Atherosclerosis in detail for 5 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive 5-mark answer. Let me compile the full response.
Atherosclerosis
Definition
Atherosclerosis is a chronic inflammatory disease of large and medium-sized arteries characterized by intimal lesions called atheromas (atherosclerotic plaques) - raised lesions composed of a soft, friable lipid core (mainly cholesterol and cholesterol esters with necrotic debris) covered by a fibrous cap. It is the single leading cause of morbidity and mortality in the Western world, responsible for roughly half of all deaths.
- Robbins & Kumar Basic Pathology, p. 314
Epidemiology & Risk Factors
Risk factors are categorized as:
| Constitutional (Non-modifiable) | Modifiable |
|---|---|
| Genetic variation / family history | Hyperlipidemia (high LDL, low HDL) |
| Increasing age (incidence of MI rises 5x between ages 40-60) | Hypertension |
| Male sex (premenopausal women relatively protected) | Cigarette smoking |
| - | Diabetes mellitus |
| - | Inflammation (elevated CRP, homocysteine) |
| - | Obesity / sedentary lifestyle |
Risk factors are multiplicative: hyperlipidemia + hypertension + smoking increases MI risk ~7-fold.
Pathogenesis: "Response-to-Injury" Hypothesis
The central concept is that chronic endothelial injury initiates a cascade of events. The sequence involves:
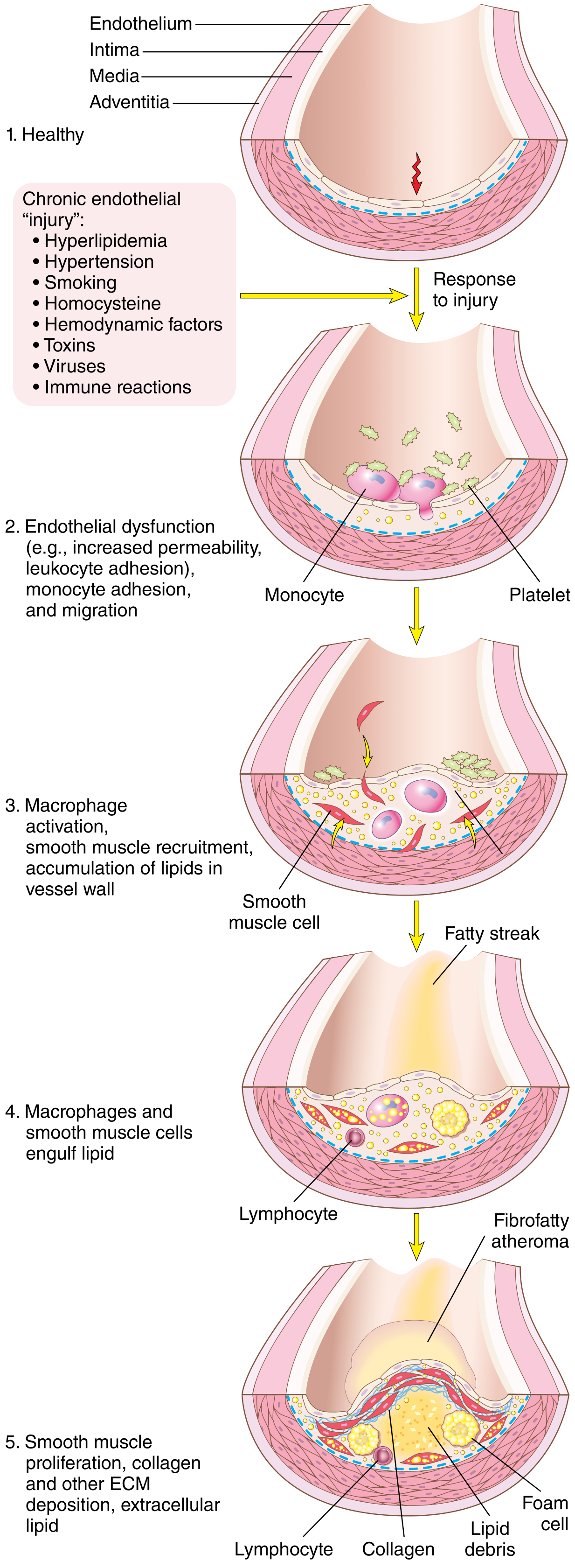
Step 1 - Endothelial Injury & Dysfunction
- Causes: hemodynamic turbulence (at branch points, ostia), hypercholesterolemia, smoking, hypertension, toxins, homocysteine
- Results in: increased permeability, upregulation of adhesion molecules (VCAM-1, ICAM-1), decreased nitric oxide production, altered gene expression
- Laminar flow normally induces the transcription factor KLF-2 which suppresses pro-inflammatory genes ("atheroprotective"); turbulent flow abolishes this effect
Step 2 - Lipoprotein Accumulation & Oxidation
- LDL enters the intima through the dysfunctional endothelium and is oxidized (ox-LDL)
- Oxidized LDL is pro-inflammatory: it stimulates endothelial cells to express more adhesion molecules and chemokines
- HDL has a protective role by reverse cholesterol transport
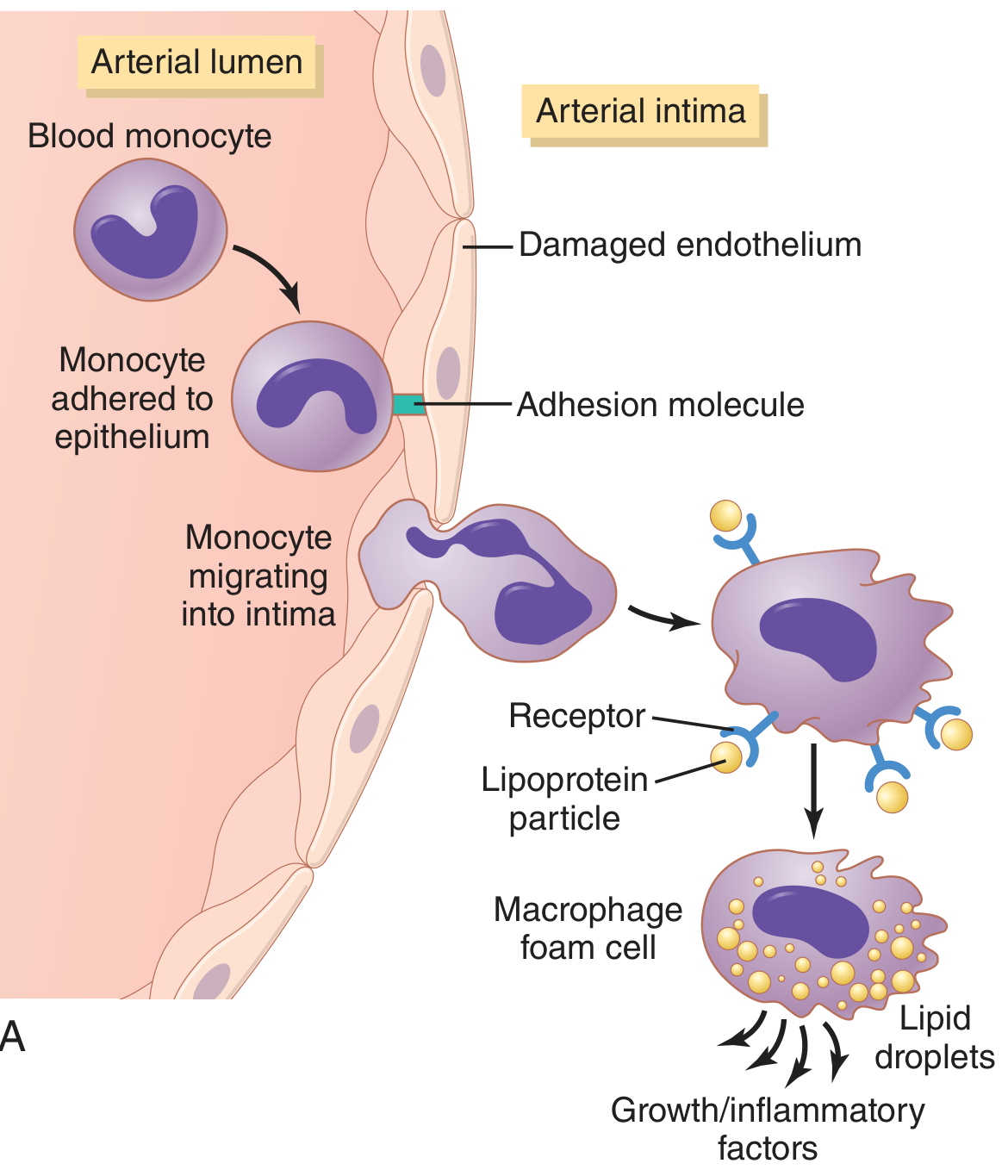
Step 3 - Monocyte Recruitment & Foam Cell Formation
- Monocytes adhere to the activated endothelium via adhesion molecules, then migrate into the intima
- In the intima, monocytes differentiate into macrophages, which ingest oxidized LDL via scavenger receptors (not downregulated like normal LDL receptors) → become foam cells (lipid-laden macrophages)
- Foam cells aggregate to form visible fatty streaks - the earliest grossly visible lesion (reversible, seen even in aortas of children)
Step 4 - Smooth Muscle Cell (SMC) Migration & Proliferation
- Activated macrophages, platelets, and endothelial cells release growth factors (PDGF, FGF, TGF-β) and cytokines
- SMCs migrate from the media into the intima, proliferate, and synthesize extracellular matrix (collagen, proteoglycans) → forming a neointima
- T lymphocytes also accumulate and sustain local inflammation
Step 5 - Advanced Plaque Formation
- Progressive accumulation of lipid, foam cells, SMCs, ECM, and T cells forms a full fibrous atheromatous plaque
- Central lipid core (necrotic debris from dead foam cells) is covered by a fibrous cap (collagen-rich, SMC-derived)
- Late stages: calcification of ECM and necrotic debris ("hardening of arteries")
Morphology of Atherosclerotic Plaques
Gross:
- Yellow-white raised intimal lesions
- Sites: aorta (esp. posterior abdominal), coronary arteries, popliteal arteries, carotid bifurcation, circle of Willis
Microscopic components:
- Fibrous cap - SMCs, collagen, proteoglycans, T cells
- Lipid core - cholesterol crystals, necrotic debris, foam cells, extracellular lipid
- Shoulder region - more cellular (macrophages, foam cells, T cells) - most vulnerable to rupture
- Neovascularization and calcification in advanced lesions
Consequences of Atherosclerosis
1. Atherosclerotic Stenosis
- Gradual plaque growth occludes the lumen
- Initially compensated by Glagov phenomenon (outward remodeling of the media)
- Critical stenosis occurs when the lumen cross-section is reduced by 70-75% - causes tissue ischemia and angina
- Result: chronic ischemic heart disease, peripheral vascular disease
2. Acute Plaque Change (Plaque Rupture / Erosion)
- The most dangerous complication
- Rupture of the fibrous cap (especially at the thin "shoulder" region) exposes the thrombogenic lipid core
- Triggers acute thrombosis → sudden occlusion → acute MI, stroke, sudden cardiac death
- Erosion (endothelial loss without rupture) can also trigger thrombosis
3. Aneurysm Formation
- Plaque thickens the intima, impeding diffusion from lumen to media
- Ischemia of the media weakens the arterial wall → aortic aneurysm (especially abdominal aorta)
4. Embolism
- Thrombus or atheromatous debris can embolize distally → embolic stroke, renal infarction, limb ischemia
Summary Table
| Feature | Details |
|---|---|
| Primary lesion | Atheroma (fibrous plaque) |
| Earliest lesion | Fatty streak (reversible) |
| Key cell | Macrophage foam cell |
| Central mechanism | Endothelial injury → lipid accumulation → inflammation → fibrosis |
| Key arteries affected | Aorta, coronary, carotid, popliteal |
| Main complications | MI, stroke, aneurysm, peripheral vascular disease |
| Critical stenosis threshold | 70-75% luminal cross-sectional area reduction |
Sources: Robbins & Kumar Basic Pathology (10e), p. 313-321; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 466-475; Guyton and Hall Textbook of Medical Physiology (14e), p. 851
This is a shared conversation. Sign in to Orris to start your own chat.