What is pleural effusion
Reading File
Finding Sources
Searching PubMed
"pleural effusion"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of pleural effusion, drawing from ROSEN's Emergency Medicine, Murray & Nadel's Textbook of Respiratory Medicine, and Grainger & Allison's Diagnostic Radiology.
Pleural Effusion
Definition
Pleural effusion is an abnormal collection of fluid in the pleural space - the potential space between the visceral and parietal pleura. Under normal conditions, a thin layer of fluid (~0.1-0.2 mL/kg body weight, about 5-15 mL total) maintains dynamic equilibrium, with approximately 1 L traversing the pleural space every 24 hours. An effusion develops when fluid influx exceeds efflux.
- ROSEN's Emergency Medicine, p. 988
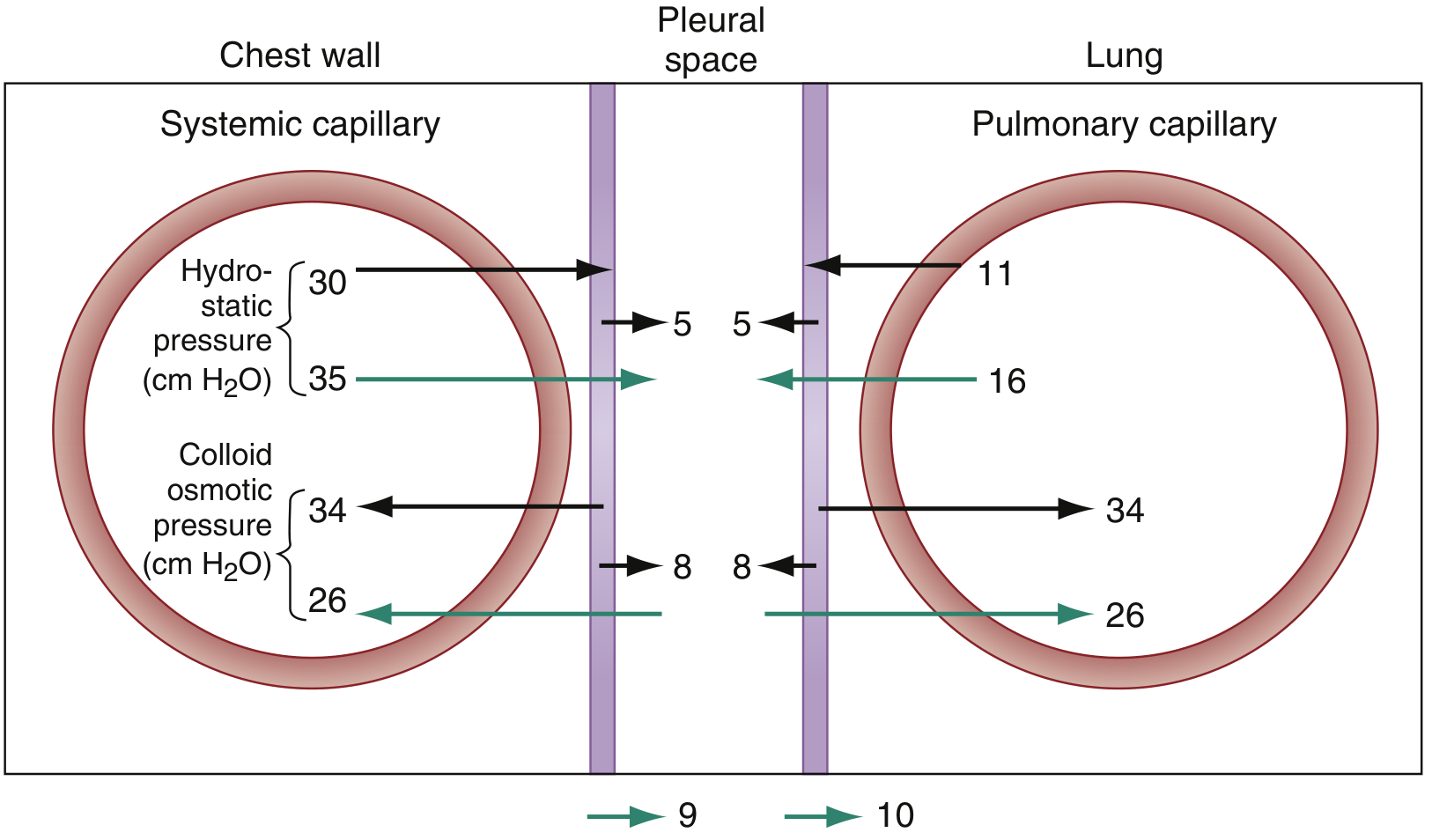
Anatomy and Physiology of Fluid Balance
Pleural fluid is produced from systemic capillaries at the parietal pleural surface and absorbed into pulmonary capillaries at the visceral pleural surface. The direction of flow is governed by the difference in hydrostatic pressures between the systemic and pulmonary circulations, with lymphatics also assisting drainage.
Causes
Pleural effusions are divided into transudates and exudates based on fluid composition.
Transudates (ultrafiltrates of plasma; low protein)
Caused by increased hydrostatic pressure or decreased oncotic pressure:
- Congestive heart failure (most common cause overall)
- Cirrhosis with ascites
- Nephrotic syndrome
- Hypoalbuminemia / severe malnutrition
- Myxedema
- Peritoneal dialysis
- Superior vena cava obstruction
- Pulmonary embolism (can be transudative or exudative)
Exudates (high protein; reflects intrinsic pleural abnormality)
Caused by inflammation, increased permeability, or lymphatic obstruction:
- Infections: bacterial pneumonia (parapneumonic effusion), TB, lung abscess, bronchiectasis, viral illness
- Malignancy: primary lung cancer, mesothelioma, metastases, lymphoma
- Connective tissue disease: rheumatoid arthritis, SLE
- Abdominal/GI disorders: pancreatitis, subphrenic abscess, esophageal rupture
- Miscellaneous: pulmonary infarction, uremia, chylothorax
Key terminology: A parapneumonic effusion is one associated with bacterial pneumonia or lung abscess. Empyema (pyothorax) means pus in the pleural space. A loculated effusion is fluid confined by adhesions between the visceral and parietal pleura.
- ROSEN's Emergency Medicine, p. 988-989
Pathophysiology
| Type | Mechanism | Common Causes |
|---|---|---|
| Transudate | High hydrostatic pressure OR low oncotic pressure | Heart failure, cirrhosis, nephrotic syndrome |
| Exudate | Pleural/pulmonary inflammation, increased capillary permeability, lymphatic obstruction | Pneumonia, malignancy, PE (often mixed) |
Massive effusions (>1.5-2 L) are usually malignant but can occur in heart failure and volume overload states. They can restrict respiratory movement, compress lung parenchyma, cause intrapulmonary shunting, and in extreme cases lead to tension hydrothorax with mediastinal shift and circulatory compromise.
Clinical Features
- Small effusions: typically asymptomatic
- Moderate-large effusions: dyspnea (usually does not develop until >500 mL fluid accumulates), cough
- Pleuritic pain: sharp chest pain worse with deep breathing; may radiate to ipsilateral shoulder (indicates pleural inflammation)
Physical examination findings:
- Diminished or absent breath sounds
- Dullness to percussion
- Decreased tactile fremitus
- Pleural friction rub (with pleuritis)
- Hemodynamic compromise with massive effusions
Diagnosis
Imaging
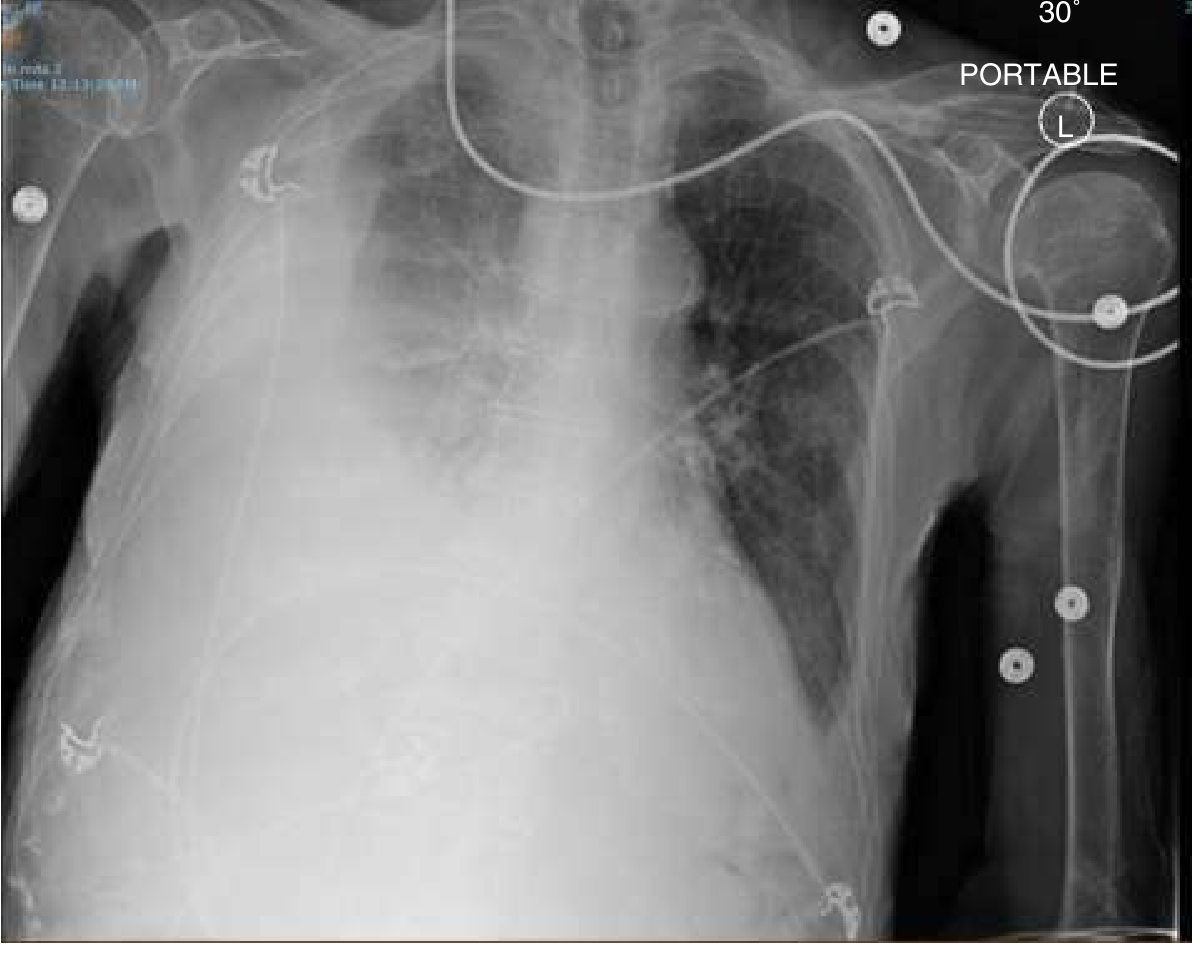
Chest X-ray:
- Requires ~200 mL to be visible on upright frontal view
- Classic finding: blunting of the costophrenic angle
- Larger effusions obscure the hemidiaphragm with an upward concave ("meniscus") appearance - fluid layers higher laterally than centrally
- Massive effusion can completely opacify the hemithorax
CT scan: Gold standard for small effusions; detects as little as 3-5 mL. Useful for distinguishing pleural from parenchymal disease and detecting underlying causes.
Ultrasound: Can detect as little as 50 mL. More sensitive than chest X-ray. Simple transudates appear hypoechoic; complex/exudative effusions may show heterogeneous echogenicity, septations, or loculations. Ultrasound guidance significantly reduces the risk of iatrogenic pneumothorax during thoracentesis.
Thoracentesis and Fluid Analysis
Most patients with a new pleural effusion should undergo diagnostic thoracentesis (can be deferred if an obvious cause like heart failure is clear).
Light's Criteria - the most widely accepted method for differentiating transudates from exudates. Fluid is an exudate if ANY ONE of the following is present:
| Criterion | Threshold |
|---|---|
| Pleural fluid protein / serum protein | > 0.5 |
| Pleural fluid LDH / serum LDH | > 0.6 |
| Pleural fluid LDH | > 2/3 of upper limit of normal serum LDH |
Additional markers:
-
pH < 7.3: suggests parapneumonic effusion, malignancy, rheumatoid effusion, TB, or systemic acidosis
-
Glucose, cell count, differential, culture, cytology ordered as clinically indicated
-
ROSEN's Emergency Medicine, p. 989-990
Management
Management depends entirely on the underlying cause:
| Cause | Treatment |
|---|---|
| Heart failure | Diuresis (IV if severe) |
| Parapneumonic/empyema | Antibiotics + early drainage; empyema benefits from surgical drainage |
| Malignant effusion | Therapeutic thoracentesis; recurrent cases require pleurodesis or indwelling pleural catheter |
| Hepatic hydrothorax | Sodium restriction + diuretics; refractory cases: TIPS, VATS repair of diaphragmatic defects, or indwelling catheter as bridge to transplant |
| Viral pleuritis | Supportive (self-limited) |
| TB effusion | Anti-TB chemotherapy |
- Conventional chest tube drainage is not recommended for hepatic hydrothorax due to risk of protein/electrolyte loss, infection, and renal failure.
- In ~20% of effusions, no definitive diagnosis is established; most resolve spontaneously.
Summary
Pleural effusion is a common clinical finding with a broad differential. The key diagnostic step is classifying the fluid as a transudate vs. exudate using Light's criteria, guided by clinical context. Ultrasound has become the standard for both diagnosis and procedure guidance. Treatment targets the underlying cause.
Sources: ROSEN's Emergency Medicine Concepts and Clinical Practice; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.