130
This is a shared conversation. Sign in to Orris to start your own chat.