Superficial and invasive fungal infections diagnosis and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
fungal infections diagnosis treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive material to compile a thorough, well-structured answer. Let me synthesize everything from these authoritative sources.
Fungal Infections: Diagnosis and Treatment
Overview and Classification
Mycoses are divided into three depth-based categories:
- Superficial - confined to the stratum corneum, hair, and nails
- Subcutaneous - involving the dermis and subcutaneous tissue
- Deep/Systemic (Invasive) - hematogenous spread, including opportunistic infections in immunocompromised hosts
- Fitzpatrick's Dermatology, Vol. 1-2, p. 2956
- Harrison's Principles of Internal Medicine 22E, p. 1766
Part I: Superficial Fungal Infections
A. Dermatophytoses (Tinea Infections)
Dermatophytes are molds in three genera - Trichophyton, Microsporum, and Epidermophyton - that live within keratinized structures. They are classified by ecological niche:
- Anthropophilic (human-to-human): T. rubrum, T. tonsurans, T. interdigitale, Epidermophyton floccosum
- Zoophilic (animal-to-human): T. mentagrophytes (rodents), Microsporum canis (cats/dogs)
- Geophilic (soil): M. gypseum
T. rubrum is the most common cause of dermatophytosis in the US; T. tonsurans is the leading cause of tinea capitis in the US.
Globally, an estimated 1 billion people are affected by dermatophyte infections.
Clinical Syndromes
| Infection | Site | Key Features |
|---|---|---|
| Tinea capitis | Scalp | Children 3-7 yrs; patchy alopecia, scaling, hair shafts broken above skin; kerion = severe inflammatory reaction |
| Tinea corporis | Body | Annular, pruritic, well-demarcated plaque with central clearing and raised scaling border; centrifugal growth |
| Tinea cruris | Groin | Obese adult males; erythematous rash, scaly border, no satellite lesions; pruritic |
| Tinea pedis | Feet ("athlete's foot") | 30-40% lifetime prevalence; web space maceration, scaling, can lead to lower-limb cellulitis via skin fissures |
| Tinea unguium / Onychomycosis | Nails | Thickening, discoloration, crumbling, onycholysis; toenails >> fingernails; risk: DM, vascular disease, elderly |
| Tinea barbae | Beard | Uncommon; adult males only |
- Harrison's, p. 1767; Robbins & Cotran Pathologic Basis of Disease, p. 1078
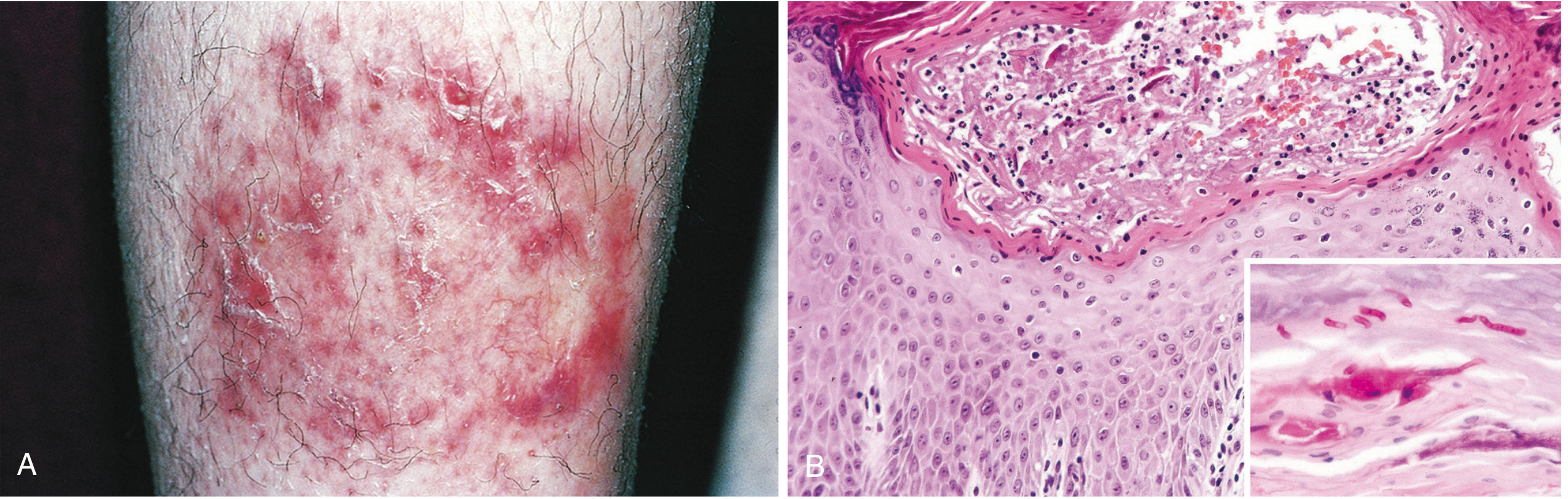
Histopathology
Fungi stain bright pink-red with Periodic Acid-Schiff (PAS) stain (cell walls rich in mucopolysaccharides). They are confined to the anucleate cornified layer. The histologic pattern is variable: mild eczematous (spongiotic) dermatitis with intraepidermal neutrophils and focal neutrophilic abscesses.
Diagnosis
- KOH preparation: Scraping from the active border of a lesion dissolved in KOH reveals septate hyphae - the gold-standard bedside test
- Wood's lamp: Microsporum species fluoresce green-yellow; T. tonsurans (most common US tinea capitis) does NOT fluoresce
- Culture: Sabouraud's dextrose agar (SDA); definitive for speciation; urease test differentiates T. interdigitale (positive) from T. rubrum (negative)
- Histopathology with PAS or GMS stain: For nail clippings
- Clinical appearance is sufficient for most typical cases
Treatment
Topical (most skin infections):
- Azoles (clotrimazole, miconazole, ketoconazole, econazole) or terbinafine cream
- Apply for 2-4 weeks; lotions/sprays preferred for hairy/large areas
- Tinea cruris: keep area dry
Oral (hair-bearing areas, nails, extensive disease):
| Indication | Agent | Dose/Duration |
|---|---|---|
| Tinea capitis | Griseofulvin or terbinafine | 6-8 weeks |
| Extensive tinea corporis/cruris/pedis | Terbinafine | 250 mg/day × 1-2 weeks |
| Extensive tinea (alternative) | Itraconazole | 200 mg/day × 1-2 weeks |
| Onychomycosis | Terbinafine | 250 mg/day × 3 months (fingernails); 6 months (toenails) |
| Onychomycosis (alternative) | Itraconazole | 200 mg/day × 3 months OR pulse 200 mg twice daily × 1 week/month × 3 months |
| Onychomycosis (topical option) | Efinaconazole topical solution | Applied to nail for up to 1 year |
Terbinafine interacts with fewer drugs than itraconazole and is generally first-line for systemic therapy. Both require monitoring for hepatotoxicity.
- Harrison's, pp. 1767, TABLE 225-1
B. Malassezia Infections
Agents: Malassezia furfur, M. pachydermatis - lipophilic yeasts, part of normal skin microbiota in sebaceous areas.
Clinical presentations:
- Tinea versicolor (pityriasis versicolor): Hypo- or hyperpigmented scaly macules on neck/chest/upper arms; may be confused with vitiligo (which lacks scale)
- Malassezia folliculitis: Papulopustules on back and chest mimicking bacterial folliculitis
- Seborrheic dermatitis: Erythematous, pruritic, scaly lesions in eyebrows, nasolabial folds, scalp (dandruff); severe in AIDS
Diagnosis: Clinical; KOH prep shows "spaghetti and meatballs" pattern - short hyphae + budding bottle-shaped yeasts. Culture requires olive oil overlay.
Treatment:
- Topical: selenium sulfide shampoo, ketoconazole shampoo/cream, terbinafine cream × 2 weeks
- Extensive disease: oral itraconazole or fluconazole 200 mg/day × 5-7 days
- Mild steroids for seborrheic dermatitis
- Rare fungemia (premature neonates on parenteral lipids): AmB or voriconazole + remove central catheter + stop lipid infusion
C. Mucocutaneous Candidiasis
Key organisms: C. albicans, C. tropicalis, C. glabrata, C. parapsilosis
Clinical forms:
- Oral thrush: White removable plaques; severity proportional to immune status
- Esophageal candidiasis: Always treat systemically
- Vulvovaginal candidiasis (VVC): Whitish discharge, pruritus, erythema
- Cutaneous candidiasis: Intertriginous areas, diaper dermatitis, paronychia
Diagnosis:
- Oral: Clinical appearance; scraping reveals yeasts + pseudohyphae
- VVC: Wet prep or culture of vaginal secretions
- Biopsy shows yeasts/pseudohyphae invading epithelium (colonization shows yeasts only superficial to epithelium)
Treatment:
- Mild oral thrush: Nystatin suspension "swish and swallow," or clotrimazole troches 10 mg 4-5× daily × 7-14 days
- Moderate/severe or AIDS-related thrush: Oral fluconazole 100-200 mg/day × 7-14 days
- VVC: Topical azoles (miconazole, clotrimazole) or oral fluconazole 150 mg single dose; recurrent VVC requires chronic suppression with fluconazole
- Newer agents for VVC: Ibrexafungerp (triterpenoid, inhibits β-glucan; 300 mg twice daily × 1 day); oteseconazole (long-acting tetrazole - NOT for patients of reproductive potential due to fetal ocular toxicity)
- Esophageal candidiasis: Fluconazole 200 mg/day × 14 days
D. Subcutaneous Mycoses
Sporotrichosis (Sporothrix schenckii)
- Inoculation from soil/plants (rose thorn, sphagnum moss)
- Fixed cutaneous form: itraconazole × 3-6 months
- Lymphocutaneous form: itraconazole 200 mg/day × 3-6 months; supersaturated potassium iodide is an alternative
- Pulmonary/osteoarticular: Itraconazole × ≥1 year
- Severe/disseminated/CNS: AmB induction → itraconazole step-down; lifelong suppression in AIDS
Eumycetoma (Madura Foot)
- Chronic swelling, sinus tracts, discharge of grains (fungal colonies)
- Mainly lower extremities, can involve bone
- Diagnosis: biopsy + culture (to distinguish from actinomycetoma)
- Treatment: Itraconazole ± surgical debridement; high recurrence rates
Chromoblastomycosis
- Nodular/verrucous lesions on lower extremities; indolent growth over years
- Risk: squamous cell carcinoma in chronic lesions
- Diagnosis: "copper pennies" (muriform cells) on histology
- Treatment: Itraconazole ± cryotherapy; resistant cases add terbinafine
Part II: Invasive/Systemic Fungal Infections
A. Invasive Candidiasis
Risk factors: ICU stay, central venous catheters, broad-spectrum antibiotics, total parenteral nutrition, hematologic malignancy, neutropenia, immunosuppression, renal replacement therapy.
Diagnosis
- Blood cultures: Standard but only 50% sensitive; 1-4 days to positivity - problematic in critically ill patients
- β-D-glucan: Cell wall component of most fungi (not Cryptococcus or Mucor); moderately sensitive in high-risk patients; NOT Candida-specific
- PCR: More sensitive than β-D-glucan and cultures but not yet standardized
- Funduscopic exam: Mandatory in all candidemic patients - classic white retinal lesions indicate dissemination
- Imaging: CT/MRI for chronic disseminated candidiasis (multiple hepatosplenic lesions)
- Biopsy: Focal lesions (skin, liver); Gram stain or silver stain for yeasts
- Catheter tips should be cultured; any yeast growth is treated
Treatment
Mucocutaneous disease: (see above)
Candidemia/Invasive candidiasis:
- First-line: Echinocandin - caspofungin 50 mg/day, micafungin 100 mg/day, or anidulafungin 100 mg/day (preferred in all critically ill patients including neutropenic)
- Alternative: Fluconazole 400-800 mg/day only for non-severely ill, low-resistance-risk patients
- Step-down: Fluconazole after clinical stability if isolate (e.g., C. albicans) is susceptible
- Duration: At least 2 weeks after first negative blood culture
- Remove central venous catheters whenever feasible - accelerates clearance
- Voriconazole, AmB, and lipid AmB are alternatives
Candida endocarditis:
- Lipid AmB 3-5 mg/kg/day × 6 weeks ± flucytosine 25 mg/kg qid
- Valve replacement mandatory; lifelong fluconazole suppression if surgery not possible
Empirical therapy (febrile, critically ill with risk factors): Echinocandin preferred; reserved for those with Candida colonization + organ failure + broad-spectrum antibiotics
- Goldman-Cecil Medicine, pp. 3365-3403
B. Invasive Aspergillosis
Key organism: Aspergillus fumigatus (most common), A. flavus, A. terreus, A. niger
Risk factors: Prolonged neutropenia, allogeneic HSCT, solid organ transplant, high-dose corticosteroids, biologic immunosuppressants, CGD (Chronic Granulomatous Disease)
Clinical forms:
- Invasive pulmonary aspergillosis (IPA): Most common; fever, cough, pleuritic chest pain, hemoptysis
- Tracheobronchitis
- Sinusitis: Acute invasive (immunocompromised); chronic invasive (diabetics/mild immune defects)
- Disseminated: Brain, heart, kidneys, liver
Diagnosis:
- CT chest: Halo sign (ground-glass halo around nodule - early neutropenic) → Air-crescent sign (late, recovering neutropenia)
- Galactomannan (GM) assay: Serum or BAL; sensitivity higher in BAL; false positives with piperacillin-tazobactam, certain foods
- β-D-glucan: Positive in aspergillosis; less specific
- Bronchoscopy + BAL: Cytology, culture, GM from lavage
- Tissue biopsy: Definitive - shows acute-angle branching (45°), septate hyaline hyphae on Grocott-Gomori methenamine silver (GMS) stain
Treatment:
- First-line: Voriconazole (IV or oral; therapeutic drug monitoring required - target trough 1-5.5 mcg/mL)
- Alternatives: Isavuconazole (better tolerated, less drug interactions), liposomal AmB 3-5 mg/kg/day
- Salvage: Posaconazole, combination voriconazole + echinocandin (for refractory cases)
- Duration: Minimum 6-12 weeks, guided by response and immune recovery
- Surgical debridement for invasive sinusitis or single accessible pulmonary lesion
C. Mucormycosis
Key organisms: Rhizopus, Mucor, Cunninghamella (Mucorales)
Risk factors: Uncontrolled diabetes (especially DKA), hematologic malignancy, iron overload, deferoxamine therapy, corticosteroids
Distinguishing pathology: Aseptate (sparsely septate) hyphae with wide, ribbon-like morphology; angioinvasion causing thrombosis and tissue infarction
Clinical forms:
- Rhinocerebral: Most common; begins in sinuses, spreads to orbit and brain; black eschar on palate/turbinates is pathognomonic
- Pulmonary: Fever, hemoptysis, cavitation
- Cutaneous: After burns or trauma
Diagnosis:
- CT/MRI of sinuses/brain
- Biopsy with GMS or H&E stain: Wide aseptate hyphae with irregular branching at right angles (90°) - distinguishes from Aspergillus
- Culture (handle gently - sparsely septate hyphae fragment easily)
Treatment:
- First-line: Liposomal AmB 5-10 mg/kg/day
- Step-down: Isavuconazole or posaconazole after stabilization
- Surgery: Aggressive early surgical debridement is essential and life-saving
- Control underlying diabetes; reverse immunosuppression if possible
- Voriconazole has NO activity against Mucorales - prior voriconazole use is a risk factor for breakthrough mucormycosis
D. Pneumocystis jirovecii Pneumonia (PCP)
Note: Reclassified as a fungus (not a protozoan).
Risk factors: AIDS (CD4 <200), organ transplant, high-dose steroids, biologic agents, hematologic malignancy
Clinical features: Subacute onset of dyspnea, non-productive cough, fever; PaO2 lower than expected; LDH elevated
Diagnosis:
- Chest X-ray: Bilateral interstitial/perihilar infiltrates ("bat-wing" pattern); may be normal early
- HRCT: Ground-glass opacities
- BAL: PCP trophozoites/cysts identified by Giemsa, toluidine blue O, GMS stain, or direct immunofluorescence
- PCR on respiratory specimens: Highly sensitive in immunocompromised patients (recent systematic review PMID 38860786)
- β-D-glucan: Elevated (useful adjunct)
Treatment:
- First-line: TMP-SMX (trimethoprim-sulfamethoxazole) 15-20 mg/kg/day (TMP component) PO/IV × 21 days
- Adjunctive corticosteroids: If PaO2 <70 mmHg on room air or A-a gradient >35 mmHg
- Alternatives: Pentamidine IV; atovaquone (mild-moderate); clindamycin + primaquine
- Prophylaxis: TMP-SMX DS daily; alternatives = dapsone, atovaquone, aerosolized pentamidine
E. Cryptococcosis
Agent: Cryptococcus neoformans (AIDS/immunocompromised), C. gattii (can infect immunocompetent hosts)
Risk factors: AIDS (CD4 <100), organ transplant, high-dose steroids, hematologic malignancy
Clinical features: Subacute meningoencephalitis (headache, fever, confusion), pulmonary cryptococcosis, rarely skin lesions (molluscum-like in AIDS)
Diagnosis:
- CSF India ink: Budding yeasts with large capsule (polysaccharide)
- Cryptococcal antigen (CrAg): Serum or CSF - highly sensitive and specific; lateral flow assay available for low-resource settings
- CSF opening pressure: Often markedly elevated (>25 cm H2O)
- Culture on Sabouraud agar: Mucoid colonies
Treatment (CNS disease):
- Induction: AmB deoxycholate (0.7-1 mg/kg/day) OR liposomal AmB (3-4 mg/kg/day) + flucytosine 25 mg/kg qid × 2 weeks
- Consolidation: Fluconazole 400 mg/day × 8 weeks
- Maintenance/Suppression: Fluconazole 200 mg/day (lifelong in AIDS until immune reconstitution)
- Manage elevated ICP: Serial lumbar punctures or lumbar drain; elevated ICP is a major cause of early mortality
- Pulmonary (mild-moderate): Fluconazole alone
F. Endemic Mycoses (Dimorphic Fungi)
These dimorphic fungi grow as molds in the environment and convert to yeast forms in tissue at body temperature:
| Disease | Organism | Geography | Diagnosis | Treatment |
|---|---|---|---|---|
| Histoplasmosis | Histoplasma capsulatum | Ohio/Mississippi River valleys; bird/bat droppings | Urine/serum Histoplasma antigen; culture; narrow intracellular yeasts in macrophages | Mild: no treatment or itraconazole; Moderate-severe: AmB → itraconazole; Disseminated: itraconazole × 12 months |
| Coccidioidomycosis | Coccidioides immitis/posadasii | Southwestern US, Mexico | Serology (IgM precipitin, IgG CF); EIA; culture (BSL-3); large spherules on biopsy | Mild pulmonary: often self-limited; Disseminated/meningeal: fluconazole or itraconazole × years (lifelong for meningitis) |
| Blastomycosis | Blastomyces dermatitidis | North America (Great Lakes, Mississippi) | Broad-based budding yeast with thick wall on KOH/histology; antigen assay | Mild-moderate: itraconazole × 6 months; Severe/CNS: AmB → itraconazole |
| Paracoccidioidomycosis | Paracoccidioides brasiliensis | Latin America | "Pilot's wheel" multiply-budding yeast on histology | Itraconazole (first-line); TMP-SMX or amphotericin B for severe disease |
Part III: Antifungal Drug Classes - Summary
| Class | Mechanism | Key Agents | Activity |
|---|---|---|---|
| Polyenes | Bind ergosterol → membrane disruption | AmB deoxycholate, Liposomal AmB, ABLC | Broad spectrum: Candida, Aspergillus, Cryptococcus, Mucor, endemic fungi; lipid formulations reduce nephrotoxicity |
| Azoles | Inhibit CYP51 (lanosterol 14α-demethylase) → deplete ergosterol | Fluconazole, Itraconazole, Voriconazole, Posaconazole, Isavuconazole | Fluconazole: Candida/Cryptococcus; Voriconazole/Posaconazole: + Aspergillus; Posaconazole/Isavuconazole: + Mucor (posaconazole only) |
| Echinocandins | Inhibit β(1,3)-D-glucan synthase → disrupt cell wall | Caspofungin, Micafungin, Anidulafungin | Candida (fungicidal), Aspergillus (fungistatic); NO activity vs Cryptococcus, Mucor; first-line for invasive candidiasis |
| Pyrimidine analog | Inhibits DNA/RNA synthesis | Flucytosine (5-FC) | Candida, Cryptococcus; always combine with AmB to prevent resistance |
| Allylamines | Inhibit squalene epoxidase → deplete ergosterol | Terbinafine | Dermatophytes (fungicidal); limited yeast activity |
| Novel | Inhibits β-glucan (triterpenoid) | Ibrexafungerp | VVC; active against some azole-resistant Candida |
- Murray & Nadel's Respiratory Medicine, Table 57.1
Key Diagnostic Tools: At-a-Glance
| Test | Use |
|---|---|
| KOH prep | All superficial infections; hyphae in tinea, "spaghetti and meatballs" in tinea versicolor |
| Wood's lamp | Microsporum tinea capitis (green fluorescence) |
| Culture (SDA) | Speciation of dermatophytes; definitive for most fungi |
| PAS / GMS stain | Histopathology: fungi stain pink-red (PAS) or black (GMS) |
| β-D-glucan | Broad invasive fungal screening (Candida, Aspergillus, PCP); false negatives for Cryptococcus/Mucor |
| Galactomannan | Specific for Aspergillus; serum and BAL |
| CrAg (Cryptococcal antigen) | Highly sensitive/specific for Cryptococcosis |
| Histoplasma/Blastomyces antigen (urine/serum) | Endemic mycoses |
| Blood culture | Candidemia; only ~50% sensitive |
| India ink | Cryptococcal meningitis (CSF) |
| PCR | Increasingly used for PCP, Aspergillus, Candida; not fully standardized for all |
Recent evidence note: A 2024 systematic review (PMID 38860786, Clin Infect Dis) confirmed PCR on respiratory specimens is highly sensitive for PCP diagnosis in immunocompromised patients, supporting its use alongside or instead of traditional staining. A network meta-analysis (PMID 38583518, Clin Microbiol Infect, 2024) confirmed TMP-SMX as the most effective PCP prophylaxis in HIV. For Allergic Bronchopulmonary Aspergillosis (ABPA), a 2024 meta-analysis (PMID 38898129, Lung) supports the efficacy of biologic agents (anti-IL-4/IL-13, anti-IgE) in reducing exacerbations.
Summarize it
Fungal Infections: Summary
Classification
Mycoses are superficial (skin/hair/nails), subcutaneous (dermis/soft tissue), or deep/systemic (invasive, hematogenous).
Superficial Infections
| Infection | Cause | Diagnosis | Treatment |
|---|---|---|---|
| Tinea (capitis/corporis/cruris/pedis) | Dermatophytes (T. rubrum, T. tonsurans) | KOH prep (hyphae), culture | Topical azoles/terbinafine; oral terbinafine or itraconazole for extensive/scalp/nail disease |
| Onychomycosis | Dermatophytes | KOH, nail clipping culture | Terbinafine 250 mg/day × 3 months (first-line); itraconazole pulse therapy |
| Tinea versicolor | Malassezia furfur | KOH ("spaghetti & meatballs") | Selenium sulfide/ketoconazole shampoo; oral fluconazole/itraconazole for extensive disease |
| Mucocutaneous candidiasis | Candida spp. | Clinical, KOH, culture | Topical nystatin/clotrimazole (mild); oral fluconazole (moderate-severe/esophageal) |
Subcutaneous Infections
- Sporotrichosis: Itraconazole × 3-6 months; AmB for severe/CNS disease
- Eumycetoma (Madura foot): Itraconazole + surgery
- Chromoblastomycosis: Itraconazole ± cryotherapy
Invasive/Systemic Infections
| Infection | Key Diagnosis | First-line Treatment |
|---|---|---|
| Invasive Candidiasis | Blood culture, β-D-glucan, funduscopy | Echinocandin (caspofungin/micafungin); step-down to fluconazole |
| Invasive Aspergillosis | CT (halo sign), galactomannan, BAL culture | Voriconazole (or isavuconazole) |
| Mucormycosis | Biopsy (aseptate hyphae), CT sinuses | Liposomal AmB + aggressive surgery |
| Cryptococcal meningitis | CSF CrAg, India ink | AmB + flucytosine (induction) → fluconazole (consolidation/maintenance) |
| PCP | BAL, PCR, β-D-glucan | TMP-SMX × 21 days ± corticosteroids if PaO₂ <70 mmHg |
| Histoplasmosis | Urine/serum antigen | Itraconazole (mild); AmB → itraconazole (severe) |
| Coccidioidomycosis | Serology, spherules on biopsy | Fluconazole or itraconazole (often lifelong for meningitis) |
Antifungal Drug Classes
| Class | Agents | Targets |
|---|---|---|
| Polyenes | AmB (conventional + lipid) | Broad spectrum; Candida, Aspergillus, Mucor, Cryptococcus |
| Azoles | Fluconazole, Voriconazole, Posaconazole, Isavuconazole | Ergosterol synthesis; varies by agent |
| Echinocandins | Caspofungin, Micafungin, Anidulafungin | Candida/Aspergillus; no Cryptococcus/Mucor activity |
| Allylamines | Terbinafine | Dermatophytes (fungicidal) |
| Pyrimidine analog | Flucytosine | Only in combination (with AmB) to prevent resistance |
Key Diagnostic Pearls
- KOH prep - bedside test for all superficial infections
- β-D-glucan - broad invasive fungal screen (false negative for Cryptococcus and Mucor)
- Galactomannan - specific for Aspergillus
- Cryptococcal antigen (CrAg) - highly sensitive/specific for cryptococcosis
- Aseptate vs. septate hyphae on biopsy distinguishes Mucor (aseptate) from Aspergillus (septate, 45° branching)
- Voriconazole has no activity against Mucorales - prior use is a risk factor for breakthrough mucormycosis
This is a shared conversation. Sign in to Orris to start your own chat.