Hodgkins lymphoma
Reading File
Finding Sources
Searching PubMed
"Hodgkin lymphoma"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it.
Hodgkin Lymphoma
Overview
Hodgkin lymphoma (HL) is a B-cell malignancy distinguished from all other lymphomas by the presence of Reed-Sternberg (RS) cells set within a background of reactive inflammatory infiltrate. Despite arising from neoplastic cells, those tumor cells make up only a small fraction of the total tumor mass - the bulk is reactive host tissue. It carries one of the best prognoses of any malignancy, with cure achievable in the majority of patients. - Robbins & Kumar Basic Pathology, p. 417
Epidemiology
-
Incidence: ~2.7 per 100,000 in North America; approximately 30,000 new cases annually in North America and Europe
-
Bimodal age distribution: early peak at ages 25-30 years, later peak after age 50
-
Slightly more common in men; higher rates in Whites and higher socioeconomic groups
-
Lifetime risk approximately 1 in 250-300 in North America
-
Low incidence in East Asia; in the Indian subcontinent, the age distribution shifts strongly into childhood
-
Goldman-Cecil Medicine, p. 1964
Pathogenesis & Etiology
Cell of origin: RS cells derive from germinal center B cells. This was proven by microdissection studies showing identical, somatically hypermutated immunoglobulin gene rearrangements in every RS cell within a given tumor. Despite this B-cell origin, classic RS cells paradoxically lose most B-cell surface markers. - Robbins & Kumar, p. 417
Epstein-Barr Virus (EBV):
- EBV is identified in RS cells in ~50% of all HL cases (up to 70% in the mixed-cellularity subtype)
- A history of infectious mononucleosis increases HL risk approximately 3-fold
- Integration site is identical in all RS cells per case, confirming infection precedes clonal expansion
- Anti-EBV antibodies appear several years before tumor development
- EBV is likely one of several oncogenic steps, not the sole cause
Immune evasion: Classic HL escapes immune surveillance by:
- Loss of beta-2 microglobulin → failure to express MHC class I molecules (hiding from cytotoxic T cells)
- High-level expression of PD-L1 and PD-L2 (immune checkpoint ligands) - often due to amplification of chromosome 9p region
- This PD-1/PD-L1 axis is clinically exploitable: anti-PD-1 antibodies produce responses even in chemotherapy-resistant disease
Cytokine milieu: RS cells secrete IL-5 (eosinophil recruitment), TGF-β (fibrosis), and IL-13 (autocrine growth). The reactive inflammatory cells in turn produce factors that feed back to support RS cell growth.
- Robbins & Kumar, pp. 417-419
Reed-Sternberg Cell - The Diagnostic Hallmark
The RS cell is a very large cell (15-45 µm diameter) with:
- An enormous multilobate nucleus or two mirror-image nuclei/lobes
- Exceptionally prominent nucleoli (inclusion-like, acidophilic), surrounded by a clear halo - the classic "owl-eye" appearance
- Abundant eosinophilic cytoplasm
Immunophenotype of classic RS cells:
- Positive: CD15, CD30
- Negative: CD45 (leukocyte common antigen), B-cell markers (CD20), T-cell markers
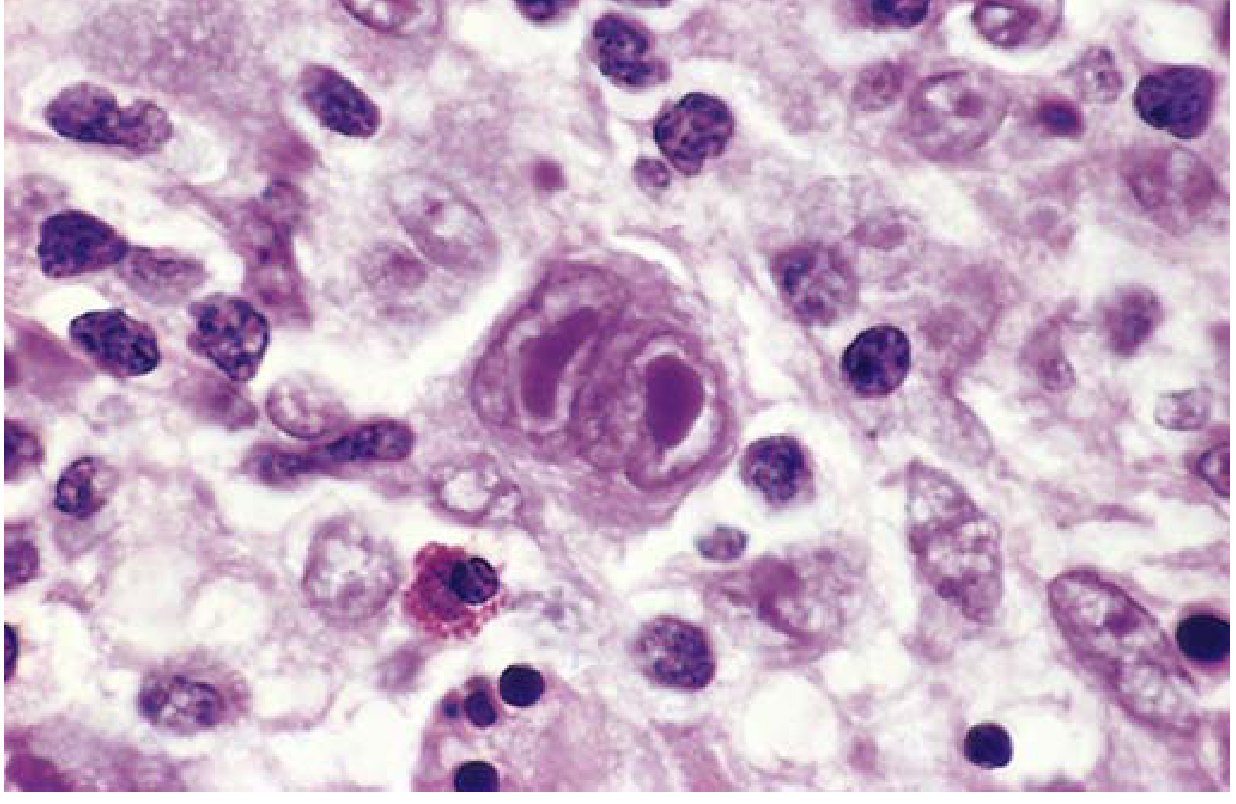
Classic Reed-Sternberg cell with its large multilobate nucleus and prominent nucleoli, surrounded by reactive lymphocytes and eosinophils. - Robbins & Kumar Basic Pathology
- Robbins & Kumar, p. 418
Classification - Five Subtypes
Classic Hodgkin Lymphoma (~90% of cases)
Shares the RS immunophenotype (CD15+, CD30+, CD45-) across four subtypes:
| Subtype | Frequency | Key Features | Demographics |
|---|---|---|---|
| Nodular Sclerosis | Most common (60-70%) | Lacunar cell variant; collagen bands dividing tissue into nodules; fibrosis | Equal M:F; adolescents/young adults; mediastinal, cervical, supraclavicular nodes |
| Mixed Cellularity | 20-25% | Classic RS cells; EBV+ in ~70%; eosinophils, plasma cells, macrophages | Older adults; more advanced stage at presentation |
| Lymphocyte Rich | ~5% | Rare RS cells; lymphocyte-predominant background | Good prognosis |
| Lymphocyte Depleted | Rare (<1%) | Abundant RS cells, sparse lymphocytes; often EBV+ | Advanced stage; worst prognosis among classic subtypes |
Nodular Lymphocyte-Predominant HL (~10% of cases)
-
Distinct entity: RS cell variants ("popcorn cells" or LP cells) express germinal center B-cell markers including CD20, CD79a
-
CD15 negative, CD30 negative (key distinction from classic HL)
-
Indolent course; excellent prognosis; late relapses possible
-
Robbins & Kumar, p. 417; Goldman-Cecil Medicine, p. 1963
Clinical Features
Typical presentation:
- Painless lymphadenopathy - most commonly cervical, supraclavicular, or axillary
- Mediastinal involvement is very common (especially nodular sclerosis subtype) - may cause cough, dyspnea, or superior vena cava syndrome
- Disease spreads in a predictable, contiguous fashion through lymph node groups - unlike non-Hodgkin lymphoma
B Symptoms (prognostically significant):
- Fever (>38°C)
- Drenching night sweats
- Unexplained weight loss >10% body weight in 6 months
Other features:
-
Pruritis (can be severe)
-
Pel-Ebstein fever - cyclical fever pattern (classic but uncommon)
-
Alcohol-induced pain at nodal sites (characteristic but rare)
-
Splenomegaly in advanced disease
-
Goldman-Cecil Medicine, p. 1964
Staging - Modified Ann Arbor System
| Stage | Definition |
|---|---|
| I | Single lymph node region (I) or one extralymphatic site (IE) |
| II | Two or more lymph node regions, same side of the diaphragm (II), or local extralymphatic extension (IIE) |
| III | Lymph node regions on both sides of the diaphragm; may include spleen (IIIS) |
| IV | Diffuse extralymphatic involvement (bone marrow, liver, lung, etc.) |
Suffix A = no B symptoms; suffix B = B symptoms present
Bulky disease: mediastinal mass >1/3 of thoracic diameter, or any nodal mass >10 cm
Workup / Staging Evaluation
-
Complete history (B symptoms, bone pain, other localizing symptoms)
-
Physical examination for lymphadenopathy, organomegaly
-
CBC, ESR, serum creatinine, alkaline phosphatase, LDH, bilirubin, albumin, protein electrophoresis
-
HIV and hepatitis B/C serology
-
Chest X-ray (PA and lateral)
-
Contrast-enhanced CT scan of neck, thorax, abdomen, and pelvis
-
FDG-PET/CT - now standard; more sensitive and specific than CT alone; has replaced bone marrow biopsy for staging
-
Excisional lymph node biopsy for histological diagnosis
-
Goldman-Cecil Medicine, p. 1965
Treatment
Early-Stage (I-II, non-bulky) - Favorable
- ABVD x 2-4 cycles followed by involved-site radiation therapy (ISRT) - the standard backbone
- ABVD = Adriamycin (doxorubicin) + Bleomycin + Vinblastine + Dacarbazine
- PET-adapted therapy: if PET is negative after 2 cycles of ABVD, radiation may be omitted in selected patients; if PET positive, escalation to BEACOPP is considered
Early-Stage with Unfavorable Features or Bulky Disease
- ABVD x 4-6 cycles + ISRT, or
- BEACOPP-based regimens
Advanced-Stage (III-IV)
Current standard (replacing ABVD):
- A+AVD = Brentuximab vedotin + Doxorubicin + Vinblastine + Dacarbazine
- Brentuximab vedotin is an anti-CD30 antibody-drug conjugate
- Shown to improve 5-year progression-free and overall survival vs. ABVD in stage III/IV disease
- Now considered standard of care for previously untreated advanced HL
Alternative (ABVD-based):
- ABVD x 6 cycles; if PET negative after 2 cycles, bleomycin can be safely omitted
- Escalated BEACOPP (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone) - superior initial disease control but no proven overall survival benefit over ABVD in randomized trials; used for high-risk patients under age 60
PET-guided therapy is central to modern management - end-of-treatment PET distinguishes residual fibrosis (75% of residual masses) from persistent lymphoma.
- Goldman-Cecil Medicine, p. 1965
Relapsed / Refractory Disease
For most patients with relapsed or refractory HL:
- Salvage chemotherapy (e.g., BEAM - carmustine, etoposide, cytarabine, melphalan)
- High-dose chemoradiation + autologous hematopoietic stem cell transplant (ASCT)
- Approximately 1/3 of refractory patients and 2/3 of relapsed patients can be cured
- Consolidative brentuximab vedotin post-ASCT reduces relapse rate by ~1/3
Post-ASCT relapse - checkpoint inhibitors:
-
Nivolumab (anti-PD-1) and pembrolizumab (anti-PD-1) produce high response rates (60-70%) even in multiply relapsed/refractory HL, exploiting the PD-L1/PD-L2 overexpression on RS cells
-
Some patients achieve durable remissions; role as bridge to allogeneic transplant is evolving
-
Goldman-Cecil Medicine, pp. 1965-1966
Prognosis
- Early-stage disease (I-II): cure rate >90% with combined modality therapy
- Advanced-stage (III-IV): 5-year overall survival ~80-85% with modern regimens
- International Prognostic Score (IPS) for advanced HL - 7 adverse factors: albumin <4 g/dL, hemoglobin <10.5 g/dL, male sex, age ≥45, stage IV, leukocytosis (WBC ≥15,000), lymphopenia (<600/µL or <8% of WBC)
- Long-term complications of treatment (secondary malignancies, cardiotoxicity from anthracyclines, pulmonary toxicity from bleomycin, hypothyroidism from neck radiation) are a major focus of modern treatment design
Key Distinguishing Points vs. Non-Hodgkin Lymphoma
| Feature | Hodgkin Lymphoma | Non-Hodgkin Lymphoma |
|---|---|---|
| RS cells | Present (pathognomonic) | Absent |
| Spread pattern | Contiguous, predictable | Non-contiguous, unpredictable |
| Mediastinal involvement | Common | Less common (except some subtypes) |
| Bone marrow/liver/GI | Uncommon early | Frequent |
| Curability | Very high (most stages) | Varies widely by subtype |
| B-cell origin | Yes (though markers often lost) | Yes (mostly) |
Sources:
- Robbins & Kumar Basic Pathology, Chapter 10, pp. 417-419
- Goldman-Cecil Medicine, Chapter 172 (Connors JM, Savage KJ)
Make it more lucid.
Hodgkin Lymphoma
What Is It?
Hodgkin lymphoma (HL) is a cancer of B lymphocytes that almost always starts in lymph nodes. What makes it unique among lymphomas is the presence of a bizarre giant cell - the Reed-Sternberg (RS) cell - sitting in a sea of normal-looking inflammatory cells. Paradoxically, those tumor cells are actually the minority in the tumor mass; most of what you see under the microscope is a reactive host response that fails to eliminate the cancer.
The good news: HL is one of the most curable cancers in medicine, with >90% cure rates in early-stage disease.
Who Gets It?
- Affects roughly 1 in 250-300 people over a lifetime
- Classic bimodal age curve: first peak in young adults (ages 25-30), second peak after age 50
- Slightly more common in men
- Higher rates in developed countries, White populations, and higher socioeconomic groups
- Rare in East Asia; when it does occur in South Asia, it tends to affect children rather than young adults
Why Does It Happen?
The short answer: we don't fully know, but there are two major clues.
1. The cell of origin
RS cells come from germinal center B cells - the B cells normally busy refining antibody quality. Something goes wrong during this process and the cell transforms. Despite being B cells, classic RS cells paradoxically lose their B-cell surface markers, which is one reason it took so long to figure out their origin.
2. Epstein-Barr Virus (EBV)
- EBV (the virus behind mono/glandular fever) is found inside RS cells in about 50% of cases - up to 70% in the mixed-cellularity subtype
- Having had infectious mononucleosis triples your subsequent risk of HL
- Anti-EBV antibodies appear in the blood years before the tumor, suggesting EBV is an early contributor, not a bystander
- EBV is probably one step on the path to transformation, not the sole cause
How does the tumor hide from the immune system?
RS cells are clever at evasion:
- They shed their MHC class I molecules (the flag that lets killer T cells recognize and attack them) by losing beta-2 microglobulin
- They overexpress PD-L1 and PD-L2 - immune checkpoint proteins that put the brakes on T-cell activity, essentially telling the immune system "stand down"
- This PD-L1 overexpression turns out to be their Achilles heel - anti-PD-1 drugs (checkpoint inhibitors) can lift that brake and reawaken the immune response even in heavily treated disease
The Reed-Sternberg Cell - What to Look For
The RS cell is enormous (15-45 µm - several times the size of a normal lymphocyte) with:
- A huge multilobate nucleus - or two mirror-image nuclei side by side
- Giant, prominent nucleoli surrounded by a clear halo
- The classic look: two nuclei each staring back at you like a pair of eyes - the "owl-eye" appearance
How to identify them on immunostaining (classic HL):
| Marker | Result | Memory hook |
|---|---|---|
| CD30 | Positive | CD30 = the "target" for brentuximab |
| CD15 | Positive | |
| CD45 | Negative | Unusual - most lymphoid cells are CD45+ |
| CD20 / B-cell markers | Negative | Paradoxical for a B-cell tumor |
| CD3 / T-cell markers | Negative |
The Five Subtypes
Classic HL (~90% of all HL)
All share the CD15+/CD30+/CD45- RS immunophenotype.
Nodular Sclerosis - the most common subtype (60-70%)
- Thick collagen bands divide the lymph node into nodules
- RS cell variant here is the lacunar cell - looks like it's sitting in an empty space (lacune) because the cytoplasm retracts in formalin fixation
- Loves the mediastinum, lower cervical, and supraclavicular nodes
- Typical patient: adolescent or young adult; equal male-to-female ratio
- Excellent prognosis
Mixed Cellularity (~20-25%)
- Classic owl-eye RS cells are abundant
- Most strongly linked to EBV (~70% positive)
- Background is a rich mix - eosinophils, plasma cells, macrophages, lymphocytes
- More common in older adults; often presents at a later stage
Lymphocyte Rich (~5%)
- RS cells are sparse in a sea of lymphocytes
- Good prognosis
Lymphocyte Depleted (rare, <1%)
- RS cells are abundant, lymphocytes are few
- Worst prognosis among classic subtypes; often EBV-positive; tends to present at advanced stage
Nodular Lymphocyte-Predominant HL (~10%)
This is a fundamentally different disease that just happens to share the "Hodgkin" name:
- The neoplastic cells are called LP cells ("popcorn cells") - with a folded, lobulated nucleus
- They retain germinal center B-cell markers: CD20+, CD79a+
- They are CD15 negative, CD30 negative - the opposite of classic HL
- Indolent course; excellent long-term prognosis; can relapse late but usually responds again to treatment
Clinical Presentation
The classic patient: a young adult with painless, rubbery lymph node swelling - most often in the neck or above the collarbone. It has been there for weeks to months, slowly growing.
What else to look for:
- B symptoms (important for staging and prognosis):
- Fever >38°C
- Drenching night sweats
- Weight loss >10% over 6 months
- Mediastinal mass - cough, breathlessness, or superior vena cava obstruction (facial swelling, dilated neck veins)
- Pruritis - can be severe and is often underappreciated
- Pel-Ebstein fever - a cyclical fever pattern; classic but uncommon
- Alcohol-induced pain at nodal sites - rare but almost pathognomonic for HL
How it spreads: HL spreads in an orderly, contiguous step-by-step fashion through adjacent lymph node groups. This predictability is one reason it responds so well to radiation, and it distinguishes HL from non-Hodgkin lymphomas, which spread non-contiguously.
Staging - The Ann Arbor System
Think of the diaphragm as the dividing line:
| Stage | Meaning |
|---|---|
| I | One lymph node region only |
| II | Two or more regions, but all on the same side of the diaphragm |
| III | Regions on both sides of the diaphragm |
| IV | Spread into organs (bone marrow, liver, lung) |
Add A if no B symptoms, B if B symptoms are present (e.g., "Stage IIB").
Bulky disease: a mediastinal mass >1/3 the thoracic diameter, or any mass >10 cm - treated more aggressively regardless of stage.
Workup
| Test | Why |
|---|---|
| Excisional lymph node biopsy | Definitive histological diagnosis |
| CBC, ESR, LDH, albumin, liver/renal function | Baseline and prognostic markers |
| HIV, hepatitis B/C serology | Before immunosuppressive chemotherapy |
| Contrast CT (neck/chest/abdomen/pelvis) | Anatomical staging |
| FDG-PET/CT | Now standard; more sensitive than CT; has replaced bone marrow biopsy |
PET is central to modern HL management - not just for initial staging, but for mid-treatment response assessment that can guide whether to intensify or de-escalate therapy.
Treatment
Early-Stage (I-II, non-bulky)
ABVD x 2-4 cycles + involved-site radiotherapy (ISRT)
ABVD is the standard chemotherapy backbone:
- A - Adriamycin (doxorubicin)
- B - Bleomycin
- V - Vinblastine
- D - Dacarbazine
Modern practice is PET-adapted: if PET is negative after 2 cycles of ABVD, radiation can sometimes be safely omitted. If PET remains positive, treatment is escalated.
Advanced-Stage (III-IV)
The standard has recently shifted away from ABVD alone.
Current standard: A+AVD
- Brentuximab vedotin (anti-CD30 antibody-drug conjugate) + Adriamycin + Vinblastine + Dacarbazine
- Brentuximab delivers a cytotoxic payload directly to CD30+ RS cells
- Proven to improve both progression-free and overall survival vs. ABVD in stage III/IV HL
Alternative: escalated BEACOPP (for younger, fit patients)
- Bleomycin, Etoposide, Adriamycin, Cyclophosphamide, Oncovin (vincristine), Procarbazine, Prednisone
- Better initial disease control but no proven overall survival advantage over ABVD in randomized trials
End-of-treatment PET distinguishes residual fibrosis (in ~75% of residual masses) from active disease - critical for deciding who needs consolidation radiation.
Relapsed or Refractory Disease
Step 1: Salvage chemotherapy (e.g., BEAM regimen)
Step 2: High-dose chemoradiation + autologous stem cell transplant (ASCT)
- Cures ~1/3 of refractory patients and ~2/3 of those who relapse after primary therapy
Step 3 (post-ASCT): Consolidative brentuximab vedotin - reduces further relapse by about one third
Step 4 (post-ASCT relapse): Checkpoint inhibitors
- Nivolumab or pembrolizumab (anti-PD-1 antibodies) achieve 60-70% response rates by reactivating the T-cell response that RS cells had suppressed via PD-L1/PD-L2
- Some patients achieve durable remissions; can bridge to allogeneic transplant
Prognosis
| Stage | Approximate Cure Rate |
|---|---|
| Early (I-II, favorable) | >90% |
| Early (I-II, unfavorable/bulky) | ~85% |
| Advanced (III-IV) | ~80-85% with modern regimens |
International Prognostic Score (IPS) for advanced HL - one point each for:
- Albumin <4 g/dL
- Hemoglobin <10.5 g/dL
- Male sex
- Age ≥45
- Stage IV disease
- Leukocytosis (WBC ≥15,000)
- Lymphopenia (<600/µL or <8% of WBC)
Score 0-1 = ~85% 5-year freedom from progression; score ≥5 = ~55%
Long-term survivorship issues are a growing concern given how many patients are cured young - secondary malignancies (breast cancer after chest radiation, leukemia after alkylating agents), cardiomyopathy from doxorubicin, pulmonary fibrosis from bleomycin, and hypothyroidism after neck radiation. Modern treatment design actively tries to minimize these risks.
HL vs. Non-Hodgkin Lymphoma - At a Glance
| Hodgkin | Non-Hodgkin | |
|---|---|---|
| Reed-Sternberg cells | Always present | Absent |
| Spread pattern | Orderly, contiguous | Unpredictable, skips nodes |
| Mediastinum | Commonly involved | Less common |
| Bone marrow / GI tract | Rare early on | Frequently involved |
| Curability | Very high across stages | Highly variable by subtype |
Sources: Robbins & Kumar Basic Pathology, Chapter 10, pp. 417-419; Goldman-Cecil Medicine, Chapter 172 (Connors JM, Savage KJ)
This is a shared conversation. Sign in to Orris to start your own chat.