Write me about rectus sheath for a long answer mbbs exam with diagrams .
Reading File
Finding Sources
Searching the Web
rectus sheath anatomy MBBS long answer formation contents clinical importance
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the content needed for a comprehensive MBBS long-answer response. Let me compile the full answer with diagrams.
Rectus Sheath
Introduction
The rectus sheath is a strong aponeurotic compartment enclosing the rectus abdominis and pyramidalis muscles. It is formed by the interlacing aponeuroses of the three flat muscles of the lateral abdominal wall - the external oblique, internal oblique, and transversus abdominis. Its composition changes significantly above and below the arcuate line (line of Douglas), which is one of the most tested anatomical facts in MBBS examinations.
Formation of the Rectus Sheath
The sheath is formed by a unique layering arrangement that differs at two levels:
Above the Arcuate Line (Upper Three-Quarters of the Rectus Abdominis)
| Layer | Composition |
|---|---|
| Anterior wall | Aponeurosis of external oblique + anterior lamella of internal oblique |
| Posterior wall | Posterior lamella of internal oblique + aponeurosis of transversus abdominis |
The internal oblique aponeurosis splits at the lateral border of the rectus abdominis into two lamellae - one passing in front and one behind the muscle. The rectus is thus completely enclosed above the arcuate line.
Below the Arcuate Line (Lower One-Quarter of the Rectus Abdominis)
| Layer | Composition |
|---|---|
| Anterior wall | Aponeuroses of all three muscles (external oblique + internal oblique + transversus abdominis) |
| Posterior wall | ABSENT - only transversalis fascia and peritoneum |
At approximately the midpoint between the umbilicus and the pubic symphysis (3-5 cm below the umbilicus), all three aponeuroses pass entirely anterior to the rectus abdominis. The lower posterior surface of the muscle is in direct contact with the transversalis fascia, separated from peritoneum only by preperitoneal fat.
Mnemonics:
- Above arcuate line: "EI / IT" (External+Internal Anterior / Internal+Transversus Posterior)
- Below arcuate line: All three go anterior, posterior = Transversalis fascia only
Diagrams
Fig. 1 - Transverse sections through the rectus sheath (Gray's Anatomy for Students)
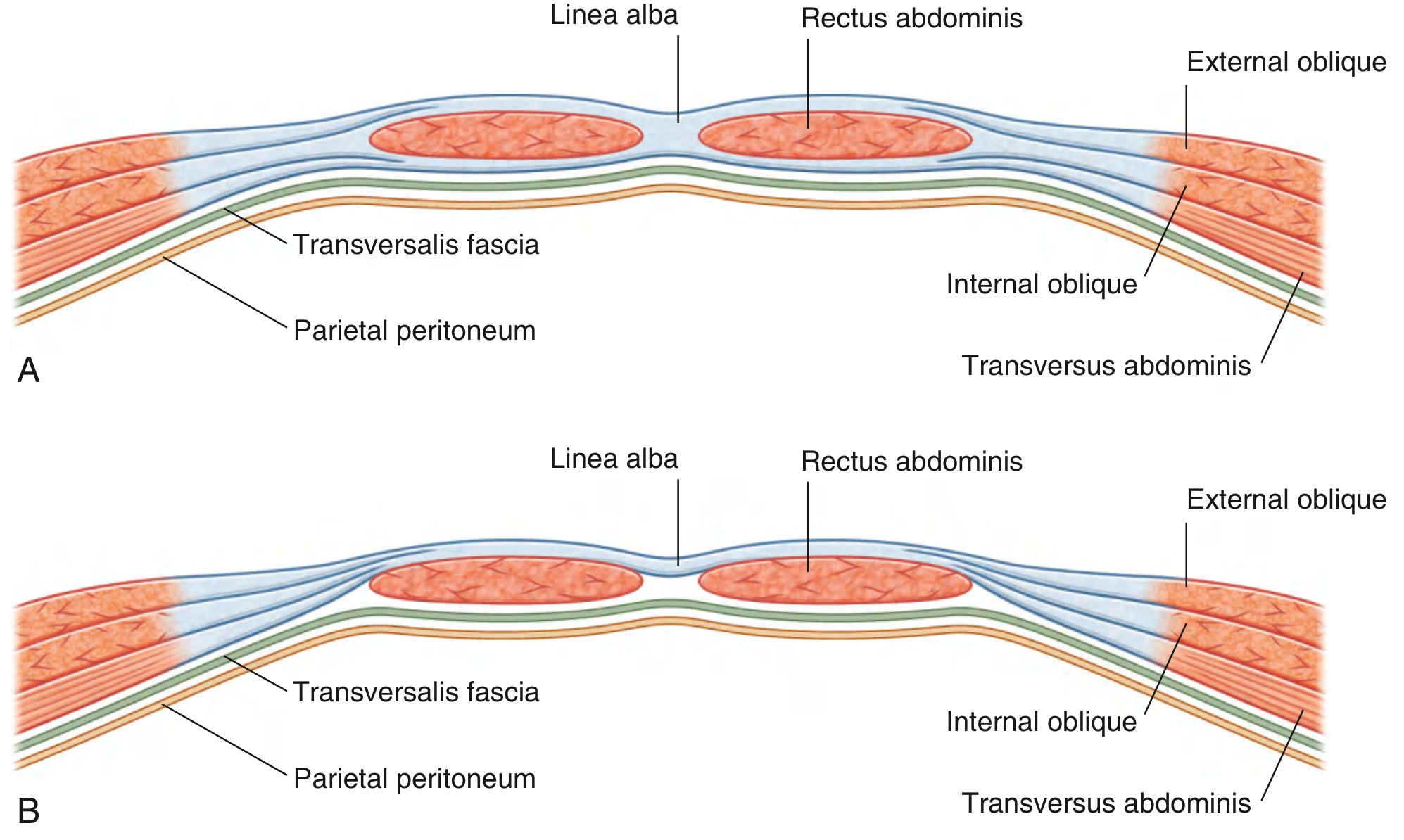
(A) Above the arcuate line - note the complete anterior and posterior walls enclosing the rectus abdominis, with transversalis fascia and peritoneum deep to them. (B) Below the arcuate line - all aponeuroses shift anteriorly; only transversalis fascia and peritoneum remain posteriorly.
Fig. 2 - Detailed labeled cross-sections (Mulholland & Greenfield's Surgery)
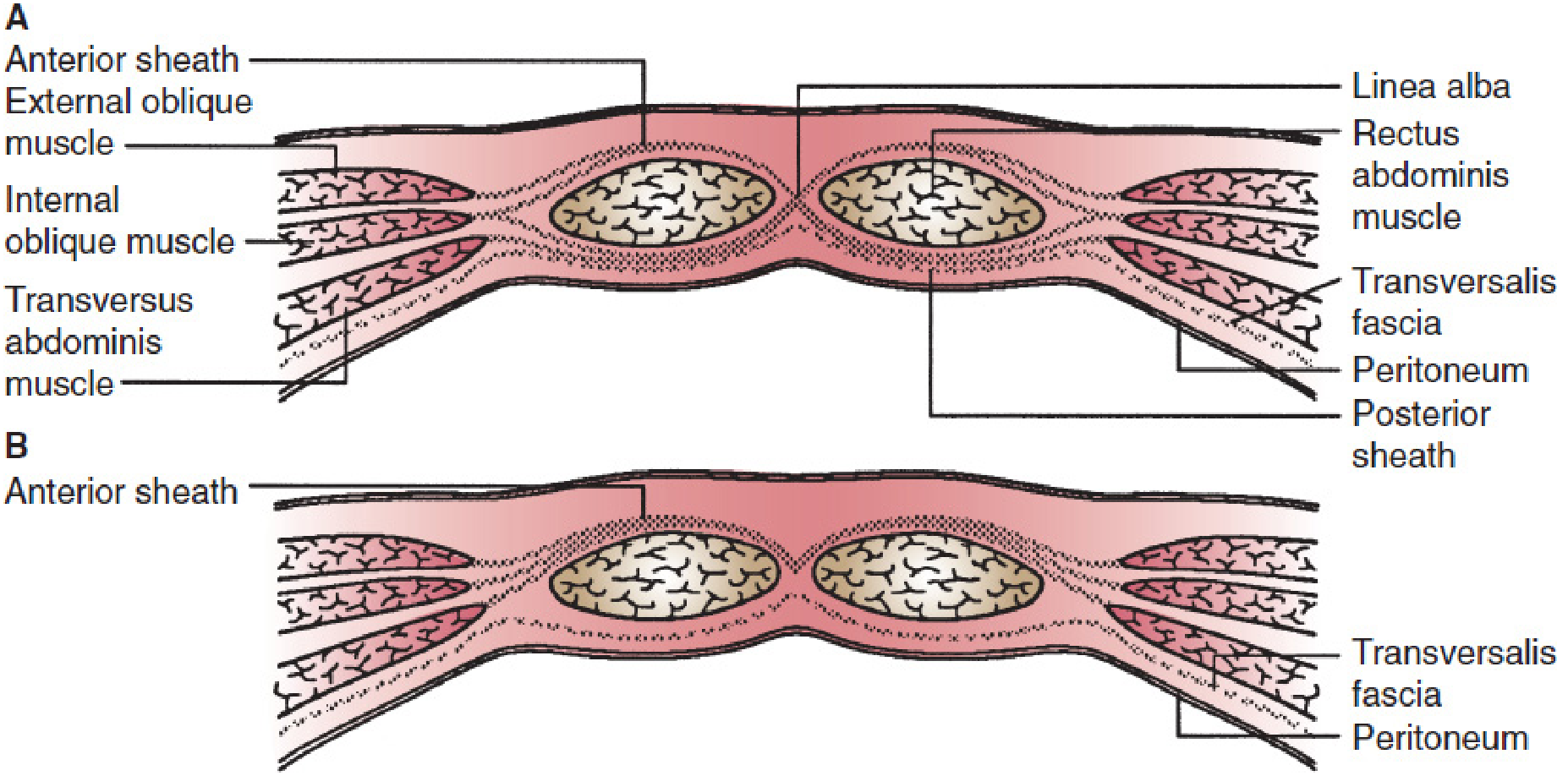
(A) Superior to the arcuate line: both anterior and posterior sheaths are well-defined. (B) Below the arcuate line: only an anterior sheath exists; transversalis fascia and peritoneum form the posterior boundary.
The Arcuate Line (Line of Douglas / Linea Semicircularis)
- A crescent-shaped curved lower free border of the posterior wall of the rectus sheath
- Located approximately midway between the umbilicus and the pubic symphysis (commonly stated as 3-5 cm below the umbilicus)
- Below this line, the posterior wall of the rectus sheath is absent
- The inferior epigastric vessels and their branches are relatively fixed here, making them vulnerable to shearing forces
Boundaries of the Rectus Sheath
| Boundary | Structure |
|---|---|
| Medially | Linea alba (midline fusion of all aponeuroses) |
| Laterally | Linea semilunaris (semilunar line) - slight depression marking lateral edge of rectus |
| Anteriorly | Anterior wall of sheath (as above) |
| Posteriorly | Posterior wall above arcuate line; transversalis fascia below |
The linea semilunaris marks the site where the aponeuroses of the lateral muscles first insert onto the rectus sheath - it is visible as a curved groove in muscular individuals.
Contents of the Rectus Sheath
- Rectus abdominis muscle - a paired, longitudinal strap muscle running from the pubic crest and symphysis to the xiphoid process and 5th-7th costal cartilages; crossed by 3 tendinous inscriptions (basis of the "six-pack")
- Pyramidalis muscle - a small triangular muscle anterior to the lower part of rectus abdominis; absent in about 20% of people; lies between the pubic symphysis and the linea alba
- Superior epigastric artery - terminal branch of the internal thoracic (internal mammary) artery; enters the sheath below the costal margin
- Inferior epigastric artery - branch of the external iliac artery; enters the sheath below the arcuate line from the lateral side
- Superior and inferior epigastric veins - accompany their respective arteries
- Lower five intercostal nerves and subcostal nerve (T7-T12) - pierce the lateral aspect of the rectus sheath to innervate the rectus abdominis
- Lymphatic vessels
The superior and inferior epigastric arteries anastomose near the umbilicus, forming an important collateral pathway between the subclavian and external iliac systems.
Blood Supply
| Artery | Origin | Entry into Sheath |
|---|---|---|
| Superior epigastric | Internal thoracic artery | Enters above, through posterior sheath below costal margin |
| Inferior epigastric | External iliac artery | Enters below arcuate line, medial to deep inguinal ring |
| Lower intercostal arteries (7th-11th) | Thoracic aorta | Pierce lateral aspect of sheath |
Nerve Supply
The rectus abdominis is innervated segmentally by the anterior rami of T7-T12 (lower 6 thoracoabdominal nerves). These nerves travel between the internal oblique and transversus abdominis, then pierce the lateral wall of the rectus sheath to enter and supply the muscle. This segmental arrangement is why a paramedian incision (made lateral to the rectus, splitting the sheath) risks denervating the medial part of the muscle if the nerves are cut - a known complication predisposing to ventral hernia.
Related Structures / Topographic Landmarks
- Tendinous inscriptions: 3 transverse fibrous bands crossing the rectus anteriorly (at xiphoid, umbilicus, and midway between them), firmly attached to the anterior sheath but NOT to the posterior sheath - this is why blood/pus can track freely behind the muscle
- Linea alba: midline fusion of all aponeuroses from xiphoid to pubic symphysis
- Linea semilunaris: lateral border of the rectus sheath - site of Spigelian hernias
Clinical Importance
1. Rectus Sheath Hematoma
- Caused by rupture of the inferior epigastric artery or its branches, most commonly at or near the arcuate line where the vessel is relatively fixed and susceptible to shearing
- Predisposing factors: trauma, vigorous coughing/sneezing (chronic pulmonary disease), anticoagulation therapy, laparoscopic trocar injury
- Clinically presents as sudden onset abdominal pain with a palpable abdominal wall mass
- Fothergill's sign: a mass palpable in the abdominal wall that does not change position (does not disappear) when the patient tenses the rectus muscles - distinguishes rectus sheath hematoma from intraperitoneal pathology
- May mimic appendicitis (right-sided hematoma)
- Below the arcuate line, the absent posterior sheath allows hematoma to spread freely in the prevesical space
- Diagnosis: ultrasound or CT scan with IV contrast
- Treatment: conservative (compression, reversal of anticoagulation) for stable patients; angiographic embolization for larger hematomas or haemodynamic instability; surgical evacuation if all else fails
2. Spigelian Hernia
- Herniation through the linea semilunaris (at the junction of the arcuate line and the semilunar line)
- Most occur just below the umbilicus near the edge of the rectus sheath
- Clinically challenging to detect as the hernia often lies below the external oblique aponeurosis (interparietal hernia)
3. Diastasis Recti
- Widening of the linea alba between the two rectus muscles
- Not a true hernia (midline fascia intact; no risk of incarceration/strangulation)
- Common in obesity, pregnancy, and after multiple surgeries
- Treated conservatively; surgery (open or laparoscopic plication) only for significant functional disability or cosmesis
4. Surgical Incisions Through the Rectus Sheath
| Incision | Description | Advantage/Disadvantage |
|---|---|---|
| Midline (median) | Through linea alba | Avascular, quick; poor healing due to low vascularity |
| Paramedian | Through anterior sheath, rectus retracted laterally | Good access; risks denervation if nerves cut medially |
| Pfannenstiel | Transverse incision through anterior sheath below umbilicus | Used in obstetric/pelvic surgery; good cosmesis |
| Kocher's | Subcostal oblique | Upper abdominal viscera |
5. Rectus Sheath Block (Regional Anesthesia)
- Local anaesthetic injected into the space between the rectus muscle and the posterior sheath bilaterally
- Used for midline abdominal wall analgesia (umbilical hernia repair, laparoscopy port sites)
- Effective because the thoracoabdominal nerves (T9-T11) run in this plane
6. Posterior Rectus Sheath Release (Component Separation)
- A technique used in complex abdominal wall reconstruction (large ventral hernias)
- The posterior rectus sheath is divided and the transversus abdominis aponeurosis is released, allowing the abdominal wall components to advance medially to close large defects
Summary Table
| Feature | Above Arcuate Line | Below Arcuate Line |
|---|---|---|
| Anterior wall | External oblique + ant. lamella of internal oblique | All three aponeuroses |
| Posterior wall | Post. lamella of internal oblique + transversus abdominis | Absent (transversalis fascia only) |
| Posterior sheath | Complete | Absent |
| Rectus muscle covered posteriorly by | Aponeurotic sheath | Transversalis fascia |
Key Points for the Examiner
- The arcuate line is at the junction of the upper 3/4 and lower 1/4 of the rectus abdominis - roughly 3-5 cm below the umbilicus.
- Below the arcuate line, the posterior wall is ABSENT - only transversalis fascia + peritoneum remain.
- The inferior epigastric vessels are particularly vulnerable to injury at the arcuate line.
- Tendinous inscriptions of the rectus abdominis are attached only to the ANTERIOR sheath, not the posterior sheath - allowing pus or blood to track posterior to the muscle freely.
- Fothergill's sign is positive in rectus sheath hematoma.
- Spigelian hernias occur at the linea semilunaris, typically near the level of the arcuate line.
Sources: Gray's Anatomy for Students; Schwartz's Principles of Surgery, 11th ed.; Mulholland & Greenfield's Surgery, 7th ed.; THIEME Atlas of Anatomy - General Anatomy & Musculoskeletal System; Bailey & Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.