Here is the complete, structured answer for all topics in both chapters.
CHAPTER 1 - VIRUSES CAUSING HEPATITIS
ENUMERATE THE VIRUSES CAUSING HEPATITIS
Hepatitis viruses are a taxonomically diverse (heterogeneous) group of viruses that share one common feature: they are hepatotropic (they infect and damage the liver). They are classified into six types - HAV through HGV (excluding "F" which was disproved):
| Virus | Family | Genome | Transmission | Chronicity |
|---|
| HAV | Picornaviridae (genus Hepatovirus) | ssRNA (+) | Fecal-oral | No |
| HBV | Hepadnaviridae | Partially ds-DNA | Parenteral, sexual, vertical | Yes (5-10%) |
| HCV | Flaviviridae (genus Hepacivirus) | ssRNA (+) | Parenteral | Yes (>70%) |
| HDV | Unclassified (deltavirus) | ssRNA (-), circular | Parenteral (requires HBV) | Yes (with HBV) |
| HEV | Hepeviridae | ssRNA (+) | Fecal-oral | No (rarely in immunosuppressed) |
| HGV | Flaviviridae | ssRNA (+) | Parenteral | Uncertain significance |
Other viruses that can cause sporadic hepatitis (not primarily hepatotropic):
- Cytomegalovirus (CMV)
- Epstein-Barr virus (EBV)
- Herpes simplex virus (HSV)
- Adenoviruses
- Rubella virus
- Hantaviruses
- Mumps virus
- Enteroviruses (Coxsackieviruses)
- Yellow fever virus - an arbovirus (Flaviviridae) causing hemorrhagic fever with hepatitis
HEPATITIS B VIRUS (HBV) - COMPREHENSIVE
1. MORPHOLOGY (Structure)
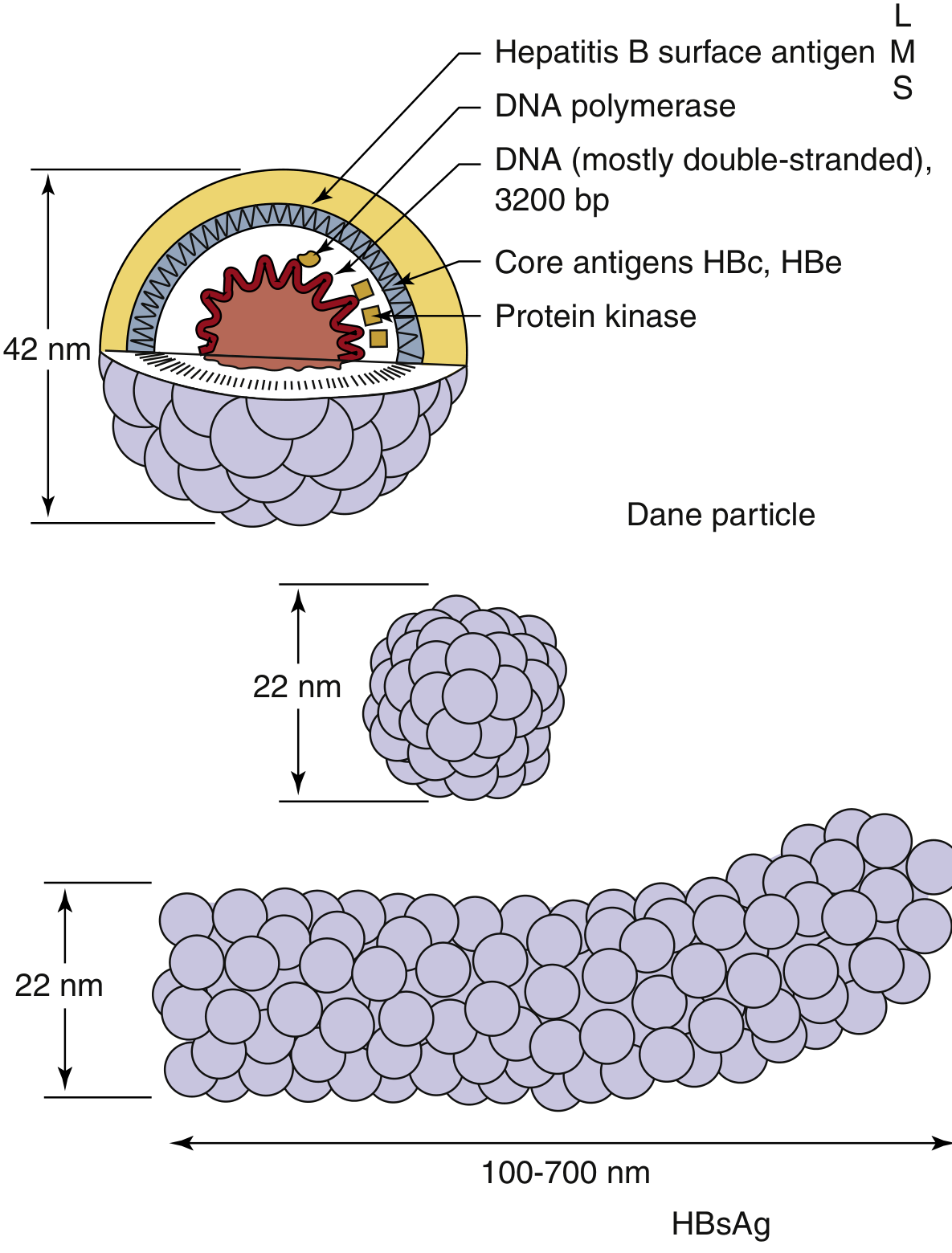
HBV belongs to the family Hepadnaviridae. The complete infectious virion is called the Dane particle.
Dane Particle:
- Size: 42 nm in diameter
- Enveloped virus
- Contains:
- Outer envelope: carries HBsAg (Hepatitis B surface antigen) in three forms: L (large/gp42), M (medium/gp36), S (small/gp27)
- Inner icosahedral nucleocapsid/core: composed of HBcAg (Hepatitis B core antigen)
- Genome: Partially double-stranded circular DNA, ~3200 base pairs (unique among DNA viruses - replicates via RNA intermediate using reverse transcriptase)
- DNA polymerase with reverse transcriptase and RNase H activity
- Protein kinase
- HBeAg: non-structural protein encoded by precore region; secreted into serum
Fig: Hepatitis B virus (Dane particle) and HBsAg particles - Medical Microbiology 9e
HBsAg particles in serum (non-infectious, outnumber virions):
- Spherical particles: 22 nm diameter, composed mainly of S-form HBsAg
- Tubular/Filamentous particles: 22 nm wide, 100-700 nm long, composed of S, M, and L forms
Genome Organization (4 major open reading frames):
- S gene: encodes HBsAg (S, M, L forms = surface antigen)
- C gene / Precore: encodes HBcAg (core) and HBeAg (precore)
- P gene: encodes DNA polymerase (reverse transcriptase)
- X gene: encodes HBxAg - a transactivating factor implicated in hepatocellular carcinoma (HCC)
Serotypes/Genotypes:
- HBV divided into 4 major serotypes (adr, adw, ayr, ayw) based on antigenic epitopes on HBsAg envelope protein
- 8-10 major genotypes (A through H/J) based on DNA sequence; immunity is NOT serotype-specific
- Genotype C: associated with higher risk of cirrhosis and HCC; low response to interferon treatment
2. MODES OF TRANSMISSION
HBV is present in blood, serum, saliva, semen, vaginal secretions, breast milk, and other body fluids.
- Sexual transmission - most common route in developed countries (particularly homosexual males at higher risk)
- Parenteral / Blood-borne transmission:
- Blood transfusions (residual risk ~1 in 600,000 with screening)
- Sharing IV drug use needles
- Needle-stick injuries (health care workers)
- Hemodialysis
- Tattooing, acupuncture with unsterilized equipment
- Vertical (Perinatal) transmission - from HBsAg-positive mother to neonate (usually at or around delivery, not in utero). Carrier rate if infected perinatally: ~90%; if infected as adults: ~5-10%
- Horizontal transmission in childhood - skin abrasions, contact with infected secretions (common in endemic areas)
- HBV is NOT transmitted by the fecal-oral route, breast milk (generally), casual contact (hugging, kissing), contaminated food, or water
Key risk factor for chronicity: Age at infection inversely correlates with chronicity - perinatal infection → 90% chronic; early childhood → 30%; adults → 5-10%
3. PATHOGENESIS
HBV pathogenesis is primarily immune-mediated, not directly cytopathic.
Steps:
- Entry: HBV attaches to hepatocytes via HBsAg glycoproteins binding to the sodium/bile acid cotransporter NTCP (sodium taurocholate cotransporting polypeptide)
- After entry, the nucleocapsid delivers the partially ds-DNA genome to the nucleus where it is completed into a covalently closed circular DNA (cccDNA) - a viral minichromosome that persists in infected hepatocytes
- The genome is transcribed, producing 4 types of mRNA including a 3500-base pregenomic RNA (pgRNA)
- Replication: pgRNA is packaged into core particles; reverse transcriptase synthesizes negative-sense DNA from the RNA template; RNA is degraded; positive-sense DNA is partially synthesized → new virions released by exocytosis
Immune-mediated liver damage:
- Hepatocytes carrying viral antigens are recognized by CD8+ cytotoxic T cells and NK cells - these kill infected hepatocytes → liver damage
- In adults with intact immunity: robust immune response → clearance (~95%)
- In neonates/infants: immature immune response → virus tolerated → carrier state (immune tolerance phase)
Consequences of chronic infection:
- Chronic active hepatitis → cirrhosis → hepatocellular carcinoma (HCC)
- HBV X gene product (HBxAg) transactivates cellular growth genes, promotes carcinogenesis
- Integration of HBV DNA into host genome triggers chromosomal rearrangements
- PHC (primary hepatocellular carcinoma) - HBV one of the three most common causes of cancer mortality worldwide
4. LABORATORY DIAGNOSIS OF HBV - SEROLOGICAL MARKERS AND SIGNIFICANCE
The serological picture describes the course and nature of HBV infection. There are three antigen-antibody systems:
A. Hepatitis B Surface Antigen/Antibody (HBsAg / Anti-HBs)
HBsAg (Australia antigen):
- First detectable marker; appears 1-10 weeks after exposure (before symptoms)
- Indicates active infection (acute or chronic)
- Presence for >6 months = chronic infection
- Detected by: ELISA, chemiluminescence, ICT
Anti-HBs (Antibody to HBsAg):
- Appears after clearance of HBsAg (after resolution)
- Indicates: recovery + immunity OR successful vaccination
- Only marker positive in vaccinated individuals
- HBsAg and anti-HBs cannot be detected simultaneously (immune complex obscures both) → "window period"
B. Hepatitis B Core Antigen/Antibody (HBcAg / Anti-HBc)
HBcAg:
- Hidden antigen; surrounds the viral core
- NOT detectable in serum (non-secretory, enclosed within HBsAg coat)
- Detectable only in hepatocytes by immunofluorescence
Anti-HBc:
- First antibody to appear; detected during the "window period" (after HBsAg disappears but before anti-HBs appears)
- IgM anti-HBc = marker of acute HBV infection (diagnostic during window period)
- IgG anti-HBc = marker of past infection; persists for decades
- Anti-HBc is present in both acute AND chronic infection; absent only in vaccinated persons
Window Period: The HBsAg window is the diagnostic gap when HBsAg has cleared but anti-HBs has not yet appeared. During this time, IgM anti-HBc is the only detectable marker - it is the diagnostic marker of acute HBV.
C. Hepatitis Be Antigen/Antibody (HBeAg / Anti-HBe)
HBeAg:
- Encoded by precore region; a soluble, secreted protein
- Present in serum when active viral replication is occurring
- Best correlate of viral infectivity - its detection indicates high viral load and high infectiousness
- Its persistence beyond 3 months indicates progression toward chronic hepatitis
- NOT detectable in "precore mutant" strains of HBV
Anti-HBe:
- Appears after clearance of HBeAg
- Signals reduction in infectivity and viral replication
- In chronic HBV, transition from HBeAg+ to anti-HBe+ (seroconversion) = good prognostic sign
Serological Marker Interpretation Table
| HBsAg | HBeAg | Anti-HBc (IgM) | Anti-HBc (IgG) | Anti-HBe | Anti-HBs | Interpretation |
|---|
| + | + | + | - | - | - | Acute HBV, high infectivity |
| + | - | - | + | + | - | Chronic HBV, low infectivity (precore mutant possible) |
| + | + | - | + | - | - | Chronic active HBV, high infectivity |
| - | - | + | - | - | - | Window period (acute) |
| - | - | - | + | + | + | Past infection, resolved |
| - | - | - | - | - | + | Vaccination (only anti-HBs) |
Additional Tests:
- HBV DNA (Viral Load): Detected by PCR; quantified by real-time PCR; most sensitive indicator of viral replication; used for monitoring treatment response and guiding antiviral therapy
- Liver enzymes (ALT, AST): Elevated in hepatitis; not specific but indicate hepatocyte injury
- Liver biopsy: "Gold standard" for staging HBV infection (degree of fibrosis); Fibroscan (elastography) is non-invasive alternative
- HBcAg: Detected in liver biopsy specimens by immunofluorescence
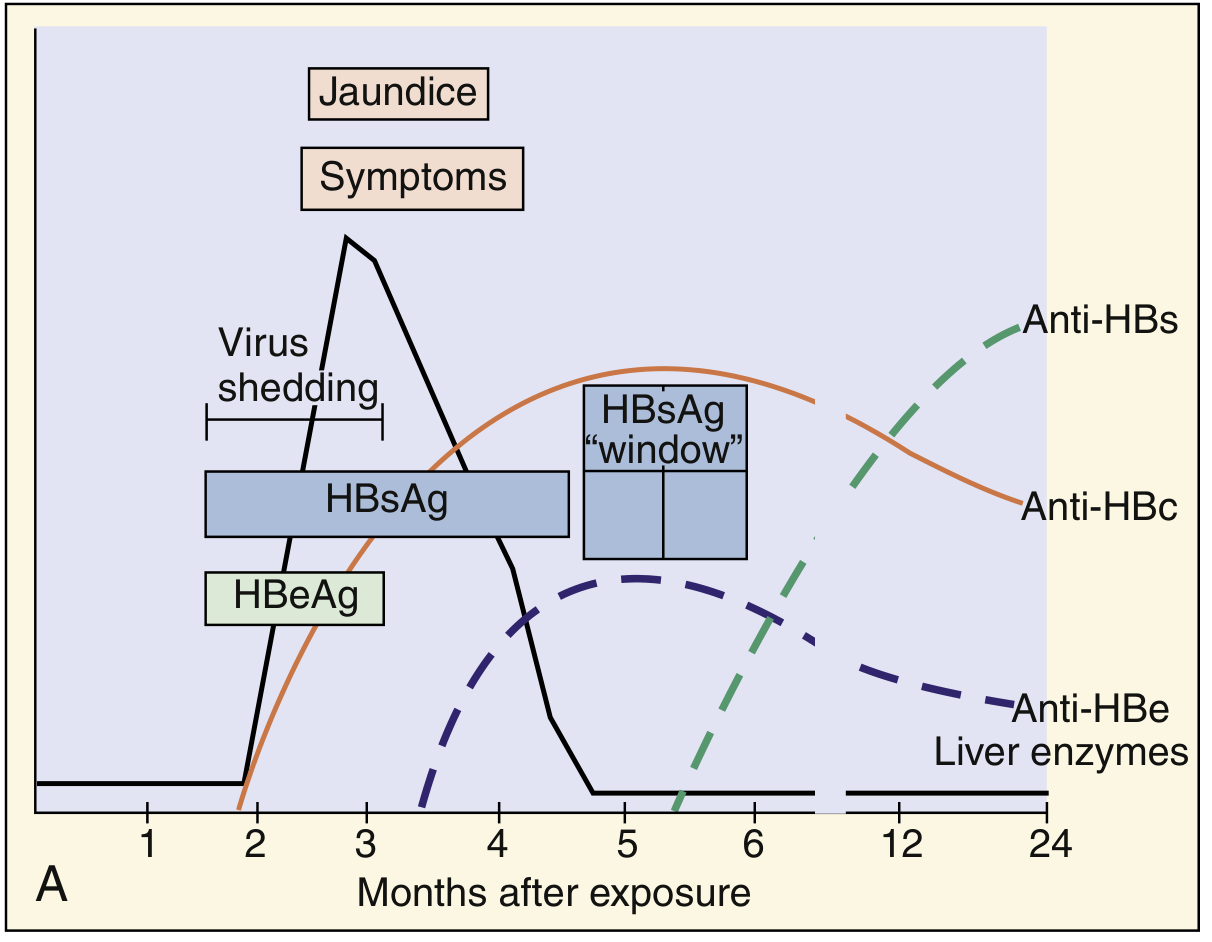
Fig: Serological events in acute HBV infection - Medical Microbiology 9e
Markers of ACUTE HBV infection (summary):
- HBsAg - earliest marker
- HBeAg - active replication marker
- IgM anti-HBc - the most specific marker of ACUTE infection (present even during window period)
- Elevated serum ALT/AST
5. PREVENTION OF HBV
A. Passive Immunization (Post-exposure prophylaxis)
- Hepatitis B Immunoglobulin (HBIG): Contains high-titer anti-HBs
- Given within 7 days of exposure (needle-stick) or within 24 hours of birth to neonate of HBsAg+ mother
- Provides immediate but temporary protection
B. Active Immunization - Hepatitis B Vaccines
First-generation vaccine (now obsolete):
- Plasma-derived vaccine: HBsAg purified from plasma of chronic carriers
- Safe but concerns about blood-borne pathogens
Second-generation vaccine (currently used):
- Recombinant DNA (yeast-derived) vaccine - most widely used globally
- HBsAg (S-protein) expressed in Saccharomyces cerevisiae by recombinant DNA technology
- Trade names: Recombivax HB, Engerix-B
- Highly immunogenic, safe (no blood products)
Third-generation vaccine:
- Contains pre-S1 and pre-S2 antigens in addition to S protein
- Better immune response in non-responders
Schedule (standard):
- 3 doses: 0, 1, and 6 months (IM in deltoid)
- Infants of HBsAg+ mothers: HBIG + vaccine within 24 hours of birth
- For newborns: 0, 1-2, and 6-18 months
Seroconversion rates:
- Healthy adults: ~95% respond
- Non-responders (~5-10%): do not develop anti-HBs even after 6 doses; HLA-linked non-response
- Immunocompromised, obese, smokers, elderly: lower response rates
Combined vaccines available:
- Twinrix = HAV + HBV vaccine
- Pentavalent vaccine (includes HBV, DTP, Hib)
Other prevention measures:
- Screening blood donations for HBsAg and anti-HBc
- Universal precautions for healthcare workers
- Needle exchange programs
- Safe sex (condoms)
- No sharing of razors, toothbrushes, needles
HEPATITIS A - LABORATORY DIAGNOSIS
HAV Morphology: 27-32 nm icosahedral particle, non-enveloped, linear ssRNA(+), family Picornaviridae (genus Hepatovirus). Single serotype; 7 genotypes.
Laboratory Diagnosis of HAV:
-
Anti-HAV IgM (Method of choice for acute diagnosis):
- Detected by ELISA
- Appears at onset of symptoms; persists 3-6 months
- Positive = acute HAV infection
-
Anti-HAV IgG:
- Appears 1 week after IgM
- Persists for decades (lifelong)
- Detection in absence of IgM = past infection or vaccination (immunity)
- Used in seroprevalence studies
-
HAV Antigen detection (rarely used clinically):
- ELISA or immunofluorescence on stool samples
- HAV shed in feces 2 weeks before to 2 weeks after onset of jaundice
-
PCR (RT-PCR for HAV RNA):
- Detects HAV RNA in blood and stool during viremic phase
- Used for genotyping and outbreak investigation
-
Liver function tests (ALT/AST): Elevated, non-specific
Key point: HAV does NOT cause chronic infection. No carrier state. ELISA is the method of choice; many rapid test formats available.
HEPATITIS C - LABORATORY DIAGNOSIS
HCV morphology: Spherical, 40 nm, enveloped, ssRNA(+). Family Flaviviridae, genus Hepacivirus. Has three structural proteins: nucleocapsid core protein C; two envelope glycoproteins E1 and E2. Six non-structural proteins (NS2, NS3, NS4A, NS4B, NS5A, NS5B). One p7 membrane protein.
HCV genotypes: 6 major genotypes (1-6); genotype 1 most common worldwide. Genotyping important for treatment decisions.
Laboratory Diagnosis:
-
Anti-HCV (ELISA / CIA):
- Screening test of choice
- First and second generation ELISA: now obsolete (less sensitive)
- Third-generation ELISA: uses antigens from NS5 region in addition to core, NS3, NS4 regions; sensitivity/specificity >99%; becomes positive ~5 weeks post-infection
- Limitation: does not distinguish acute from chronic or resolved infection
-
HCV RNA (RT-PCR/NAAT):
- Most sensitive test; detects viremia within 1-2 weeks of infection
- Qualitative PCR: for diagnosis and confirmation of anti-HCV positive results
- Quantitative RT-PCR (viral load): for monitoring antiviral treatment
- HCV RNA prevalence in general population is >0.1%
-
Recombinant Immunoblot Assay (RIBA) - formerly used as confirmatory test after ELISA; now obsolete as PCR is preferred
-
HCV Core Antigen:
- ELISA-based
- Detectable earlier than anti-HCV; correlates with viral load
- Useful when NAT unavailable
-
HCV Genotyping (PCR-based): Required before initiating antiviral therapy (direct-acting antivirals)
-
Liver biopsy / Fibroscan: Staging of liver fibrosis
HCV does NOT spread through breast milk, food, water, hugging, kissing, or casual contact. Vertical transmission rate is ~4% (much lower than HBV ~20%). Sexual transmission is rare.
YELLOW FEVER
Classification: Family Flaviviridae. Prototype flavivirus. Single serotype; 7 genotypes (5 in Africa, 2 in South America).
Vector: Aedes aegypti mosquito (urban cycle); Haemagogus species (jungle/sylvatic cycle)
Transmission cycles:
- Jungle (sylvatic) cycle: Between forest mosquitoes and monkeys
- Urban cycle: Aedes aegypti → human → Aedes aegypti
Pathogenesis:
- Mosquito inoculates virus into skin
- Virus multiplies in local lymph nodes → spreads to liver, spleen, kidney, bone marrow, heart
- Viremia during early phase (source of infection for mosquitoes)
- Liver: midzone necrosis of hepatocytes, Councilman bodies (eosinophilic inclusion bodies - necrotic hepatocytes), fatty change
- Kidneys: fatty degeneration and necrosis of tubular epithelium
Clinical Features:
- Incubation: 3-6 days
- Three phases:
- Acute phase (infection): fever, chills, headache, myalgia, backache, nausea, vomiting, bradycardia
- Remission: brief improvement
- Toxic phase (~15% of cases): jaundice, renal failure, hemorrhage (hematemesis - "black vomit"), myocarditis; mortality 20-50%
Laboratory Diagnosis:
- Virus isolation: From blood (first 4 days); intracerebral inoculation of mice; cell culture
- Antigen detection: ELISA antigen capture, immunohistochemistry in tissue
- PCR (RT-PCR): Detects viral RNA in blood/tissue
- Serology:
- Anti-YF IgM (ELISA): Appears after viremia; diagnostic for recent infection
- Plaque Reduction Neutralization Test (PRNT): Most specific; confirms diagnosis
- IgG antibodies persist for years
- Histopathology (postmortem): Midzone necrosis, Councilman bodies, fatty change in liver
Prevention:
- Live attenuated vaccine 17D strain: Highly effective, single dose provides lifelong immunity; required for travel to endemic areas
- Vector control: eradication of Aedes aegypti breeding sites
CHAPTER 2 - PARASITIC INFECTIONS OF HEPATOBILIARY SYSTEM
CESTODES (TAPEWORMS)
Classification of Cestodes
Cestodes (tapeworms) are flat, ribbon-like, hermaphroditic helminths of the class Cestoda.
Classification:
Order Cyclophyllidea (most medically important):
| Species | Common Name | Intermediate Host | Definitive Host |
|---|
| Taenia solium | Pork tapeworm | Pig (cysticercus) | Human |
| Taenia saginata | Beef tapeworm | Cattle | Human |
| Echinococcus granulosus | Dog tapeworm/Hydatid | Sheep/cattle/humans | Dog |
| Echinococcus multilocularis | Alveolar hydatid | Rodents/humans | Fox |
| Hymenolepis nana | Dwarf tapeworm | None (direct) | Human |
| Diphyllobothrium latum | Fish tapeworm | Copepods + fish | Human |
Order Pseudophyllidea:
General Features of Cestodes:
- No alimentary canal - absorb nutrients through tegument
- Hermaphroditic - both male and female reproductive organs in each segment
- Scolex (head): attachment organ with suckers (and hooks in some)
- Neck: zone of proliferation
- Strobila: chain of proglottids
- Proglottids: segments - immature, mature, gravid (contain eggs)
- Life cycle requires two hosts (definitive + intermediate), except H. nana
ECHINOCOCCUS GRANULOSUS (HYDATID DISEASE / CYSTIC ECHINOCOCCOSIS)
Morphology
Adult worm (in dog intestine):
- 3-6 mm long; smallest tapeworm of medical importance
- Scolex: with 4 suckers + double row of hooklets (rostellum)
- Neck: short
- Strobila: only 3-4 proglottids: 1 immature + 1 mature + 1-2 gravid
- Gravid proglottid: contains 500-800 eggs
Eggs:
- Spherical, thick-walled, 30-40 μm
- Contain oncosphere (hexacanth embryo) with 6 hooklets
- Indistinguishable from Taenia eggs
Hydatid Cyst (larval stage in intermediate host/human):
- Unilocular fluid-filled cyst
- Three layers:
- Pericyst (Host layer) - outermost; fibrous layer derived from host tissue (compressed liver parenchyma)
- Ectocyst (Laminated/Outer layer) - middle; white, laminated, acellular, non-nucleated membrane; produced by the parasite
- Endocyst (Germinal/Inner layer) - innermost; single layer of nucleated germinal epithelium; gives rise to all internal structures
Internal structures of the hydatid cyst:
- Brood capsules: daughter cysts budding inward from the germinal layer; each contains protoscoleces (immature tapeworm heads with hooklets)
- Daughter cysts: smaller cysts within the main cyst
- Hydatid fluid: clear, colorless, under pressure; contains oncospheres and protoscoleces; antigenic and anaphylactogenic
- Hydatid sand: sediment at bottom of cyst fluid; contains free protoscoleces + hooklets + brood capsule fragments
Neat Labeled Diagram of Hydatid Cyst
┌──────────────────────────────┐
│ PERICYST (host fibrous wall) │
├──────────────────────────────┤
│ ECTOCYST (laminated membrane) │
├──────────────────────────────┤
│ GERMINAL LAYER (endocyst) │◄── produces all structures
│ ┌──────────────┐ │
│ │ Brood Capsule│ │
│ │ ┌──────────┐ │ │
│ │ │Protoscoleces│ │
│ │ │(with hooks)│ │ │
│ │ └──────────┘ │ │
│ └──────────────┘ │
│ [ Daughter Cysts ] │
│ [ Hydatid Fluid ] │
│ [ Hydatid Sand ] │
└──────────────────────────────┘
Life Cycle of E. granulosus
Dog (Definitive Host) ←────────────────────────────┐
↓ Adult worm in intestine │
↓ Gravid proglottids shed eggs in feces │
↓ │
Eggs ingested by intermediate host │
(sheep, cattle, pig, or HUMAN - accidental host) │
↓ Oncosphere hatches in small intestine │
↓ Penetrates intestinal wall │
↓ Travels via portal circulation → liver │
↓ (or lung, brain, bone, spleen rarely) │
↓ Forms HYDATID CYST (grows slowly over years) │
↓ │
Dog ingests raw viscera of infected sheep/cattle ───┘
(containing protoscoleces which develop into adult worms in dog intestine)
Humans are accidental intermediate hosts - infected by ingesting eggs from dog feces (hand-to-mouth, contaminated vegetables, water). The cycle does NOT continue because humans are not eaten by dogs (in most settings).
Pathogenesis
- Eggs ingested by human → oncosphere hatches in duodenum → penetrates gut wall → enters portal circulation
- Arrested in liver first (most common site, 60-70%)
- If passes liver → lungs (20-30%); rarely brain, bone, spleen
- Develops into hydatid cyst over months to years (slow-growing)
- Clinical manifestations depend on site, size, complications:
- Liver cyst: hepatomegaly, abdominal pain, obstructive jaundice (bile duct compression)
- Lung cyst: cough, chest pain, hemoptysis
- Cyst rupture (most dangerous):
- Spillage of antigenic cyst fluid → anaphylactic shock (life-threatening)
- Secondary seeding: daughter cysts implant and grow in peritoneum/other organs
- Hydatid fluid is extremely antigenic
Laboratory Diagnosis
1. Imaging:
- Ultrasound (USG): First-line; shows cystic lesion with daughter cysts, calcification, hydatid sand; WHO classification of cysts (CL, CE1-CE5)
- CT scan / MRI: Better anatomical detail, shows daughter cysts within mother cyst
- X-ray: May show calcified cyst (eggshell calcification)
2. Serology (Immunological tests):
- ELISA: Most sensitive; detects anti-Echinococcus antibodies (IgG); screening test
- Indirect Hemagglutination (IHA): Positive in ~80% of liver cysts
- Latex Agglutination Test (LAT)
- Casoni's Intradermal Test (Casoni's test): Injection of sterile hydatid cyst fluid intradermally
- Positive: wheal >5 mm at 20 minutes = hypersensitivity to hydatid antigens
- Sensitivity: 80%; many false positives and negatives; now largely replaced by serology
- Historically important but no longer widely used
3. Aspiration (PAIR procedure):
- Puncture, Aspiration, Injection, Re-aspiration - guided by ultrasound
- Aspirated fluid examined microscopically for protoscoleces and hooklets (diagnostic)
- Hydatid sand: scolex + hooks + brood capsule debris seen under microscope
- Risk of spillage limits its use to specialist centers
4. Indirect methods:
- Blood count: Eosinophilia (present in ~25% of patients; higher if cyst has leaked)
- Elevated ALP/GGT if biliary obstruction
5. Casoni's Test (detail):
- 0.2 mL sterile hydatid cyst fluid injected intradermally
- Read at 15-30 minutes: Immediate reaction (wheal + flare >5mm = positive)
- Read at 24-48 hours: Delayed reaction (induration = positive for cellular immunity)
- Sensitivity ~70-80% but lacks specificity (cross-reacts with other cestode infections)
Two key diagnostic tests to name:
- ELISA (most sensitive serological test)
- Casoni's intradermal test (classic, though now obsolete clinically)
INVASIVE (EXTRAINTESTINAL) AMOEBIASIS
Extraintestinal Manifestations of Amoebiasis
Entamoeba histolytica can spread beyond the intestine to cause:
- Amoebic Liver Abscess (ALA) - most common (accounts for ~50% of liver abscess cases)
- Route: portal bloodstream from large intestine → right lobe of liver preferentially
- "Anchovy sauce" pus (chocolate-brown fluid = liquefied hepatic tissue)
- Pleuropulmonary amoebiasis: direct extension from liver abscess through diaphragm
- Amoebic brain abscess: rare, hematogenous spread
- Cutaneous amoebiasis: perianal skin; rare
- Amoebic pericarditis: extension from left lobe liver abscess (rare, life-threatening)
Laboratory Diagnosis of Extraintestinal Amoebiasis / Amoebic Liver Abscess
1. Microscopy:
- Aspiration of liver abscess fluid: Examine for trophozoites at the wall of the abscess (not in the necrotic pus itself)
- Trophozoites with ingested red blood cells (erythrophagocytosis) seen on wet prep
- Yield is low (~10-40%); better from the last aspirated material
2. Serology (most useful for extraintestinal amoebiasis):
- ELISA / IFA (Immunofluorescence Assay): Most sensitive (~90-99%); detects anti-amoeba IgG antibodies
- Countercurrent Immunoelectrophoresis (CIE): Rapid, highly specific
- Indirect Hemagglutination Assay (IHA): Positive in >90% of ALA
- Latex Agglutination: Rapid, useful in field settings
- Note: Serology may be negative early in illness; repeat if initially negative
3. Antigen detection:
- ELISA for Gal/GalNAc lectin antigen in serum (highly specific for E. histolytica)
- Fecal antigen ELISA: for intestinal amoebiasis; not useful for ALA
4. Molecular diagnosis:
- PCR (stool, biopsy): Differentiates E. histolytica from non-pathogenic E. dispar and E. moshkovskii (morphologically identical)
- Most specific available test
5. Imaging:
- Ultrasound: First-line; ALA appears as hypoechoic lesion in right lobe of liver
- CT/MRI: Better characterization; round/oval lesion with peripheral enhancement ("ring sign")
6. Stool examination (for intestinal amoebiasis):
- Direct wet mount: Trophozoites with ingested RBCs (diagnostic), or cysts
- Iodine preparation: Better visualization of cysts (4 nuclei in E. histolytica)
- Culture (Jones' medium / Robinson's medium): rarely done clinically
- Biopsy of colonic ulcer: shows "flask-shaped" ulcers with trophozoites
7. Complete blood count:
- Leukocytosis (neutrophilia)
- Elevated ESR, CRP
- Elevated serum ALP (liver involvement)
LIVER FLUKES - ENUMERATION
Liver flukes are trematodes (flukes) that infect the biliary system:
| Species | Common Name | Intermediate Hosts | Final Host |
|---|
| Fasciola hepatica | Liver fluke (sheep liver rot) | Snail (Lymnaea) + water vegetation | Sheep, cattle, humans |
| Fasciola gigantica | Giant liver fluke | Snail + aquatic plants | Cattle, buffaloes, humans |
| Clonorchis sinensis | Chinese/Oriental liver fluke | Snail + freshwater fish | Humans, dogs, cats |
| Opisthorchis viverrini | Southeast Asian liver fluke | Snail + freshwater fish | Humans, cats |
| Opisthorchis felineus | Cat liver fluke | Snail + freshwater fish | Cats, humans |
| Dicrocoelium dendriticum | Lancet fluke | Land snail + ants | Sheep, cattle, humans (rare) |
LARVA MIGRANS
Larva migrans refers to the prolonged migration of larval helminths through human tissues, as humans are dead-end/aberrant hosts.
1. Cutaneous Larva Migrans (CLM) - "Creeping Eruption"
Causative agents: Ancylostoma braziliense (most common), A. caninum, Uncinaria stenocephala
- Larvae from cat/dog hookworms penetrate human skin
- Unable to complete life cycle in humans → migrate in dermis creating serpiginous (snake-like), intensely itchy tracks
- Diagnosis: Clinical; skin biopsy; serology
- Treatment: Albendazole or ivermectin
2. Visceral Larva Migrans (VLM)
Causative agents: Toxocara canis (dog roundworm) most common; T. cati (cat roundworm)
Route: Ingestion of Toxocara eggs from contaminated soil (geophagia, contact with dogs)
Pathogenesis: Larvae hatch in intestine → penetrate gut wall → migrate hematogenously → arrested in tissues (liver, lungs, eye, brain) → eosinophilic granulomas form around larvae
Clinical features:
- Systemic VLM: Hepatomegaly (most common), fever, cough, wheeze (pulmonary infiltrates), urticaria
- Ocular Larva Migrans (OLM): Larvae in eye → endophthalmitis, granuloma, retinal damage, can mimic retinoblastoma
- Covert/Common toxocariasis: Mild symptoms in older children; abdominal pain, neurological symptoms
Diagnosis:
- Eosinophilia (prominent, often >30%)
- Serology: ELISA for anti-Toxocara antibodies (larval excretory-secretory [ES] antigens; highly sensitive and specific)
- Imaging: Liver USG/CT - multiple small hypodense lesions
- Ophthalmic examination (for OLM)
- Liver biopsy (rarely needed): eosinophilic granulomas with larvae
Treatment: Albendazole or mebendazole; corticosteroids for severe disease/OLM
3. Neural Larva Migrans
- Baylisascaris procyonis (raccoon roundworm): causes fatal eosinophilic meningoencephalitis
SOURCES
- Medical Microbiology 9e (Murray, Rosenthal & Pfaller)
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Edition
- Robbins & Kumar Basic Pathology